

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Peritoneal adhesions occur after 63%–97% of abdominal operations, and they are associated with significant morbidity and even mortality. Adhesions may reduce quality of life as a result of recurrent abdominal pain, poor oral intake, and increased healthcare costs [1234].
During rectal cancer surgery, diverting ileostomy may be necessary in selective patients with various risk factors such as low level of anastomosis, preoperative chemoradiotherapy, emergency operation, and a large amount of perioperative blood loss or transfusion [567]. Ileostomy reversal is usually performed 2–8 months after rectal cancer surgery [89], and during ileostomy reversal, the degree of peritoneal and intramuscular adhesion formation affects operative outcomes, including operation time, the length of the resected small bowel, and postoperative complications [101112].
Adhesion inhibitors have been developed to prevent peritoneal adhesions, especially in the intraabdominal space. Many studies have evaluated the effectiveness of adhesion inhibitors among patients who had undergone ileostomy procedures and who could be evaluated for the degree of adhesion formation at the time of ileostomy reversal [3131415]. In addition to intraperitoneal adhesions, adhesions between the ileostomy and the rectus abdominal muscle can affect the outcomes of reversal surgery. Severe adhesions between the ileostomy and the muscle may lead to longer operation time, longer bowel resection length, and increased surgical complications. Some surgeons theorize that anchoring sutures between the anterior sheath of the rectus abdominal muscle and the peritoneum, which minimize muscle exposure to the ileostomy, can reduce this type of adhesion and thus improve the surgical outcomes. However, other surgeons do not perform anchoring sutures, with the thought that additional sutures may result in more adhesions. Although anchoring sutures can be considered a simple, low-risk, and inexpensive method for reducing adhesion formation around ileostomy sites, there are no published reports on the effects of anchoring sutures in this regard.
This study aimed to evaluate the effects of anchoring sutures on the degree of adhesion formation between the ileostomy and the intramuscular and peritoneal space after sphincter-saving rectal cancer surgery. Operative and postoperative outcomes at the time of ileostomy reversal were also investigated.
Go to : 
METHODS
Patients
This study included rectal cancer patients who underwent curative-intent surgery with diverting ileostomy at Asan Medical Center, Seoul, Korea, between January 2013 and December 2017. Patients who received minimal-invasive surgery including laparoscopic and robotic surgery were included. Patients were excluded if they were younger than 20 years or older than 80 years, had a history of abdominal surgery, had other malignancies, had inflammatory bowel disease during the study period, or received open surgery. The study protocol was approved by the Institutional Review Board of Asan Medical Center (No. 2018–0609), and this study was performed in accordance with the Declaration of Helsinki. The requirement for informed consent was waived because of the retrospective nature of the study.
Decision of ileostomy site was made by surgeon preference. Surgeons who perform more robotic surgeries tend to locate the stoma in the left lower quadrant, but this is not a fixed rule. When patients have a short small bowel mesentery and thus left lower quadrant is not suitable for ileostomy, stoma was made at the right lower quadrant. The diverting ileostomy was made either with anchoring sutures or without anchoring sutures, depending on the operator’s preference. The anchoring sutures were performed by suturing the anterior sheath of the rectus abdominal muscle and the peritoneum to minimize exposure of the muscle tissue to the ileostomy (Fig. 1). Patients in the anchoring group (AG) underwent this anchoring suture at 4 quadrants (superior, inferior, medial, and lateral direction) during diverting ileostomy formation. The suture material was Lactomer glycolide/lactide copolymer coated with caprolactone and calcium stearoyl lactylate (Polysorb 3–0, Covidien, Medtronic, Minneapolis, MN, USA) or Silk (Black silk 3–0, Ethicon, Johnson and Johnson, Somerville, NJ, USA). The non-anchoring group (NAG) did not receive any kind of manipulation between the ileostomy and the rectus abdominal muscle nor the peritoneal space. The timing of ileostomy reversal varied from 3 to 8 postoperative months, depending on whether the patients received adjuvant chemotherapy or not. All patients underwent defecography to check the anastomosis consistency. For stoma restoration, 2 types of anastomosis methods (staples or handsewn) were used according to the preference of the operator. Staple anastomoses were performed as functional end-to-end anastomoses using PROXIMATE Linear Cutters TLC 75 (BLUE, Ethicon), and hand-sewn anastomoses were performed by primary repair of the stoma opening using Polysorb 3–0.
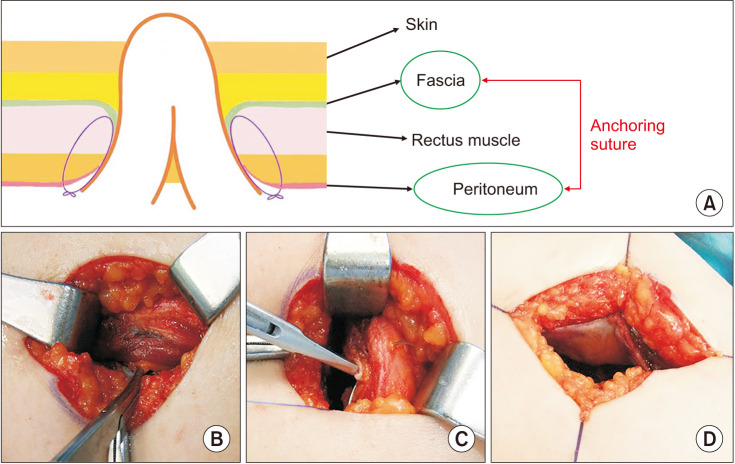 | Fig. 1Anchoring sutures are placed to pull together the anterior fascia of the abdominal wall and the peritoneal layer. This prevents the rectus muscles from directly adhering to the small bowel serosa. (A) Schematic drawing of the anchoring suture procedure. (B) Photo showing peritoneum (indicated by a forcep), rectus muscle, and anterior fascia. (C) Fixation of peritoneum and anterior fascia with vicryl suture. (D) Four-point anchoring suture, minimizing the contact area between the small bowel and abdominal wall.
|
The following variables from the medical records of the study cohort during the ileostomy restoration were collected prospectively: clinical information (age, sex, body mass index [BMI], past medical history, preoperative chemoradiotherapy, adjuvant treatment, time interval between the date of formation and reversal of ileostomy, American Society of Anesthesiologists physical status classification, ileostomy location, ileostomy group [AG vs. NAG], adhesion variables, postoperative complication, and hospital stay), pathological findings, and laboratory findings.
The adhesion variables used to evaluate the efficacy of the anchoring sutures were as follows: length of the resected small bowel, the operation time between the skin incision and the intraperitoneal approach, and peritoneal adhesion index (PAI) score. The degree of adhesion formation was scored using the PAI, which has been used in previous studies on adhesion [314151617]. PAI scores were evaluated in each of the 4 quadrants around the ileostomy; superior (12 o’clock direction), medial (3 o’clock direction in the right lower quadrant and 9 o’clock direction in the left lower quadrant), inferior (6 o’clock direction), and lateral (9 o’clock direction in the right lower quadrant and 3 o’clock direction in the left lower quadrant). The PAI was graded as follows: 0, no adhesions; 1, avascular adhesions needing blunt dissection; 2, strong and limited vascular adhesions needing sharp dissection; 3, dense adhesions, vascularized, only separable with sharp dissection, unavoidable of damage [314151617]. Two expert surgeons and 1 surgical assistant who were accustomed to PAI assessment determined the PAI scores. The sum of individual PAI scores was also evaluated, as total PAI scores ranged from 0 to 12, with 12 representing the highest degree of adhesion formation.
Statistical analysis
Categorical variables were compared using the chi-square test, and continuous variables were compared using the unpaired Student t-test or the Mann-Whitney U-test. For multivariable analyses, continuous variables were converted to categorical variables according to the mean value or general acceptance. Variables with P-values of <0.1 in the univariable analyses and clinically relevant factors were included in the multivariable analysis. Multivariable analysis using binary logistic regression was used to assess the risk factors for unfavorable PAI scores and operation times. The Hosmer-Lemeshow statistic was calculated to check the appropriateness of the logistic regression model. The cut-off value for the PAI score was 6, and patients were grouped into 2 groups accordingly. The cut-off value for operation time was 51.77 minutes, the mean value. Statistical significance was defined as P < 0.05, and all statistical analyses were performed using IBM SPSS Statistics for Windows, ver. 25 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
Clinical characteristics
A total of 90 patients were included in this study, with 60 and 30 patients in the AG and NAG, respectively. The median age of the patients was 62.66 ± 12.86 years old. Among the variables, only the location of diverting ileostomy was different between the AG and the NAG, with a significantly higher proportion of patients in the AG having undergone ileostomy in the left lower quadrant (38.3% vs. 3.3%, P = 0.001). Other clinical characteristics were not statically different between the 2 groups including sex distribution, also BMI was not significantly different between the 2 groups (mean, 23.78 ± 3.15 vs. 23.67 ± 2.90; P = 0.870) (Table 1).
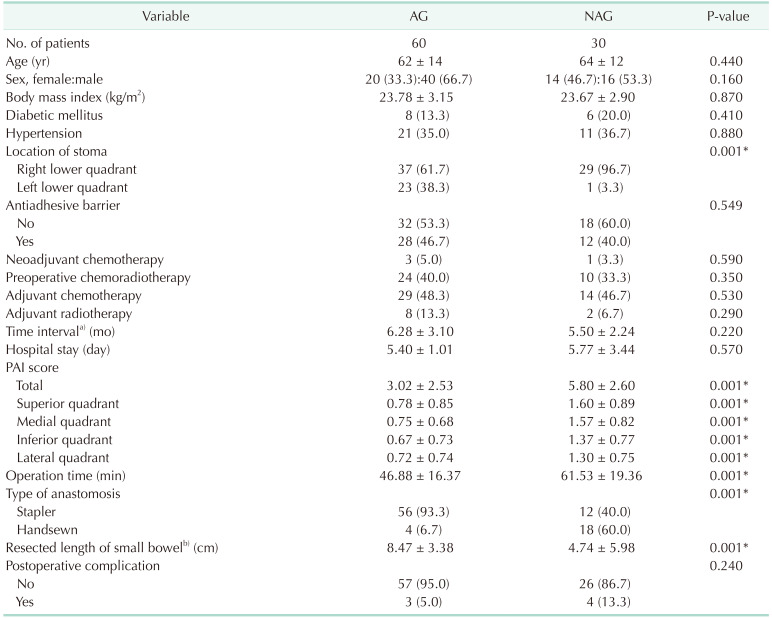
Table 1
Clinicopathological characteristics and postoperative outcomes
Values are presented as number only, mean ± standard deviation, or number (%).
AG, anchoring group; NAG, non-anchoring group; PAI, peritoneal adhesion index.
a)Time interval between the formation of diverting ileostomy and reversal. b)The length of the resected small bowel after reversal whether resection or not.
*P < 0.05.
![]()
Postoperative outcomes
The mean operation time in the AG was significantly shorter than that of the NAG (46.88 ± 16.37 minutes vs. 61.53 ± 19.36 minutes, P = 0.001). The AG was significantly more frequently associated with stapled anastomoses (93.3% vs. 40.0%, P = 0.001) and a longer mean length of resected small bowel (8.47 ± 3.38 cm vs. 4.74 ± 5.98 cm, P = 0.001), compared with the NAG. The PAI scores in the AG were significantly lower than those in the NAG in terms of both the individual quadrants (superior, medial, inferior, and lateral) and the total scores (superior: 0.78 ± 0.85 vs. 1.60 ± 0.89, P = 0.001; medial: 0.75 ± 0.68 vs. 1.57 ± 0.82, P = 0.001; inferior: 0.67 ± 0.73 vs. 1.37 ± 0.77, P = 0.001; lateral: 0.72 ± 0.74 vs. 1.30 ± 0.75, P = 0.001; and total score: 3.02 ± 2.53 vs. 5.80 ± 2.60, P = 0.001) (Table 1).
There was no significant difference in stoma-related complications after ileostomy formation between the AG and NAG. The AG showed 1 case of prolapse (1.7%), 2 hernias (3.3%), 5 skin erosion (8.3%), and the NAG showed 2 hernias (6.7%), and 4 skin erosion (13.3%). In all, AG presented 8 patients with stoma-related complications (13.3%) and NAG presented 6 patients with complications (20.0%) (P = 0.411).
The NAG had a higher postoperative complication rate (4 patients, 13.3%) compared to the AG (3 patients, 5.0%) but was not statistically significant (P = 0.164). Two patients experienced postoperative wound infection, and 1 patient experienced both wound infection and postoperative ileus in the AG. In the NAG, 2 patients experienced wound infection, and 2 patients experienced postoperative ileus.
Risk factors associated with peritoneal adhesion index score, length of small bowel resection, and operation time
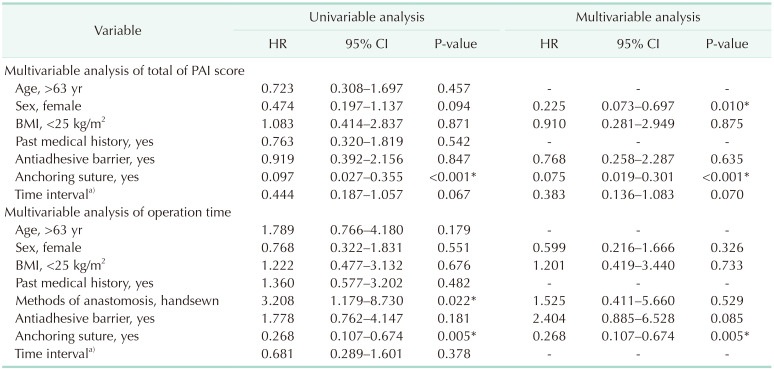
On multivariable analysis using binary logistic regression, female sex (hazard ratio [HR], 0.225; 95% confidence interval [CI], 0.073–0.697; P = 0.010) and the presence of anchoring sutures (HR, 0.075; 95% CI, 0.019–0.301; P ≤ 0.001) were significantly associated with low PAI scores (<6). Also, anchoring sutures were significantly associated with shorter operation times (HR, 0.268; 95% CI, 0.107–0.674; P = 0.005) (Table 2). According to the multivariable analysis, only handsewn anastomosis was significantly associated with the length of small bowel resection (HR, 0.205; 95% CI, 0.071–0.592; P = 0.003). Multivariable analysis including age, sex, BMI, past medical history, anchoring suture, time interval, and stoma site presented no statistical significance of stoma site to total PAI score (HR, 0.772; 95% CI, 0.228–2.618; P = 0.678) and operation time (HR, 1.690; 95% CI, 0.501–5.704; P = 0.398).
On subgroup analysis for sex distribution muscle thickness was significantly lower among females than males (1.28 ± 0.3 cm vs. 1.06 ± 0.24 cm, P = 0.038). More males had high total PAI scores (total score of >7, 67.9%) compared to females (50.0%); but it was not statistically significant. Operation time was comparable between males and females with a mean operation time of 51.46 ± 18.0 minutes and 52.26 ± 19.9 minutes, respectively.
Go to :
DISCUSSION
This study demonstrated that, compared with ileostomy without anchoring sutures, anchoring suture placement was associated with significantly lower mean total PAI score and mean operation times. It can be hypothesized that anchoring sutures can reduce adhesion formation by minimizing exposure of the rectus abdominal muscle to the ileostomy, preventing fibrotic connections between the small bowel and muscle tissue during healing. Contrary to concerns that adhesion formation could be facilitated by anchoring suture placement, simple anchoring sutures reduced the degree of adhesion formation between the peritoneum and muscle, resulting in significantly improved outcomes in terms of PAI scores and operation times. The method of anchoring using silk is quick, safe, and cost-effective, unlike many expensive commercial adhesion inhibitors.
The present study used the PAI scores to quantify the degree of adhesions between the ileostomy and the rectus muscles. The PAI score was originally designed for evaluating the degree of adhesion formation in the abdominal cavity [314151617]. It uses an easily accessible numerical scale and correlates it with the degree of adhesion formation. Although the biologic process between intraperitoneal adhesions and adhesions between the ileostomy and the rectus muscle can be different, the adhesions themselves have a similar effect in a clinical setting, which is, worsening operative or postoperative outcomes. Furthermore, when performing ileostomy reversal, the surgeon enters the intraperitoneal cavity through ileostomy-muscle adhesions, extending into the peritoneal cavity. Therefore, the numerical grading used for the PAI scoring system could be adopted in the present study to evaluate clinical outcomes. The AG had significantly lower mean scores in each of the 4 quadrants, as well as in terms of the total PAI score, compared with the NAG. This is evidence that anchoring sutures between the anterior rectus sheath and peritoneum minimize the area wherein the ileostomy comes in contact with the rectus abdominal muscle in all 4 directions around the ileostomy.
According to the multivariable analysis, the mean PAI score among females was significantly lower than that among males (HR, 0.225; 95% CI, 0.073–0.697; P = 0.010). It remains unclear whether or not one sex is more prone to developing adhesions than the other. One study reported a higher incidence of adhesions among male patients [14], but others have failed to identify any significant differences in postoperative adhesion development between males and females [18]. Recently, a defective fibrinolytic system has been reported to be intimately involved in or actually responsible for the development of adhesions [19], and differences in fibrinolytic capacity and fibrinogen levels between males and females have also been reported [2021]. Furthermore, another study found that males exhibit an enhanced stress-induced hemorheological response compared with age-matched females [22]. These studies have suggested the possibility that sex could be a predisposing factor for the development of postoperative adhesions. Another possible explanation of the sex difference in the present study is the difference in rectus muscle volume between the sexes. In the present study, adhesions occurred between 2 tissue planes: the serosal side of the small intestine and rectus muscle. It can be deduced that females have smaller rectus abdominal muscle areas around the ileostomy than males. Accordingly, in the subgroup analysis for evaluating sex differences in the rectus abdominal muscle mass around the ileostomy, muscle thickness was significantly lower among females than males (1.28 ± 0.3 cm vs. 1.06 ± 0.24 cm, P = 0.038).
The length of the small bowel resection in the AG was significantly longer than that in the NAG (mean length, 8.47 cm vs. 4.74 cm; P = 0.001). Although this result seems paradoxical as the AG had a lower PAI score and shorter operation time, it could be associated with the method of anastomosis rather than the severity of adhesions. There was a close association between the length of the resected small bowel and the method of anastomosis (affected by the operator’s preference; HR, 0.205; 95% CI, 0.071–0.592; P = 0.003). In line with previous literatures, there was no difference between the method of anastomosis (stapled vs. manual) regarding safety and risks, such as anastomotic leakage, and the surgeon could select the preferred anastomosis method [23].
The mean operation time of the AG was significantly shorter than that of the NAG (46.88 minutes vs. 61.53 minutes, P = 0.001). The shorter operation times in AG could have resulted from the lower degree of adhesion formation, as anchoring sutures were strongly associated with lower PAI scores (Table 2). However, considering that the AG had more stapled anastomoses than the NAG, the shorter operation time in the AG could be confounded by the anastomosis method, although the multivariable analysis showed no significant association between stapling method and operation time. To accurately analyze the effect of anchoring sutures on the operation times associated with adhesions, operation times should be measured as the interval from the skin incision to when the abdominal wall and ileostomy are completely separated. The present study had some limitations, such as the limited number of patients in the comparator groups and limitations related to the nature of the nonrandom assignment for the AG or NAG. Classification of patients into the AG or NAG proceeded according to the operators’ preference, and this could have affected the study results. As previously mentioned, the length of small bowel resection and the operation times were affected by the method of anastomosis, which was also decided according to the surgeon’s preference.
Anchoring suture placement during the raising of diverting ileostomies for patients who have undergone sphincter-saving surgery for rectal cancer decreased the severity of adhesions between the abdominal wall and the ileostomy sites, shortening operation times. In conclusion, anchoring sutures can be easily and safely applied to patients to facilitate improved outcomes and favorable surgical conditions for the subsequent ileostomy reversal.
Go to :
 XML Download
XML Download