

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hyaluronic acid (HA) is a biopolymer found in the human body and a component of the extracellular matrix (ECM), a type of glycosaminoglycan that is extensively distributed across the skin, muscle, cartilage, and blood vessels [1]. Because HA plays diverse roles in preserving moisture, maintaining the extracellular space, controlling osmotic pressure, and lubricating synovial joints, HA is used in various applications such as cosmetics, joint injections, and ophthalmic drugs [23]. Moreover, HA supports tissue regeneration and wound healing by promoting cell proliferation and migration during wound healing [4], which led to the launch of HA-related products, such as antiadhesive and wound dressing agents [56]. Conventional products include liquefied forms with HA concentrations (~2%) diluted using purified water [7]; however, they allow the products to easily deviate from the wound area, even following early application. Therefore, challenges remain to be addressed in areas of HA application following various surgical procedures.
Hemorrhoids, defined as enlarged areas of vascular tissue at the top of the anal canal, are common gastrointestinal disorders in Western countries [8]. In Korea, annually, approximately 170,000 patients undergo a surgical procedure for hemorrhoids, making it the second most common type of surgery in the country [9]. Conservative approaches are recommended for patients with low-grade disease. If medical management is ineffective after 6–8 weeks, subsequent treatment should be considered, from office-based therapies to excisional hemorrhoidectomy. Postoperative pain is the most common complication of excisional hemorrhoidectomy [10]. Multiple drugs are applied directly to the wound area to relieve pain in the perianal area and promote wound recovery [1112131415161718]. Previously, the drugs applied for wounds following hemorrhoidectomy mostly came in the form of a gel or ointment, and because of the properties of the ingredients, they easily deviated from the application area, resulting in decreased clinical utility, durability, and protective effects at the surgical site.
In this study, we aimed to elucidate the effects of HA application on perianal wound healing in a rat wound model.
Go to : 
METHODS
Animals and groups
This study was approved by the local ethics of Animal Experiments Committee at Seoul National University Bundang Hospital in Seongnam, Korea (No. BA1811–260/080–01, BA1904-269/019–01). We used 63 female, 8-week-old Sprague-Dawley rats (weight, ~180 to 200 g), including 15 rats in the pilot study and the rest in the present study. The rats were housed under the following conditions: temperature, 21°C–22°C; humidity, 40%–60%; and 12-hour light/12-hour dark regime. All methods were performed in accordance with the relevant guidelines and institutional regulations.
Animal experiments
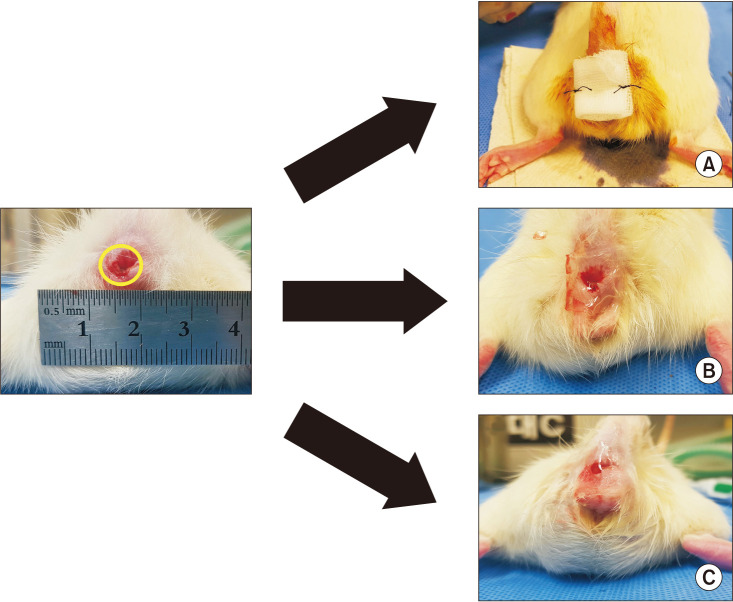
The HA gel and film were prepared according to previously described methods by Kweon et al. [19]. Varying concentrations of the solution of HA with molecular weight of ~0.8–1.2 MDa (Jinwoo Bio, Seoul, Korea) were prepared using a 10% ethanol solution (to prevent microbial contamination and remove air bubbles with ease and to reduce the time needed for drying), and then using the solvent casting method, varying concentrations of the film were prepared. The film conditions and wound size were designed according to the results of a pilot study involving 15 rats. According to the pilot study, a 3% HA concentration film was selected for adequate gelation rate, film thickness, tensile strength, and moisture content. All surgical procedures were performed under general anesthesia using isoflurane, and all efforts were made to minimize suffering. After the rats were anesthetized, a wound was made in the perianal area using a 4-mm biopsy punch (Kai Industries, Tokyo, Japan). The rats with perianal wounds were divided randomly into 3 groups: control (n = 16), HA film (n = 16), and HA gel (n = 16). In the control group only a simple gauze dressing was applied after wound formation, whereas in the HA film and HA gel groups, a topical film or gel was applied, respectively, on the wound area (Fig. 1). The HA film or HA gel was not reapplied after the intraoperative dressing.
Evaluation of perianal wound
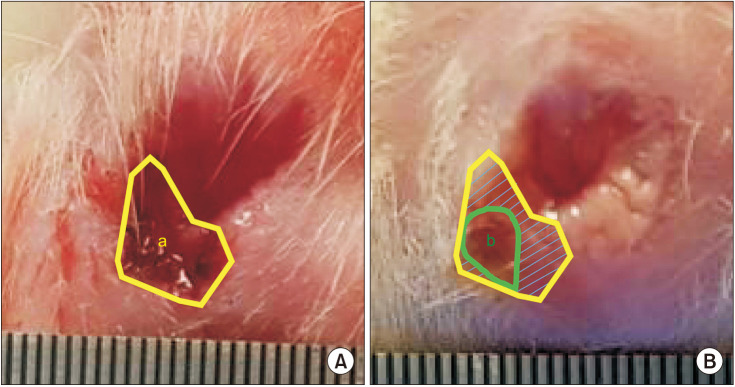
Complete wound healing according to gross visual examination was defined as complete epithelialization, loss of hemorrhage, loss of ulcer, and discontinuation of inflammatory discharge. The recovery of inflammatory lesions was determined based on the time of the disappearance of the redness and inflammatory discharge. To measure the size of the wound area, wound images were obtained on postoperative days 0, 2, 6, 9, 11, 14, and 16, using ImageJ software (National Institutes of Health, Bethesda, MD, USA). To estimate the wound healing rate, wound size on postoperative day 0 was compared with the size on each subsequent postoperative day to obtain the rate of reduction in wound size [2021] according to the following equation: wound healing rate on day x (%) = (1 – day x wound area/day 0 wound area) × 100 (Fig. 2).
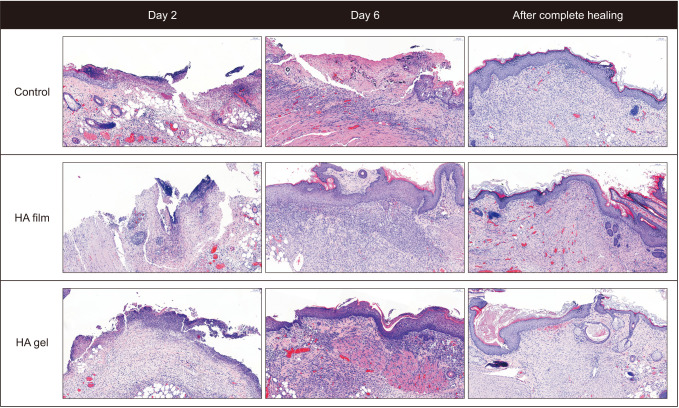
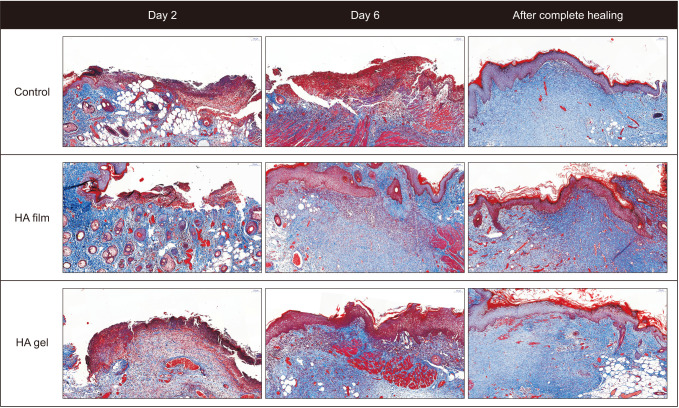
For histopathologic analysis of wound healing, 3 rats in each group were euthanized on days 2 and 6 and on the day of complete wound healing. For sampling of perianal tissue, tissues were fixed in 10% formalin, embedded in paraffin, sectioned at 4 µm, and stained with H&E and Masson's trichrome (MT). The remaining rats were euthanized after complete healing was confirmed based on the visual criteria.
Statistical analysis
Because the variables associated with wound healing rate according to the experimental day did not satisfy the normality assumption, statistical analyses were performed using a generalized estimation equation that applies a general linear model to consider within-subject correlation in data of clusters or repeated measures. For the day of complete healing, the variables did not satisfy the normality assumption; therefore, we used a distribution-free method for statistical analysis. To compare 3 independent groups, we used the Kruskal-Wallis test to verify significant differences between groups (P < 0.05). To examine intergroup differences, post hoc analyses were performed using Bonferroni correction. All statistical analyses were performed using IBM SPSS Statistics ver. 25.0 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
Gross visual examination of perianal wound
The surgical procedure was well tolerated in all groups. Based on the visual criteria of complete wound healing, loss of bleeding was observed in the HA film group on day 6 and in both the HA gel and the control groups on day 9. The loss of ulceration was observed on day 9 in both the HA film and HA gel groups and on day 11 in the control group. The recovery of inflammatory lesions was determined based on the time of disappearance of redness and inflammatory discharge, with the fastest recovery observed in the HA film group on day 11 as compared with the control group on day 16 (Fig. 3). The mean time required for gross complete healing was 11.6 ± 1.5 days in the HA film group, 11.9 ± 1.3 days in the HA gel group, and 13.8 1.7 days in the control group (P = 0.010). The mean percentage of wound healing area on day 11 was 80.2% ± 10.8% in the HA film group compared to 61.9% ± 11.2% in the HA gel group and 53.2% and ± 12.7% in the control group (P < 0.001). Fig. 4 shows the wound healing rate for each group, revealing that the HA film group showed a rate that was 1.8% per day faster than that of the control group (P < 0.001).
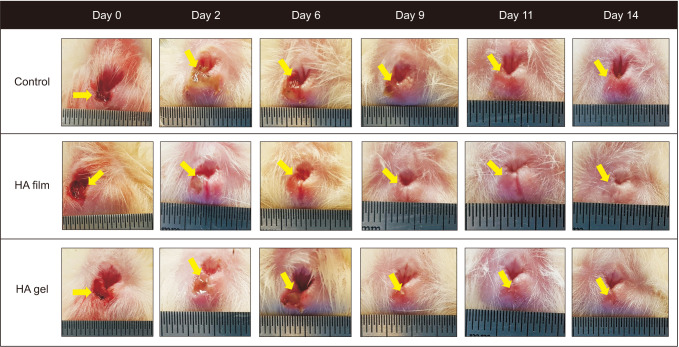 | Fig. 3Comparison based on gross visualization of complete wound healing. Hyaluronic acid (HA) film and HA gel groups showed complete wound healing on day 14 (yellow arrows indicate the wound or the scar).
|
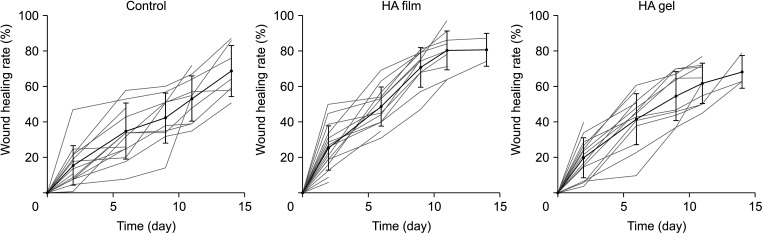 | Fig. 4The wound healing rate in each group per day up to day 14. The wound healing rate on day 11 was 53.2% in the control group, 80.2% in the hyaluronic acid (HA) film group, and 61.9% in the HA gel group. The dark line shows the mean rate per day with standard deviation, and the lighter lines show the rate per individual in each group.
|
Histopathologic evaluation
Figs. 5 and 6 show representative H&E- and MT-stained images from the control, HA film, and HA gel groups. On day 2, wound-induced epithelial defects and neutrophilic exudate were observed in all 3 groups, and neutrophil-dominant inflammation was observed in the dermis and subcutaneous tissue. On day 6, the types of inflammatory cells shifted from neutrophils to lymphocytes and monocytes in the HA film and HA gel groups, and reepithelialization was observed. In addition, MT staining revealed fibroblast proliferation and advancement of fibrosis indicating tissue repair. These phenomena were observed in all rats in the HA film group, although they were observed in 1 of 3 rats in the HA gel group, indicating a higher rate of wound healing in the HA film group. Subsequent examination after complete wound healing revealed fibrosis accompanied by reepithelialization and fibroblast proliferation in all animals in all 3 groups; however, the level of fibroblast and inflammatory cell infiltration was decreased in the HA film group relative to that in the HA gel and control groups.
Go to :
DISCUSSION
We evaluated the efficacy of different types of HA application on perianal wounds in a rat model. To the best of our knowledge, this is the first study to show that HA in film form applied to perianal wounds improved the wound healing rate. Wound healing is generally a series of processes involving hemostasis, inflammation, proliferation, and remodeling. During each phase, HA plays diverse roles depending on its molecular weight [22]. High-molecular-weight HA (HMW-HA) suppresses inflammation and the immune response while providing cellular protection, whereas low-molecular-weight HA induces inflammation and promotes neovascularization as well as differentiation and migration of epithelial cells and tubule formation [6]. During wound healing after skin damage, changes in the ECM, including reinforced growth factor signaling with excessive proliferation, increased collagen levels, and decreased HA deposition, lead to keloid formation. The application of HMW-HA during this process aids in scar prevention and treatment [23]. Based on these characteristics, HA promotes rapid wound healing following topical application to the wound area.
Traditional products associated with HA were liquefied, for example, into a gel form, making it is easy to apply but also easy to deviate from the target area. Therefore, HA film was prepared to resolve this limitation. HA film transforms into gels after adhering to the wound area and has excellent adhesiveness, allowing more absorption than the gel form. In the microbiological safety test, the HA film outperformed the HA gel, and it was easy to store and apply to the surgical environment.
Excisional hemorrhoidectomy is a common surgical procedure that is painful, resulting in low quality of life scores in the short term [1024]. The origin of the pain is skin irritation in the sensitive perianal area and spasm of the anal sphincter. In addition, delayed wound healing might lead to prolonged wound pain, causing patients to have longer hospital stays and a lower quality of life after surgery. Many medical agents have been developed for direct application to the surgical site to alleviate pain with early recovery of perianal wounds; however, there are currently no widely used drugs showing sufficient efficacy [2526]. Previously applied medications, mostly produced as gels or ointments that easily deviate from the area of the application site, resulted in low utility and durability.
In the present study using a rat model, a film form of HA was used to maintain adherence to perianal wounds. We found minimal differences in the mean time for complete gross visual healing between HA film and gel application on the perianal wound; however, the decrease in scar size during wound healing was substantially faster in the HA film group than in the HA gel group. HA film showed better adherence to the wound area than HA gel, and continuous HA exposure promoted faster wound healing than that of HA gel. Faster healing of the perianal wound might be associated with relief from associated perianal pain and improvement in the quality of life of humans following anal surgery in the short term, which was not measured in this study.
This study had several limitations. First, the physiological function of the anus of rats is not the same as that of humans. This is a preclinical study of a rat model of the efficacy of HA film in wound healing. Further study in human beings for the application of HA films on perianal wounds is needed. Second, HA film may have limitations in its use due to the risk of fecal contamination. Third, the dressing was applied immediately after surgery. It is uncertain if just 1 application of HA film would result in a difference in the rate of wound healing. However, HA application resulted in faster wound healing than occurred in the control group, and HA film exposed HA to the surgical site for a longer period than did HA gel. The efficacy of repeated use of the HA film on perianal wounds is needed in the future.
In conclusion, topical application of HA film to perianal wounds improved the wound healing rate in a rat model. These results suggest a potential benefit of using HA film as a therapeutic agent for promoting wound healing, thereby reducing wound recovery time and the associated pain following anal surgery such as hemorrhoidectomy in humans. Further clinical studies are required.
Go to :
 XML Download
XML Download