

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Successful pancreas transplantation can establish consistent euglycemia and reduce mortality in patients with diabetes [1,2,3,4]. Introduction of immunosuppressants such as tacrolimus, mycophenolate mofetil, alemtuzumab, and rabbit anti-thymocyte globulin resulted in the decrease of acute rejection rates and the achievement of long-term graft survival [5,6,7,8,9,10,11,12]. It has also been reported that pancreas transplantation can achieve metabolic improvements, and in addition to long-term glycemic control, lipid metabolism is also improved following pancreas transplantation [13,14]. However, deterioration of β cell function and insulin sensitivity was detected during long-term follow-ups after pancreas transplantation even when glucose, hemoglobin A1c (HbA1c), and C-peptide levels were within the normal range [2,15,16,17]. Therefore, a new strategy is needed to prevent the deterioration of β cell function and insulin sensitivity after pancreas transplantation.
Dipeptidyl peptidase-4 (DPP-4) inhibitors are widely used antidiabetic drugs that mainly act through the inhibition of the rapid degradation of incretin hormones, such as glucagon-like peptide (GLP)-1 and gastric inhibitory polypeptide that facilitate insulin secretion and suppress glucagon secretion [18]. In addition to their glucose-lowering activities, DPP-4 inhibitors also confer beneficial effects on inflammation, cardiovascular and hepatic health, and the central nervous system [19]. Yet, it is unknown whether DPP-4 inhibitors can improve β cell function and insulin sensitivity after pancreas transplantation. The purpose of this study was to evaluate the effects of the use of DPP-4 inhibitors on β cell function and insulin sensitivity after pancreas transplantation.
Go to : 
METHODS
Patients, classification, and metabolic variables
This was a retrospective cohort study on the prospectively collected data in the electrical medical records of Asan Medical Center in Seoul, Korea. This study was approved by the Institutional Review Board of Asan Medical Center (No. 2015-0541). Written informed consent was obtained from all recipients. Among 372 recipients who underwent pancreas transplantation between January 2000 and June 2018 at our center, we excluded those with early graft failures (n = 6), early mortalities (n = 3), history of treatment with DPP-4 inhibitors before pancreas transplantation (n = 13), history of retransplantation (n = 3), those who received a pancreas graft from a living donor (n = 17), and those who were lost to follow up or had insufficient data (n = 18) (Fig. 1).
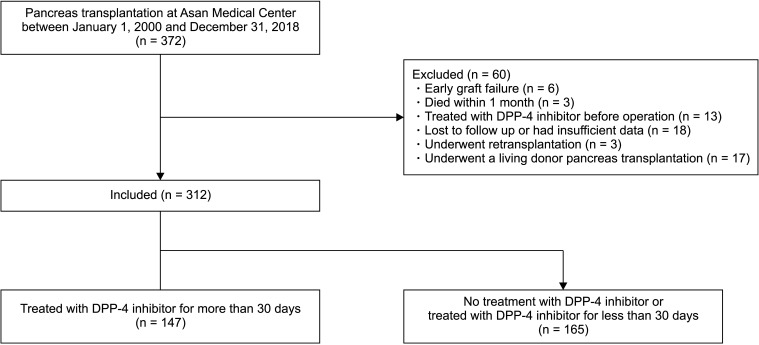
Finally, a total of 312 patients were included in this study. Of them, 147 patients who were treated with DPP-4 inhibitors for more than one month were categorized as the DPP-4 inhibitor group, and the remaining 165 patients who were treated with DPP-4 inhibitors for less than one month or never had been treated with DPP-4 inhibitors were categorized as the no DPP-4 inhibitor group.
The primary endpoint of this study was the difference in the metabolic outcomes between the 2 groups, which included the levels of serum fasting glucose, C-peptide, HbA1c, and fasting insulin at 1, 3, 6, 12, 24, and 36 months posttransplant. In addition, the homeostasis model assessment of insulin resistance (HOMA-IR) and β cell function (HOMA β cell) were calculated using the levels of fasting insulin and glucose [20].
Immunosuppression and surgical procedures
Rabbit anti-thymocyte globulin was given as an induction regimen, with a total dose ranging from 4.5 to 5.5 mg/kg. The maintenance regimen consisted of tacrolimus, mycophenolate mofetil, and methylprednisolone. The trough level of tacrolimus was targeted at 8–10 µg/L. Methylprednisolone was tapered and maintained in most patients, whereas it was withdrawn in those with simultaneous pancreas and kidney (SPK) transplantation. Surgical procedures of pancreas transplantation and the administration of postoperative anticoagulation were performed as previously described [21]. Insulin from the pancreas allograft was circulated systemically through the graft portal vein to the recipient's inferior vena cava or external iliac vein. Donor iliac arterial Y-graft was reconstructed with the superior mesenteric and splenic arteries reconstructed for anastomosis with the recipient's common iliac or external iliac artery. Exocrine drainage was performed by either bladder or enteric drainage.
Statistical analysis
Categorical variables were analyzed using the chi-square test and continuous variables were analyzed by the Student t-test or Wilcoxon rank-sum test. Using a linear mixed model, we compared the tendency of each variable over time and the values at each measuring point in the 2 groups were adjusted according to the type of transplant, type of diabetes mellitus, recipient's sex, age, and body mass index (BMI), and donor's age and BMI. Death-censored graft survival was estimated using the Kaplan-Meier survival estimates and the log-rank test. All statistical analysis was performed using the IBM SPSS Statistics for Windows, ver. 21.0 (IBM Corp., Armonk, NY, USA), and P < 0.05 was considered statistically significant.
Go to :
RESULTS
Baseline characteristics
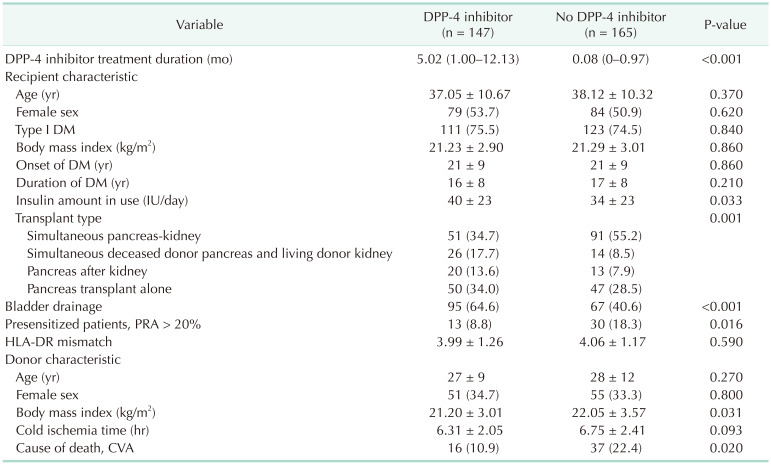
Among the 312 consecutive pancreas transplantation patients, 147 (47%) had been treated with DPP-4 inhibitors for more than 30 days (DPP-4 inhibitor group) and 165 (53%) had either been not treated with DPP-4 inhibitors (n = 137) or treated for less than 30 days (n = 28) (no DPP-4 inhibitor group) after pancreas transplantation (Table 1). Regarding the type of transplant, SPK transplantation was significantly less common in the DPP-4 inhibitor group (34.7% vs. 55.2%, P = 0.001) (Table 1). In addition, recipients in the DPP-4 inhibitor group used a larger amount of exogenous insulin compared with those in the no DPP-4 inhibitor group before pancreas transplantation (40 ± 23 IU/day vs. 34 ± 23 IU/day, P = 0.033). Bladder drainage was commonly performed in the DPP-4 inhibitor group (65% vs. 41%, P < 0.001), whereas presensitization recipients (panel reactive antibodies > 20%) were more common in the no DPP-4 inhibitor group (8.8% vs. 18.3%, P = 0.016). There were no significant differences between the 2 groups in terms of the donor characteristics except for lower BMI (21.20 ± 3.01 kg/m2
vs. 22.05 ± 3.57 kg/m2, P = 0.031) and lower cerebrovascular accident incidence (n = 16 vs. 37, P = 0.020) in the DPP-4 inhibitor group.
Comparison of metabolic variables between the DPP-4 inhibitor group and the no DPP-4 inhibitor group
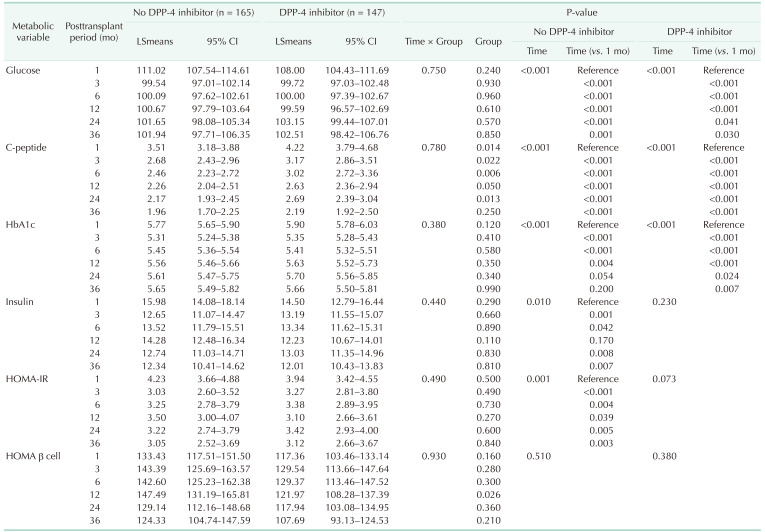
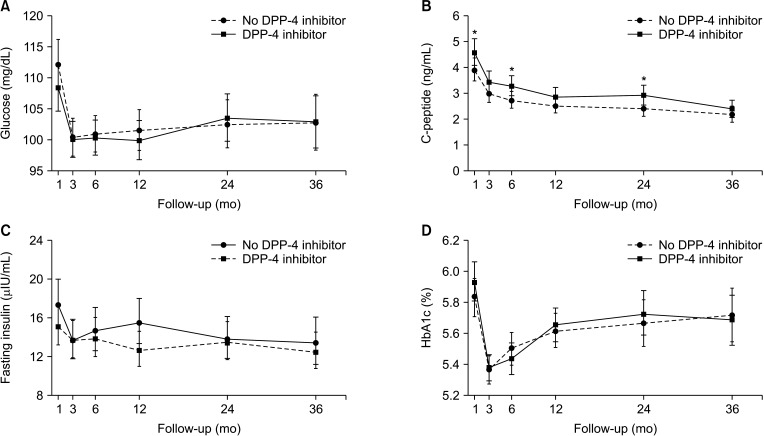
Metabolic variables were compared over time between the 2 groups before and after adjusting for transplant type, sex, age, BMI, diabetes type of recipients, and the age and BMI of donors. In both unadjusted (Table 2, Fig. 2) and adjusted (Table 3, Fig. 3) models, both groups showed decreasing levels of serum glucose, C-peptide, and HbA1c during follow-up compared with those at 1-month posttransplant. There were no significant differences in the metabolic variables at each time point between the 2 groups, except for the significantly higher serum C-peptide level in the DPP-4 inhibitor group until 24 months posttransplant (Table 2, Fig. 2B). Similarly, in the adjusted model, the levels of serum C-peptide in the DPP-4 inhibitor group at 1, 6, and 24 months posttransplant were significantly higher compared with those in the no DPP-4 inhibitor group (Fig. 3B). There were no significant differences in the levels of serum glucose, HbA1c, and insulin between the 2 groups (Fig. 3A, C, and D).
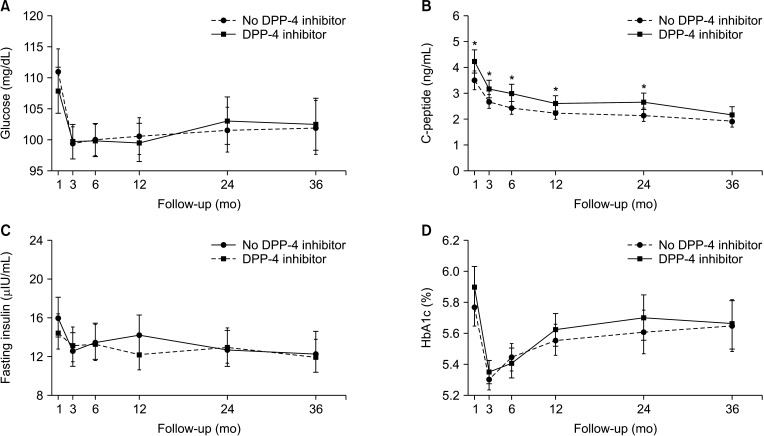 | Fig. 2Comparison of metabolic variables including glucose (A), C-peptide (B), fasting insulin (C), and hemoglobin A1c (HbA1c) (D) between the dipeptidyl peptidase 4 (DPP-4) inhibitor group and the no DPP-4 inhibitor group in the unadjusted linear mixed model. *P < 0.05.
|
 | Fig. 3Comparison of metabolic variables including glucose (A), C-peptide (B), fasting insulin (C), and hemoglobin A1c (HbA1c) (D) between the dipeptidyl peptidase 4 (DPP-4) inhibitor group and the no DPP-4 inhibitor group in the adjusted linear mixed model. *P < 0.05.
|
Table 2
Comparison of metabolic variables between the DPP-4 inhibitor group and the no DPP-4 inhibitor group (unadjusted linear mixed model)
![]()
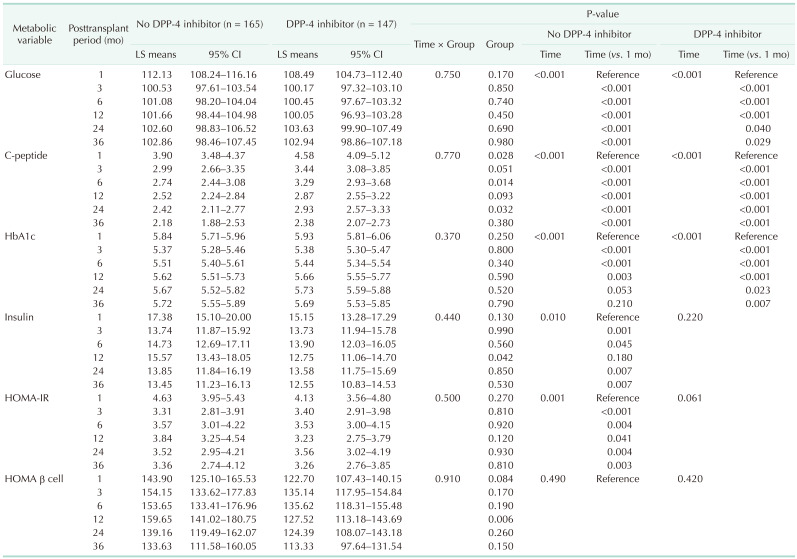
HOMA-IR and HOMA β cell did not show significant differences between the 2 groups, except for HOMA β cell at 12 months posttransplant in the adjusted model (LSmeans [95% confidence interval]: 127.52 [113.18–143.69] vs. 159.65 [141.02–180.75], P = 0.006) (Table 3, Fig. 4).
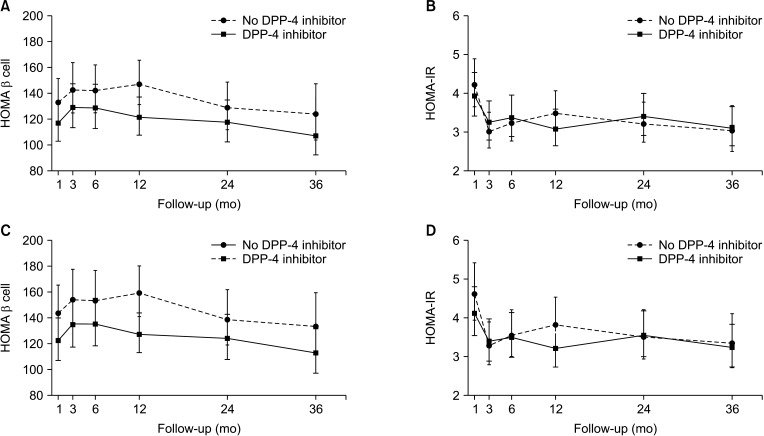 | Fig. 4Comparison of metabolic variables including HOMA β cell and HOMA-IR between the dipeptidyl peptidase 4 (DPP-4) inhibitor group and the no DPP-4 inhibitor group in the unadjusted (A and B) and adjusted (C and D) linear mixed models. HOMA-IR, homeostasis model assessment (HOMA) of insulin resistance; HOMA β cell, HOMA β cell function.
|
Comparison of patient and graft survival between the DPP-4 inhibitor group and the no DPP-4 inhibitor group
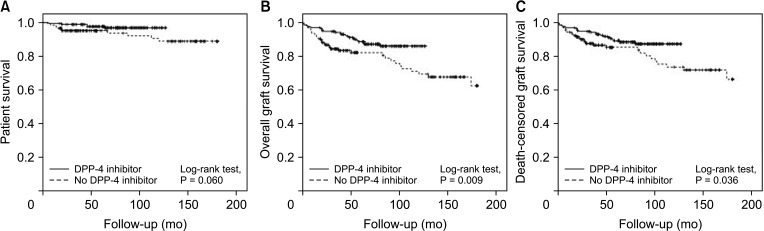
During the 15-years of follow-up, the overall (log-rank test, P = 0.009) and death-censored (log-rank test, P = 0.036) pancreas graft survival were significantly higher in the DPP-4 inhibitor group compared with the no DPP-4 group; in contrast, there were no significant differences in the biopsy-proven acute rejection rate and patient survival rate between the 2 groups (Fig. 5).
Go to :
DISCUSSION
In this study, we found that administration of DPP-4 inhibitors after pancreas transplantation was associated with better clinical outcomes in terms of metabolic results and β cell function. We also observed that recipients treated with DPP-4 inhibitors in the early posttransplant period had better clinical outcomes in terms of overall and death-censored pancreas allograft survival than those who were not treated with DPP-4 inhibitors. Although the majority of variables were not significantly different between the 2 groups, the C-peptide levels were significantly higher in the DPP-4 inhibitor group during the follow-up period.
We hypothesized that treatment with DPP-4 inhibitors would be associated with increases in the rate of pancreas allograft survival through improvements in insulin sensitivity; contrary to our expectation; however, we could not find a significant improvement in insulin sensitivity as estimated by HOMAIR in the DPP-4 inhibitor group. It has been suggested that the HOMA-IR is limited for representing the status of insulin sensitivity, as the correlation between HOMA-IR and the M-value measured by the euglycemic hyperinsulinemic glucose clamp technique is weak or absent, especially in East Asians; moreover, the validity of the HOMA-IR has been shown to vary according to the BMI [22,23].
Although pancreas transplantation is an ideal treatment for β cell failure, the islet cells of the transplanted pancreas are at the risk of damage by ischemic-reperfusion injury, rejection, and infection [24]. Furthermore, long-term use of maintenance immunosuppressants such as calcineurin inhibitors confers a negative influence on β cell function, because they disturb the activation of the relevant signaling pathways and transcription factors [25].
The effects of DPP-4 inhibitors in patients with diabetes have been demonstrated in multiple studies. Aside from aiding in the maintenance of adequate glucose levels, DPP-4 inhibitors also confer a positive influence on the cardiovascular and hepatic health as well as the central nervous system [19]. Using a transgenic mouse model, Shimizu et al. [26] found that vildagliptin has protective effects on pancreatic β cells by activating the GLP1 pathway, as the administration of vildagliptin for 24 weeks led to increases in the β cell mass and serum insulin. In addition, it has been suggested that DPP-4 inhibitors not only counteract the immunosuppressant-induced inactivation in insulin secretion but also decrease the levels of glucagon and improve insulin sensitivity [27,28]. Taken together, it may be reasonable to reduce the use of calcineurin inhibitors and to incorporate DPP-4 inhibitors for long-term maintenance of endocrine function and pancreas allograft survival.
Previous studies examined the effect of DPP-4 inhibitors on β cell function and glucose control after pancreas or islet transplantation. Ergin et al. [29] reported that compared with standard observation, treatment with a DPP-4 inhibitor for at least 1 year in recipients with hyperglycemia after pancreas transplantation prolonged the time to insulin therapy. Kim et al. [30] reported that sitagliptin treatment in islet-transplanted mice led to lower serum glucose levels and higher serum insulin levels. To our knowledge, however, our current study is the first to evaluate the effect of early administration of DPP-4 inhibitors on the metabolic and clinical outcomes after pancreas transplantation.
There are some limitations to this study. First of all, this was a retrospective study based on the medical records gathered at a single center, which limits its generalizability. Second, most of the recipients in the DPP-4 inhibitor group underwent pancreas transplantation in the later period of this study. However, there was no prominent difference in surgical techniques and postoperative management that might affect the main outcomes although there is a possibility of selection bias due to differences in bladder drainage, transplantation type, and donor profiles. Third, we defined the DPP-4 inhibitor groups as those who were treated with DPP-4 inhibitors for more than 30 days. The small number of the included patients limit the general application of the cut-off duration of DPP-4 inhibitor maintenance. In addition, our study did not assess insulin sensitivity by applying an effective insulin sensitivity index such as Matsuda's index.
In conclusion, this study suggests that early administration of DPP-4 inhibitors after pancreas transplantation may have beneficial effects on metabolic and clinical outcomes. Prospective studies are needed to further validate the effect of DPP-4 inhibitors on the improvement of insulin sensitivity after pancreas transplantation.
Go to :
 XML Download
XML Download