

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rectal cancer is a common malignant tumor of which low rectal cancer accounts for approximately 65%. The lesion is deep into the pelvis as the lower edge of the tumor being less than 5 cm from the dentate line, thus making operation more difficult [1]. The gold standard for curative resection remains total mesorectal excision (TME), and the quality of the TME is one of the most important prognostic factors for local recurrence. Laparoscopic TME (LaTME) is a classic surgical approach for low rectal cancer in recent years. Its safety, feasibility, and tumor radicalization has been confirmed by evidence-based medicine in recent years [2]. Proper TME specimens with negative resection margins are inherently challenging due to patient and tumor-related factors. These difficulties have not been overcome with the advent of the laparoscopic approach. Transanal TME (TaTME) is an innovative surgical technique developed to overcome the limitations in exposure and instrumentation in low pelvic surgery. It was suggested that TaTME appeared to be superior to LaTME for mid-to-low rectal cancer by meta-analysis [34], but these studies did not distinguish between mid rectal cancer and low rectal cancer. Most of the TaTME studies [5] reported that the distal rectal margin of rectal cancer was less than 5 cm. Therefore, distal resection of the mesorectum was also less than 5 cm, which was unable to achieve the TME principle for mid rectal cancer. For mid rectal cancer, the transabdominal approach itself is not too difficult, whereas the transanal approach increases the difficulty of surgery instead. Also, for low rectal cancer, difficulty existed in exposure with transabdominal approach. However, the proposal of TaTME provided a new method to solve this problem. TaTME for rectal malignancies is largely referred to as treatment of mid to low, especially low, rectal cancer. There is currently no precise definition for low rectal cancer. Chen et al. [6] believe that low rectal cancer should be defined as cancer below the peritoneal reflex, generally less than 7 cm from the anal verge. The current meta-analysis combines mid and low rectal cancer. For low rectal cancer, it is still inconclusive whether TaTME is more advantageous [7], and any meta-analysis purely for low rectal cancer is not seen yet. Therefore, this study conducted a meta-analysis of TaTME and LaTME comparative studies for low rectal cancer to provide a basis to evaluate the safety and efficacy of the procedure.
Go to : 
METHODS
Institutional Review Board approval for this study was obtained from Guangzhou Red Cross Hospital, Medical College of Jinan University (No. 2020-162-01), and the written informed consent from the patient was exempted. A systematic literature search was conducted using the web-based databases, China National Knowledge Infrastructure, Chinese BioMedical Database, PubMed, Embase, Cochrane Central Register of Controlled Trials, and Wanfang Database from database establishment to May 2020. Search terms included the following words: (transanal total mesorectal excision OR TaTME OR transanal minimally invasive surgery OR TAMIS OR natural orifice transluminal endoscopic surgery OR NOTES) AND (laparoscopy OR laparoscopic OR laparoscopic-assisted) AND (total mesorectal excision OR TME) AND (rectal cancer OR rectal carcinoma OR rectal adenocarcinoma OR rectal neoplasms). Published studies were considered for inclusion if they met the following criteria: the study design was randomized controlled trials (RCTs) or cohort studies, or matched case-control studies; the study population comprised patients definitely diagnosed with low rectal cancer (the distance of the tumor from the anal verge was less than 7 cm); outcomes of interest were compared between the TaTME and LaTME groups; outcome indicators included at least one of the least: intraoperative indicators, postoperative complications, oncology index, and follow-up results. If there are duplicates in the literature, choose the latest one. Whereas, studies with benign lesions only, or no distinct group of malignant rectal tumor, studies on other surgical methods, studies in languages other than English or Chinese, and correspondences, letters, case reports, reviews, meta-analysis, and conference abstracts were excluded.
The initial studies were retrieved, and data were extracted independently by 2 investigators (JR and HR), and any disagreements were resolved by consulting another author (SL). The extracted information mainly included: basic information, including author, year, country, etc.; baseline characteristics of the study, including sample size of each group, patient age, sex, body mass index (BMI), American Society of Anesthesiologists physical status (ASA PS) classification [8], TNM stage; the main outcome indicators included conversion, mesorectal resection quality, circumferential resection margin (CRM) involvement, CRM distance, distal resection margin (DRM) involvement, DRM distance, local R1 resection, intraoperative complications, morbidity, anastomotic leakage, severe morbidity, mortality, and local recurrence; secondary outcome indicators included operative time, intraoperative blood loss, harvested lymph nodes, and hospital stay. RCTs were evaluated using the Jadad scale [9] and non-RCTs (NRCs) were evaluated using the Newcastle-Ottawa Scale [10].
All analyses were performed using Review Manager (ver. 5.3, Cochrane Collaboration; available at http://community.cochrane.org/tools/review-production-tools/revman-5). For dichotomous data, risk ratios (RRs) and 95% confidence intervals (CIs) were generated for comparison between TaTME and LaTME. For continuous data, mean differences (MDs) and 95% CIs were generated. It was considered indicative of low, moderate and high heterogeneity when I2 ≤ 25%, 25% < I2 < 50%, and I2 ≥ 50%, respectively. When no obvious inter-study heterogeneity was identified from an I2 test, the results of the fixed-effect model were also provided for reference. If there was statistical heterogeneity among the results of each study, the source of heterogeneity was further analyzed. After excluding the influence of obvious clinical heterogeneity, the random effect model was applied. Sensitivity analysis was applied for significant heterogeneity. Differences were considered statistically significant at a P-value of ≤0.05.
Go to :
RESULTS
Characteristics of included studies
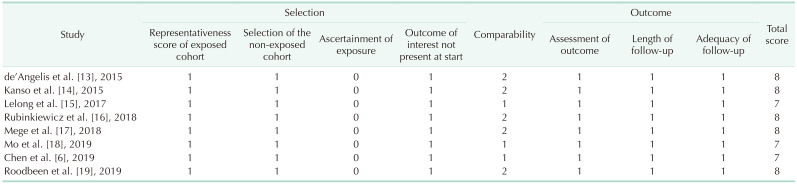
A total of 804 relevant publications were identified on initial literature search. Of these, 2 RCT [1112] and 8 NRCs [613141516171819] with high quality, involving 772 patients, met the inclusion criteria. The study selection process was illustrated in Fig. 1. Among these, 378 patients (49.0%) underwent TaTME and 394 (51.0%) underwent LaTME. The characteristics of the studies were shown in Table 1. No statistically significant differences were seen in baseline data such as age, sex, BMI, ASA PS classification, neoadjuvant therapy, and TNM stage between the 2 groups. The RCTs with a score of 4 on the Jadad scale was considered to be of high quality. All NRCs ranging from 7 to 8 stars on the Newcastle-Ottawa Scale were indicative of high quality, shown in Table 2.
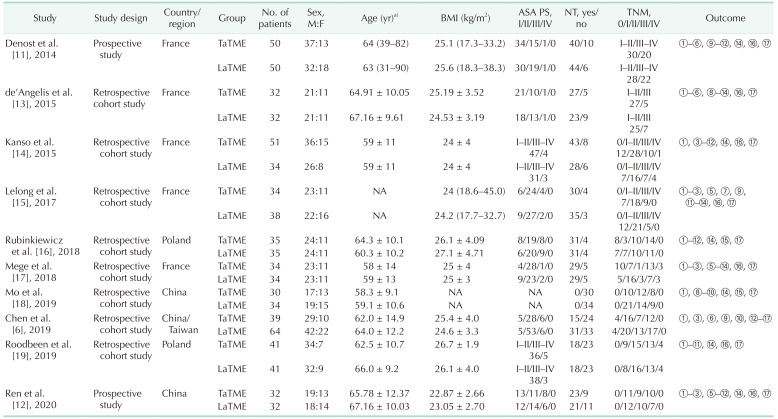
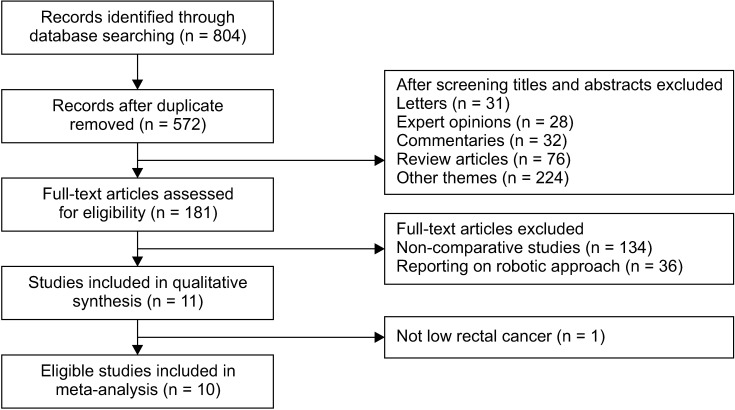
Table 1
Clinical and demographic characteristics of included studies in the meta-analysis
M, male; F, female; BMI, body mass index; ASA PS, American Society of Anesthesiologists physical status classification; NT, neoadjuvant therapy; TaTME, transanal total mesorectal excision; LaTME, laparoscopic total mesorectal excision; NA, not available.
Outcome: ① conversion, ② mesorectal resection quality, ③ circumferential resection margin (CRM) involvement, ④ CRM distance, ⑤ distal resection margin (DRM) involvement, ⑥ DRM distance, ⑦ local R1 resection, ⑧ intraoperative complications, ⑨ morbidity, ⑩ anastomotic leakage, ⑪ severe morbidity, ⑫ mortality, ⑬ local recurrence, ⑭ operative time, ⑮ intraoperative blood loss, ⑯ harvested lymph nodes, and ⑰ hospital stay.
a)Median (range) or mean ± standard deviation.
![]()
Meta-analysis results
Conversion
Conversion was defined as a procedure that was started with the intention of performing a laparoscopic dissection but was completed as an open resection requiring a midline laparotomy. Ten studies [6111213141516171819] mentioned the conversion. The conversions were significantly lower in TaTME group as compared to those in LaTME group (RR, 0.25; 95% CI, 0.11–0.54; P = 0.001). Additionally, heterogeneity among the studies was not significant (P = 0.360, I2 = 9%) (Fig. 2A).
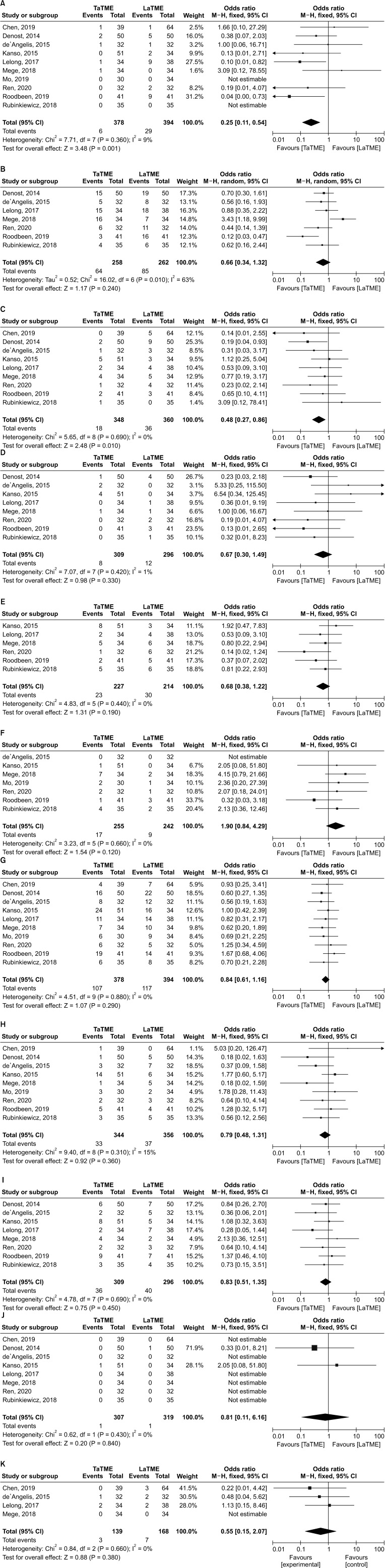 | Fig. 2Forest plots of risk ratio between transanal total mesorectal excision (TaTME) group and laparoscopic total mesorectal excision (LaTME) group. (A) Conversion. (B) Mesorectal resection quality. (C) Circumferential resection margin involvement. (D) Distal resection margin involvement. (E) Local R1 resection. (F) Intraoperative complications. (G) Morbidity. (H) Anastomotic leakage. (I) Severe morbidity. (J) Mortality. (K) Local recurrence. CI, confidence interval; df, degree of freedom.
|
Mesorectal resection quality
Seven studies [11121315161719] reported mesorectal resection quality. No significant difference was discovered between the 2 groups with respect to mesorectal resection quality (RR, 0.66; 95% CI, 0.34–1.32; P = 0.240). Nonetheless, heterogeneity was obviously significant (P = 0.010, I2 = 63%) and the random effects model was used (Fig. 2B).
Circumferential resection margin distance
Six studies [111213141619] described the data. The intergroup difference in terms of DRM distance was not significant (MD, 1.67; 95% CI, −0.42–3.75; P = 0.120). However, heterogeneity was highly significant (P < 0.001, I2 = 94%); therefore, the random effects model was used (Fig. 3A).
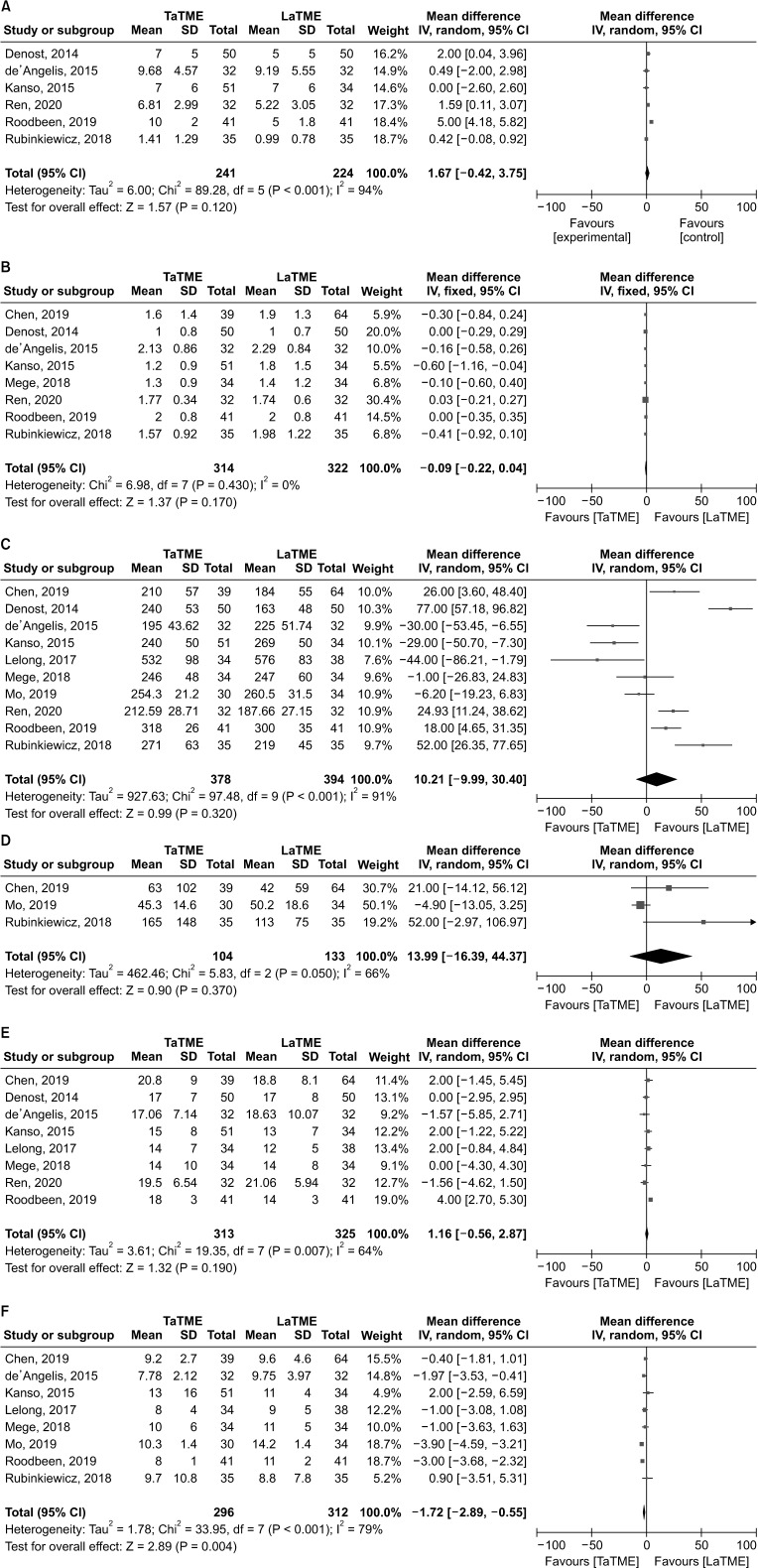 | Fig. 3Forest plots of mean difference between transanal total mesorectal excision (TaTME) group and laparoscopic total mesorectal excision (LaTME) group. (A) Circumferential resection margin distance. (B) Distal resection margin distance. (C) Operative time. (D) Intraoperative blood loss. (E) Harvested lymph nodes. (F) Hospital stay. SD, standard deviation; IV, inverse variance methods; CI, confidence interval; df, degree of freedom.
|
Intraoperative complications
Seven studies [12131416171819] described the intraoperative complications. Pooled analysis indicated that the intergroup difference in terms of intraoperative complications was not significant (RR, 1.90; 95% CI, 0.84–4.29; P = 0.120). Heterogeneity among the studies was not significant (P = 0.660, I2 = 0%) (Fig. 2F).
Severe morbidity
Severe morbidity was described as Clavien-Dindo classification III–V [20]. Eight studies [1112131415161719] reported the data. Pooled analysis demonstrated no significant difference with respect to the rates of severe morbidity (RR, 0.83; 95% CI, 0.51–1.35; P = 0.450). No heterogeneity was observed (P = 0.690, I2 = 0%) (Fig. 2I).
Local recurrence
Only 4 eligible studies [6131517] mentioned local recurrence. No significant difference was found with respect to local recurrence between the 2 groups (RR, 0.55; 95% CI, 0.15–2.07; P = 0.380). Meanwhile, no heterogeneity was observed in this respect (P = 0.660, I2 = 0%) (Fig. 2K). However, the follow-up time was quite different among different groups. The mean follow-up was 32.06 months for the TaTME group and 62.91 months for the LaTME group in the study of de'Angelis et al. [13], 31.9 months and 60.3 months in the study of Lelong et al. [15], 13 months and 25 months in the study of Mege et al. [17], and 26.3 months in the study of Chen et al. [6].
Operative time
All studies [6111213141516171819] described the operative time. Pooled analysis indicated that the intergroup difference in terms of operative time was not significant (MD, 10.21; 95% CI, −9.99–30.40; P = 0.320). Nevertheless, a significant heterogeneity was observed (P < 0.001, I2 = 91%) (Fig. 3C). Six studies [61112161718] adopted a 1-team approach, 1 study [13] adopted a 2-team approach, it was not mentioned in 3 studies [141519].
Sensitivity analysis
Sensitivity analysis was performed on outcomes with high heterogeneity (mesorectal resection quality, CRM distance, operative time, intraoperative blood loss, harvested lymph nodes, and hospital stay), and each study was excluded 1 by 1 to test the stability of relevant results. For mesorectal resection quality (RR, 0.66; 95% CI, 0.34–1.32; P = 0.240, I2 = 63%), after removing the study of Mege et al. [17], pooled analysis indicated that the TaTME group had better results (RR, 0.53; 95% CI, 0.32–0.88; P = 0.010, I2 = 21%). For CRM distance (MD, 1.67; 95% CI, −0.42–3.75; P = 0.120, I2 = 94%), pooled analysis demonstrated that of the TaTME group was longer (MD, 0.69; 95% CI, 0.12–1.26; P = 0.020, I2 = 9%) after removing the study of Roodbeen et al. [19]. Also, intraoperative blood loss was less in LaTME group (MD, 29.99; 95% CI, 0.39–59.59; P = 0.050, I2 = 0%) after removing the study of Mo et al. [18]. For operative time, harvested lymph nodes, and hospital stay, the change of I2 value was not obvious after we excluded each study 1 by 1, and the statistical results of combined effect were not reversed, indicating the stability of each study.
Go to :
DISCUSSION
Since Heald et al. proposed the theory of TME for rectal cancer in 1982 [19], this principle became the gold standard for middle and low rectal cancer surgery. Laparoscopic surgery was conditionally recommended in the treatment of rectal cancer in the 2016 edition of the National Comprehensive Cancer Network (NCCN), “Clinical Practice Guidelines for Rectal Cancer” [21]. However, for male, obesity, and lower rectal cancer patients with narrow pelvis, difficulty existed in exposure whether with open approach or laparoscopic surgery [21], which lead to incomplete resection of rectal mesentery, insufficient or excessive distal margin. For such so-called “difficult pelvis” patients, there were still huge challenges to complete highquality TME surgery. The proposal of TaTME provided a new method to solve this problem. In 2010, Sylla et al. [22] reported the first case of TaTME performed with transanal endoscopic microsurgery combined with laparoscopy. TaTME, also known as ‘bottom-up’ TME, had been pioneered to overcome these difficulties. The approach from below offers clear, direct visualization of the dissection plane, even in a narrow pelvis, allowing a more precise and trauma-free dissection, which should improve the quality of the TME specimen and decrease positive resection margins. In addition, it can be performed accurately through the anal approach, so the space around the distal mesorectum can be better exposed and dissected, which may reduce the risk of pelvic nerve injury and protect the function of pelvic organs. It may be one of the reasons for the lower rate of conversion for TaTME; improving the quality of surgery and reducing the secondary damage.
Zheng and Ma [23] are worried about whether TaTME surgery for low rectal cancer conformed to the principles of TME. For low rectal cancer, we make a circular incision 2 cm from the tumor. The distal margin is close to the levator ani muscle and can meet the principle of TME. Especially for patients with ultra-low rectal cancer or who intend to undergo intersphincteric resection, the rectal wall is incised through the anus, and then the space of internal and external sphincter is expanded and separated upward, the mesorectum can be completely removed. Perdawood et al. [24] compared the mesorectal resection quality of rectal cancer, especially for tumors below the peritoneal reflex after TaTME and LaTME. It was found that the mesorectal defects in the LaTME group were significantly higher when the tumor was below the peritoneal reflex. It was believed that transanal bottom-up TaTME could help improve the quality of specimens for low rectal cancer. Veltcamp et al. [25] compared the postoperative mesorectal remnants of TaTME and LaTME; postoperative pelvic magnetic resonance imaging showed that the postoperative mesorectal remnant rate of TaTME was significantly lower than that of LaTME surgery (3.1% vs. 46.9%, P < 0.001). Multivariate analysis showed that the operation method was the only independent risk factor affecting postoperative residual mesorectum. In the LaTME group, the residual mesorectum was mostly located below or around the anastomosis, indicating that the distal mesorectum was incomplete during LaTME surgery. Pooled analysis demonstrated that CRM involvement was significantly lower in TaTME group as compared to those in LaTME group, and the mesorectal resection quality, CRM distance, DRM distance, DRM involvement, local R1 resection, and local recurrence were similar in this meta-analysis. However, the mesorectal resection quality and CRM distance of the TaTME group were superior to those of the LaTME group in the sensitivity analysis. It is usually felt that TaTME has an advantage over LaTME in securing the distal margin, which is done under direct vision; and this meta-analysis showed that DRM involvement was 8 of 309 in the TaTME group and 12 of 296 in the LaTME group, respectively. However, due to the low incidence of DRM involvement, pooled analysis demonstrated no difference. On the other hand, LaTME is prone to the problem of insufficient or excessive distal margin; possibly one of the reasons that the average DRM is indistinguishable from TaTME.
Recently, data from a national registry study in Norway [26] showed that the local recurrence rate of TaTME surgery was significantly higher than LaTME, resulting in Norway suspending TaTME nationwide. However, the method of the Norwegian study should be investigated in a proper RCT that avoids at least 2 main pitfalls; the “poor” arm problem and inclusion of only low-risk tumors. In ordinary TME, a very high proportion of patients were not at clear risk for local recurrence. The Norwegian study adjusted for case mix and some selection biases, which was lacking in many observational studies [26]. Moreover, the pre-TaTME experience of these surgeons with both laparoscopic TME and transanal endoscopic surgery was not stipulated. The key was continued refinement and modification by masters of the craft. The adverse outcomes reported in Norway can be avoidable by stringent patient selection, structured surgical training, and frequent performance of TaTME within the context of high-volume specialty teams [27].
The most important complications for TaTME are urinary dysfunction and urethral injury. Urethral injuries were reported in some early series, the urethral injury rate was 2.5%–6.6%. It is safe and quick to perform dissection from the posterior wall of the rectum in TaTME, followed by dissection from the lateral side to the anterior wall of the rectum. Dissection from the posterior to anterior wall could avoid urinary system injury [18]. During transanal endoscopic surgery, CO2 pressure is high in a small space, especially under conventional pneumoperitoneum conditions. If bleeding occurs, CO2 may enter blood vessels and cause pulmonary embolism. It has been reported that 3 cases of CO2 embolism occurred in 80 patients with TaTME [28]. This problem needs to be properly communicated with the anesthesiologist. If bleeding occurs during the operation, the anesthesiologist should be reminded to pay attention and respond accordingly.
The treatment strategy for lateral lymph node dissection (LLND) differs between Western and Eastern countries [2930]. A standard treatment model has been established in Western countries: patients with early rectal cancer receive TME surgery only, and for advanced cases, European Society of Medical Oncology and NCCN guidelines recommend neoadjuvant chemoradiotherapy combined with TME [29]. However, Japanese scholars routinely consider TME plus LLND for resectable middle and low rectal cancer [30]. The dissection of lateral lymph node during TaTME is difficult, of the 10 studies included in this meta-analysis, 7 were from Europe and 3 were from China. LLND was not routinely performed in these regions; the studies did not mention it.
This meta-analysis showed that the TaTME group was superior to the LaTME group in terms of conversion, CRM involvement, and hospital stay for low rectal cancer, while the intergroup difference was not significant in terms of mesorectal resection quality, CRM distance, DRM involvement, DRM distance, local R1 resection, intraoperative complications, morbidity, anastomotic leakage, severe morbidity, mortality, local recurrence, operative time, intraoperative blood loss, and harvested lymph nodes. These suggest that TaTME is a promising surgical technique and is fully a safe and efficacious option in managing low rectal cancer. Larger scale, national, multicentric RCTs are warranted to further verify these results and the possible superiority of TaTME.
Compared with the similar meta-analysis published in the past [34], case selection was completely low rectal cancer, the latest literature was included, and more outcome indicators were analyzed. The limitation of this study was that most of the literature included were retrospective studies, and only 2 were RCTs. More prospective RCTs are needed to clarify the advantages of TaTME. Meanwhile, the languages included were only English and Chinese, the relevant literature in other languages were not included, and there might be potential publication bias.
In conclusion, TaTME is a promising surgical technique and is fully a safe and efficacious option in managing low rectal cancer that will possibly offer a feasible alternative to LaTME in the future. Larger scale, national, multicentric RCTs are warranted to further verify these results and the possible superiority of TaTME.
Go to :
 XML Download
XML Download