

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Locally advanced or recurrent colorectal cancer often invades into surrounding organs within the narrow pelvic space. Such disease is complex to treat, because the patient often presents with symptoms of bleeding, obstruction, and fistulation [1]. Prognosis for these patients is poor, with a median survival less than 1 year. Even patients who receive palliative chemotherapy can only extend their lifetime by 10–15 months [2]. Microscopically complete (R0) resection offers the only potential for cure [23]. Pelvic exenteration (PE) was first described in 1948 and has been indicated for the purpose of R0 resection of locally invasive pelvic malignancies [4]. However, PE is a highly invasive procedure, and extensive resection often correlates with higher morbidity and mortality rates [5]. A previous systemic review showed overall complication rates ranging between 31.6% and 86%, with a high proportion of patients requiring surgical intervention for complications (14.6%) [5]. Further, the mortality rate ranged between 5% and 23%, even with advanced operative techniques and perioperative care. Median incomplete resection rate (R1/R2) was relatively high, at 18.9%. Microscopic advanced disease and the difficulty of handling large tumors in the narrow pelvis could reflect a positive circumferential margin. Accomplishing both surgical and oncological safety would maximize the benefit from the procedure.
Laparoscopic surgery for colorectal cancer has become established as an alternative to open surgery [6]. Previous randomized controlled studies have demonstrated potential advantages of laparoscopic surgery with regard to short-term outcomes, including lower blood loss, faster recovery, and lower rates of postoperative complications [67]. In the past, PE was usually performed under an open approach [8]. However, several recent reports have suggested laparoscopic PE as a feasible and oncologically safe alternative to the open approach [91011].
Transperineal surgery is another promising approach for rectal cancer [12]. The approach can be performed from the lower edge of the tumor for direct visualization, which could facilitate safe distal margins [13]. A multidirectional approach may keep dissection within an appropriate layer, which could improve the rate of R0 resection. Furthermore, when the surgery was performed under a 2-team approach, with transabdominal and transperineal teams operating simultaneously, better perioperative outcomes including shorter operation time and lower blood loss appeared achievable [14].
PE using a transperineal approach is reported to have potential for reducing operation time, blood loss, and surgical stress, though few case reports have examined these potential benefits [1516].
The aim of this study was to identify the feasibility and safety of combined transabdominal and transperineal endoscopic PE. We also examined the effectiveness of the procedure under a 2-team approach.
METHODS
This multicenter, retrospective study was designed by the Nagasaki Colorectal Oncology Group. Between April 2016 and March 2020, 20 patients who underwent combined transabdominal and transperineal endoscopic PE for colorectal malignancies in participating hospitals were included in this study. Patients with distant metastasis and emergency surgery were excluded. A final total of 14 patients were eligible for analysis. All patients were diagnosed by physical examination, blood tests, computed tomography, magnetic resonance imaging, and colonoscopy. Indications for perioperative chemotherapy and resectability were discussed at team meetings. Total PE was defined as en bloc resection of the rectum, bladder, uterus and vagina in females, prostate in males, and lateral pelvic lymph nodes. Posterior PE was defined as en bloc resection of the rectum, and vagina in females, sparing the bladder. The study was reviewed and approved by the Clinical Research Review Board of Nagasaki University Hospital and Sasebo City General Hospital (No. 16062715-2) with the written informed consent.
Surgery was performed as transabdominal and transperineal parts. The patient was placed in a Trendelenburg lithotomy position. The transabdominal part was performed using 5 ports; 12-mm ports at the umbilicus and right lower quadrant, and 5-mm ports at the upper right and left and lower left quadrants. Medial-to-lateral retroperitoneal resection was performed first. The inferior mesenteric artery and vein were then resected. The descending colon was dissected by taking down Toldt's fusion fascia. After resecting the mesentery of the sigmoid colon, the sigmoid colon was transected using a linear stapler. Bilateral ureters were mobilized and dissected at the level of the ureterovesical junction. After the hypogastric nerve was resected at the level of the aortic branch, the surgeon dissected the posterior rectal space. Branches of the internal iliac vessels were clipped and resected, then lateral pelvic lymph node dissection was performed bilaterally. On the anterior side, the space of Retzius was dissected and the dorsal vein complex (DVC) was exposed.
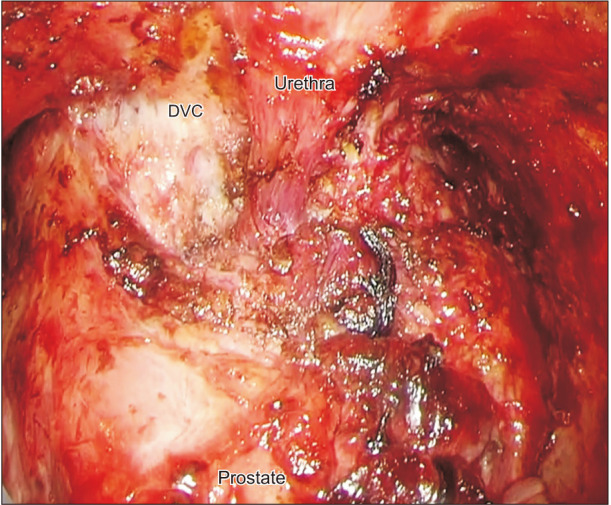
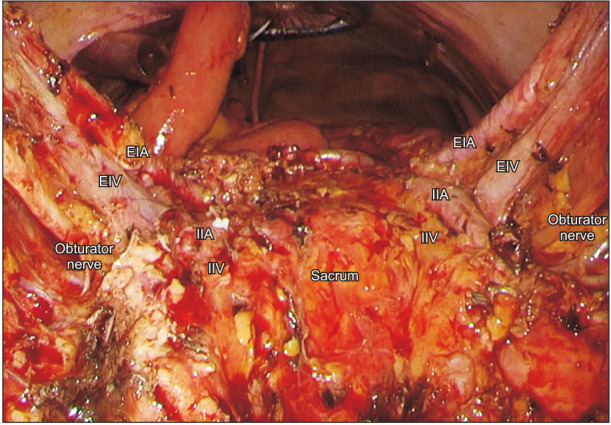
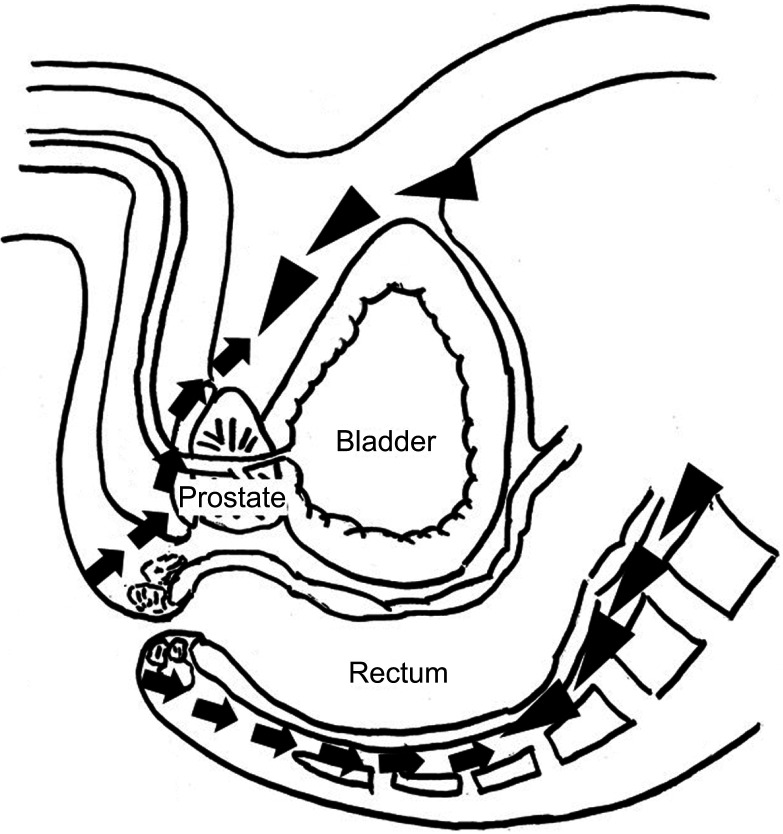
In the transperineal part, the anus was closed using a double purse-string suture. After making the perianal skin incision, the GelPOINT Path® (Applied Medical, Rancho Santa Margarita, CA, USA) was set. Three ports were installed, then the perianal fat tissue was dissected and the levator ani muscle was exposed posteriorly. Anteriorly, the transverse perineal muscle and branch of the internal pudendal vessels were resected using a vessel sealer. The bulbocavernous muscle was divided using the vessel-sealing system. The urethra was then clipped and transected. The DVC was identified and divided using the vessel-sealing system (Fig. 1), and rendezvous was achieved. Finally, the specimen was extracted through the abdominal wound (Fig. 2). An ileal conduit reservoir was constructed through the umbilical wound. Schematic diagrams of the PE procedure presented in this study are presented in Fig. 3.
Surgery performed by a transabdominal team and a transperineal team working simultaneously was defined as the 2-team approach (T group), while that performed separately was the 1-team approach (O group). We excluded patients who required a large skin incision in the perineal region from the 2-team approach, as we could not perform the laparoscopic approach from the anal side. To compare clinical features between groups, the following data were collected; sex, age at surgery, body mass index (BMI), American Society of Anesthesiologists (ASA) performance status (PS) classification, comorbidity, preoperative diagnosis, histological type, and preoperative treatment. Surgical and pathological data, including the operative procedure, lateral lymph node dissection, proportion of conversion to open surgery, operation time, time to specimen removal, estimated blood loss, blood transfusion, tumor size, lymphovascular invasion, number of retrieved lymph nodes, R0 resection rate, postoperative complications, pathological stage, postoperative hospital stay, and postoperative treatment were also compared between groups. Some patients did not receive postoperative chemotherapy based on the decision of the attending physician, the wishes of the patient, or the poor general condition of the patient due to postoperative complications.
Postoperative complications were defined as complications that occurred within 30 days of the primary surgery. Patients with complications of Clavien-Dindo (CD) grade 2 or higher were included in the complication group. Patients with recurrence during follow-up were also investigated for primary tumor site, surgical approach, postoperative chemotherapy, time to adjuvant chemotherapy, recurrence site, treatment after recurrence, and prognosis.
Statistical analysis was performed using bell curve for Excel version 2.02 software (Social Survey Research Information Corp., Tokyo, Japan). Data are presented as median values with ranges. Differences in categorical variables were compared using Fisher exact test or the chi-square test, as appropriate. Differences in continuous variables were analyzed using the Mann-Whitney U-test. All P-values of <0.05 were considered significant.
RESULTS
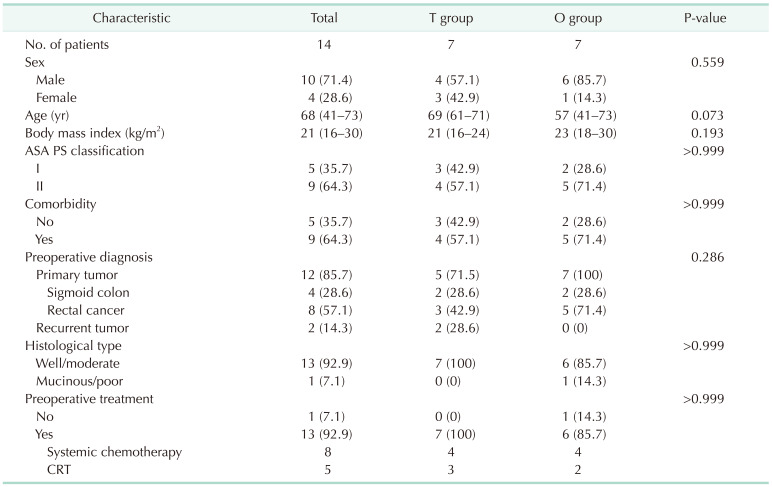
Table 1 shows clinical differences between the T group and O group. Sex, age, BMI, ASA PS classification, comorbidities, preoperative diagnosis, histological type, and preoperative treatment were comparable between groups.
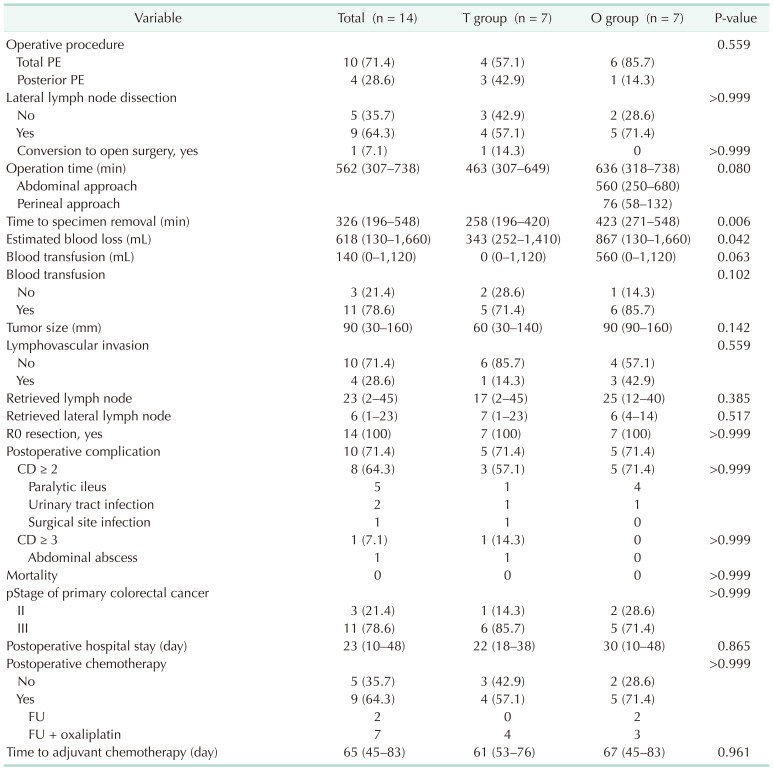
Table 2 shows the surgical and pathological differences between the T group and O group. Operation time and estimated blood loss in all patients were 562 minutes (range, 307–738 minutes) and 140 mL (range, 130–1,660 mL). All patients successfully underwent R0 resection. Operation time tended to be shorter in the T group (463 minutes) than in the O group (636 minutes, P = 0.080). Time to specimen removal was significantly shorter (258 minutes vs. 423 minutes, P = 0.006), blood loss was lower (343 mL vs. 867 mL, P = 0.042), and blood transfusion was less (0 mL vs. 560 mL, P = 0.063) in the T group. One patient in the T group required conversion to open surgery due to uncontrolled intraoperative bleeding. No significant differences were evident between groups for the remaining factors, including operative procedure, lateral lymph node dissection, tumor size, lymphovascular invasion, retrieved lymph nodes, postoperative complications, pathological stage, postoperative hospital stay, proportion of postoperative chemotherapy, and time to adjuvant chemotherapy.
Table 3 shows the patients who experienced recurrence after PE. Median follow-up for all patients was 21 months (range, 2–46 months). Five patients (35.7%) experienced recurrence during follow-up. The primary tumor site was the sigmoid colon in 3 patients and the rectum in 2 patients. Four cases were treated using a 1-team approach. Four patients received postoperative chemotherapy (fluorouracil [FU] in 1 patient; FU + oxaliplatin in 3 patients). Duration from surgery to adjuvant chemotherapy was 68 days (range, 52–76 days). Sites of recurrence were the paraaortic lymph nodes, lungs, and liver in 1 patient each. Two patients experienced local recurrence. Time from surgery to recurrence was 10 months (range, 5–26 months). With regard to treatment after recurrence, 4 patients received systemic chemotherapy and 1 patient underwent surgery.
DISCUSSION
Our results showed that combined transabdominal and transperineal endoscopic PE offered good perioperative outcomes, including low blood loss and a low complication rate. All patients achieved complete R0 resection. Furthermore, the procedure performed using a 2-team approach (abdominal and perineal teams simultaneously) shortened operation time and decreased blood loss and blood transfusion compared to the 1-team approach. To the best of our knowledge, this is the first study to investigate the safety, feasibility, and oncological outcomes of combined transabdominal and transperineal endoscopic PE.
PE includes en bloc removal of the rectum with bladder and reproductive organs for the purpose of complete R0 resection [17]. However, patients who underwent the procedure often experienced excessive stress, long operation time, high blood loss, delayed postoperative recovery, and high morbidity rates [1819]. These days, laparoscopic surgery has become popular for colorectal malignancies due to the reduced invasiveness compared to open surgery [67].
Some recent studies have investigated the feasibility of laparoscopic PE [911]. Ogura et al. [9] examined the safety and feasibility of laparoscopic PE in patients with colorectal cancer. Estimated blood loss (930 mL vs. 3,003 mL, P = 0.001) and volume of blood transfusion (0 mL vs. 1,990 mL, P = 0.002) were significantly lower in patients undergoing laparoscopic PE than in patients undergoing open PE. Operation time (829 minutes vs. 875 minutes, P = 0.660) and proportion of postoperative complications (61.5% vs. 83.3%, P = 0.171) were similar between groups. They concluded that laparoscopic PE could represent a safe and preferred option with significant advantages in terms of reducing blood loss. However, laparoscopic approaches are sometimes difficult in cases with a narrow pelvis, bulky tumor, male sex, or obesity, due to restrictions placed on handling instruments in the deep pelvic space [20]. In terms of laparoscopic PE, patients often have large tumors with invasion to surrounding organs. In the present cases, most patients (10 patients, 71.4%) showed tumors of >90 mm in maximum diameter.
To overcome these restrictions, we performed the transperineal endoscopic approach along with the transabdominal approach. The transperineal approach is an extension of the conventional abdominal approach used for lower rectal surgery [20]. Surgeons using this approach from a “down-to-up” direction could perform deep pelvic dissection despite the aforementioned obstacles. As a result, we were able to reduce inadequate plane dissection and unnecessary blood loss, which could have contributed to the reduced rates of postoperative complications. A recent meta-analysis showed that the transperineal approach for rectal surgery offers advantages in the form of the same circumferential resection margins, reduced blood loss, shorter hospital stay, and lower postoperative complication rates [20].
Transperineal endoscopic PE has potential with regard to safe R0 resection. Despite recent advances in neoadjuvant chemotherapy and careful preoperative patient selection, the R0 resection rate of PE remains unsatisfactory, in the range of 41.7%–90.2% [5]. Control of intraoperative bleeding enables the surgeon to dissect the appropriate layer, which can facilitate completion of R0 resection. In transperineal endoscopic PE, the surgeon can detect fine vessels and stop bleeding as soon as this occurs under high-definition and magnified visualization, especially for angiogenesis around the main tumor. Furthermore, high pneumoperitoneal pressure could reduce small venous oozing. Management of the DVC is an important point for controlling total blood loss in total PE. Dissection of the DVC from an abdominal approach is sometimes difficult to address due to huge pelvic tumors. With the transperineal approach, we could handle the DVC under close visualization and an appropriate angle, making the DVC easy to divide using only energy devices.
Recurrent rectal cancer is a major indication for PE and represents a risk factor for margin-positive resection due to severe fibrosis around the tumor [21]. A transperineal approach for recurrent cancers could start dissection from an untouched area, avoiding effects from the primary surgery. A multidirectional approach could help maintain a proper dissection layer, resulting in reduced intraoperative bleeding and successful R0 resection.
In this study, total blood loss (median, 618 mL; range, 130–1,660 mL) was broadly similar to that of previous laparoscopic PE (median, 400–830 mL) and lower than that of previous descriptions of open PE (median, 875–2,769 mL) [91022]. In addition, all patients (including 2 patients [14.3%] with recurrent cancer) achieved R0 resection.
The present study compared laparoscopic PE performed by a transabdominal team and a transperineal team working simultaneously (2-team approach) with that performed separately (1-team approach). The 2-team approach offers several benefits not seen with the 1-team approach. First, cooperative surgery shortens the dissection time, shortening the total operation time compared with the 1-team approach, and thus reducing accumulated bleeding. When the abdominal and pelvic cavity become one, with the achievement of the socalled “rendezvous,” the 2 teams can work together to facilitate exposure of the appropriate operation field, decreasing surgeon fatigue and stress. Unexpected bleeding that is difficult to control from one side may prove controllable by the other team. Cooperation in tissue exfoliation, development of the operation field, and bleeding control could overcome the drawbacks of laparoscopic PE. Previous case reports have revealed benefits for appropriate dissection and reduced bleeding from 2-team procedures for extended pelvic surgery [1623]. In our study of laparoscopic PE, the 2-team approach contributed to shorter operation time, lower blood loss, lower blood transfusion, and appropriate dissection.
In a previous meta-analysis, intraoperative stress on the surgeon was increased with longer operation time, bleeding, and less communication [24]. From the results in this study, we speculate that a comprehensive 2-team approach would reduce stress on the surgeon. Objective data on surgeon stress need to be measured to clarify the influences of the approach on operator stress [2526].
On the other hand, a key problem of the cooperative 2-team approach is the need for more personnel compared to the 1-team approach. The procedure is thus more expensive, and the operation field often becomes crowded. Recently, a case series of robot-assisted anterior PE was reported [27]. They observed operation time and length of hospital stay were similar to those of conventional laparoscopic surgery. However, robotic PE reduced the amount of blood loss, with no patients needing blood transfusion. They also showed that robotic PE provided good prognosis with no positive margins. Atallah et al. [28] reported a new robotic system for dual-field synchronous transanal total mesorectal excision (TME) in a preclinical model. Because robotic surgery minimizes the need and roles for an assistant, the 2-team approach could reduce personnel to only the 2 console surgeons along with a surgical assistant or expert scrub nurse. These new promising options could overcome the drawbacks of synchronous 2-team PE.
The present study had some limitations that merit consideration. First, this was a retrospective, nonrandomized study with a small number of patients. In this study, although operation time was shorter in the 2-team approach, morbidities and hospital stay were the same between the 2 approaches. One possible explanation is that the number of patients was relatively small. Another explanation is that several hospitals in areas of different characteristics participated in this study, including both high-volume and low-volume centers. The duration of hospital stay also varied between hospitals. Second, the transperineal approach showed a prolonged learning curve because of the differences in anatomical recognition. Recent studies of the transanal TME learning curve revealed that institutional proficiency was achieved after over 40 cases [2930]. Furthermore, a recent study showed that time to recurrence was short, at a median of 11 months after transanal TME. They described an increased rate of local recurrence after transanal TME due to the learning curve regarding technical problems [31]. In the present study of patients at a more advanced stage, 5 patients (35.7%) experienced recurrence. Among those, 2 patients (14.3%) showed local recurrence. Training using a structured curriculum is crucial for transperineal surgery [32]. Third, in this study, performance of the 2-team approach was limited to hospitals with experienced surgical teams and sufficient staffing. A prospective, randomized study is required to overcome these selection biases. To generalize the 2-team approach, surgeons must first accumulate experience with transperineal surgery. Novel approaches including robotic surgery could overcome staffing problems in the future [25].
Despite these limitations, we concluded that combined transabdominal and transperineal endoscopic PE using a synchronous 2-team approach represents a feasible, safe procedure with the potential to reduce operation time, blood loss, and stress on the surgeons.

 XML Download
XML Download