

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As one of the most common digestive malignant tumors, gastric cancer accounts for about 5.7% of the total cancer cases according to the GLOBOCAN 2018 data [1]. Although the survival of some patients with gastric cancer improved with the advancement of the therapeutic methods, those patients at a later stage of cancer continue to have a poor prognosis [2]. Therefore, finding effective prognostic indicators for these patients could help clinicians make proper treatment decisions.
Currently, some serum tumor indicators such as CA 125, CA 153, CA 19-9, and CEA have been applied to assess the diagnostic and prognostic values in patients with gastric cancer. For example, the elevation of CA 19-9 level was correlated with female sex and presence of lymph node metastasis in gastric cancer, and elevation of CEA level was an independent risk factor for poor prognosis of early gastric cancer [3]. However, these indicators were subject to low sensitivity and specificity for different stages of cancer [34]. In addition, some novel indicators calculated from conventional biomarkers, such as neutrophil lymphocyte ratio (NLR) [56], platelet lymphocytes ratio (PLR) [7], and CRP/albumin ratio (CAR) [89], have been reported to enhance the prognostic values in patients with various cancers. Among these indicators, the clinical significance and prognostic value of CAR in gastric cancer continue to require further elucidation.
CAR is a novel inflammation-based prognostic indicator; the high value of CAR was associated with poor outcome in various diseases, including sepsis [10], pancreatitis [11], and some cancers [12]. The prognostic value of CAR in patients with gastric cancer has also been explored [131415]. However, the robustness of previous studies still requires validation through further studies. Therefore, in order to derive a more precise assessment of the prognostic value of CAR in gastric cancer, we analyzed the data of gastric cancer and combined our data with previous data, which may further verify the role of CAR in gastric cancer.
Go to : 
METHODS
Selection of gastric cancer patients
The data of patients with gastric cancer who underwent surgery was retrospectively analyzed at the Guangxi Medical University Cancer Hospital (Guilin, China) between January 2015 and October 2019. Inclusion criteria are (1) diagnosis of gastric cancer was confirmed histologically and (2) all gastric cancer patients underwent surgical treatment. Patients with autoimmune diseases, infectious diseases, severe hematologic diseases, or major organ failure were excluded. This study was approved by the Ethics Committee of the Guangxi Medical University Cancer Hospital with a waiver for informed consent (No. KY2020015).
Data collection and calculation
The clinical features of gastric cancer were collected including patient age, sex, tumor location, differentiation grade, and TNM stage. TNM stage was defined based on the American Joint Committee on Cancer criteria, 8th edition [16]. Preoperative laboratory blood parameters, such as CRP, albumin, neutrophil, lymphocytes, platelet, and the tumor biomarkers (CEA, CA125, CA153, and CA 19-9) were collected. The NLR, PLR, and CAR were calculated. Overall survival (OS) was calculated from the date of surgery to the date of death or last follow-up.
Statistical analysis
Continuous data was presented as a median and interquartile range from 25th to 75th percentile. Mann-Whitney U-test or Student t-test were used to compare continuous variables between the 2 groups when appropriate. The chi-square test was applied to categorical variables between groups. Kaplan-Meier curve and the log-rank test were used to evaluate the survival time between the 2 groups. Cox regression analysis was employed to identify the prognostic indicators in patients with gastric cancer. The receiver operating characteristic (ROC) curve and the area under the curve (AUC) was conducted to assess the prognostic value of CAR. All statistical tests were 2-sided and P-values of <0.05 were considered statistically significant. The statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Corp., Armonk, NY, USA) and R ver. 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Meta-analysis for the data
The performance of meta-analysis on the prognostic value of CAR in gastric cancer was conducted as in our previous study [17]. Briefly, the relevant articles were retrieved and assessed from the databases (PubMed, Web of Science, and Chinese National Knowledge Infrastructure before October 2020, using “C-reactive protein/albumin ratio,” “CAR,” or “gastric cancer” as search terms) based on certain criteria and the data of these articles (author's name, number of patients, cutoff value of CAR, stage of cancer, follow-up and hazard ratio [HR] values for survival) was extracted. The differences among the subgroups were assessed using meta-regression analysis. The random-effects model (DerSimonian-Laird method) was used to combine the HRs if there was significant heterogeneity across the studies; otherwise, a fixed-effects model (Mantel-Haenszel method) was conducted. R ver. 3.5.1 was used to conduct the meta-analysis. The P-values of <0.05 were considered statistically significant.
Go to :
RESULTS
Clinical characteristics of the study populations
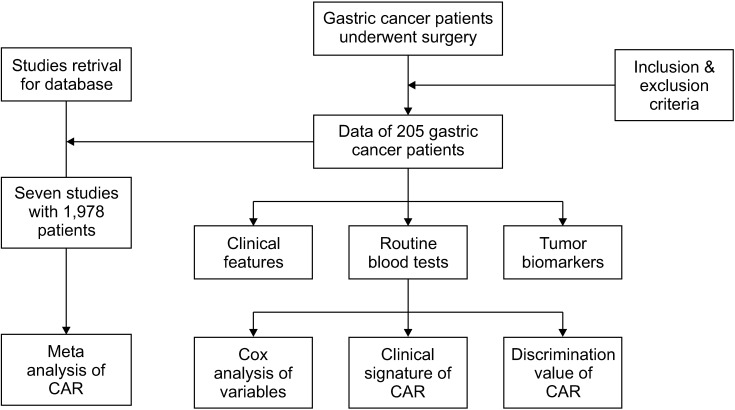
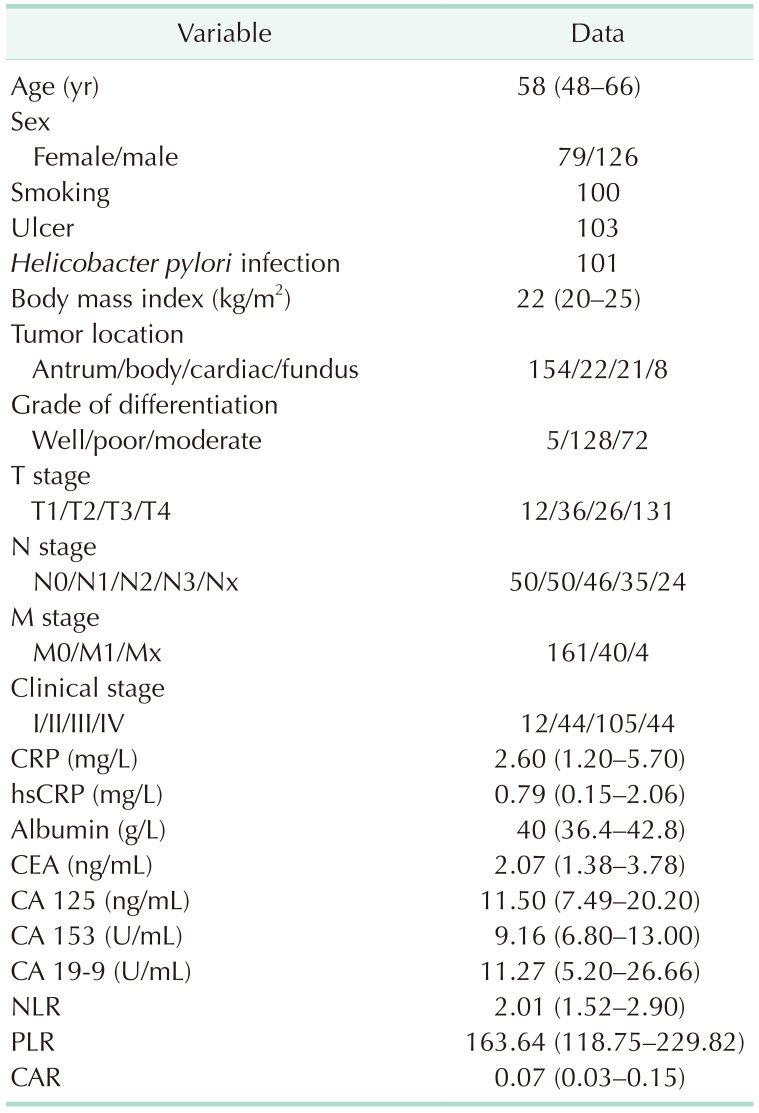
The patient selection flow chart is shown in Fig. 1. A total of 205 patients with gastric cancer who underwent surgical treatment were finally selected in this study. The median age of the patients was 58 years. The median follow-up was 44 months (1–64 months). All of 124 patients were alive and 81 patients dead during the follow-up period. The details of patients with gastric cancer are listed in Table 1.
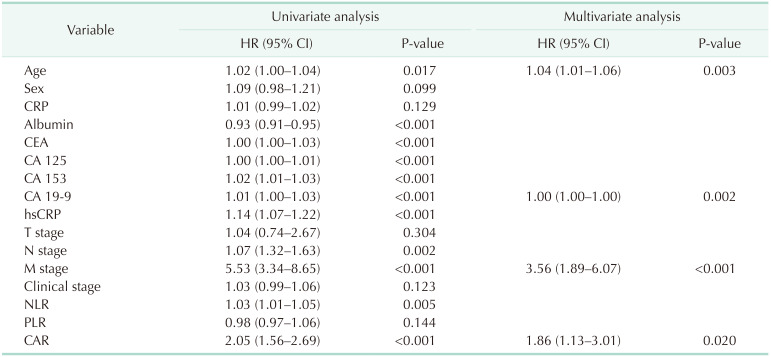
Univariate and multivariate Cox regression analysis for the clinical features
The univariate Cox regression analysis was performed by including the clinical features, including patient sex, age, histological grade, TNM stage, and laboratory variables. The results showed that patients' age, CEA, CA 125, CA 153, CA 19-9, high-sensitivity CRP, N stage, M stage, NLR, and CAR were significantly associated with the survival of patients with gastric cancer. Then, the multivariate Cox regression analysis for these variables showed that patient age (HR, 1.04; 95% confidence interval [CI], 1.01–1.06), M stage (HR, 3.56; 95% CI, 1.89–6.07), and CAR (HR, 1.86; 95% CI, 1.13–3.01) were considerably associated with the survival in patients with gastric cancer (Table 2).
Survival analysis and prognostic value of CAR in patients with gastric cancer
Using the median value as cutoff (CAR, 0.022), the Kaplan-Meier curve and log-rank test revealed that, patients with high values of CAR have shorter survival time than those with low values (Fig. 2A). We next determined the prognostic value of CAR in gastric cancer patients in different survival times, and found that CAR has a good performance in predicting the 1-, 3-, and 5-year survival in patients with gastric cancer, with the AUC as 0.758, 0.742, and 0.787, respectively (Fig. 2B). In order to evaluate the effect of different stage of cancer on the prognostic value of CAR, we conducted subgroup analysis by dividing the patients into 3 subgroups based on the clinical stage (stage I, stage II + III, and stage IV), and the results failed to show that CAR was associated with the prognosis of patients in these subgroups (P > 0.05).
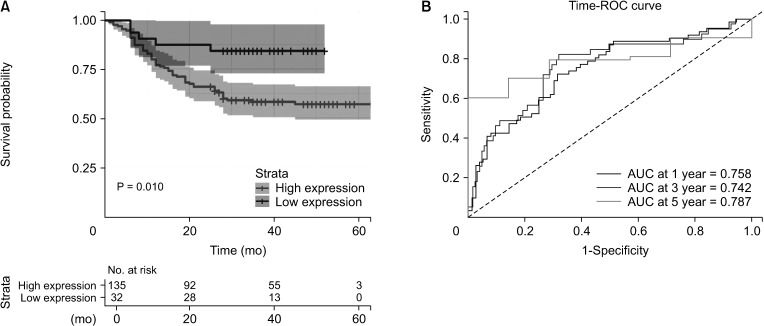 | Fig. 2(A) Kaplan-Meier curve for the CRP/albumin ratio (CAR) in patients with gastric cancer using median value as a cutoff. (B) The prognostic value of CAR in predicting the 1-, 3-, and 5-year survival in patients with gastric cancer. ROC, receiver operating characteristic; AUC, area under the curve.
|
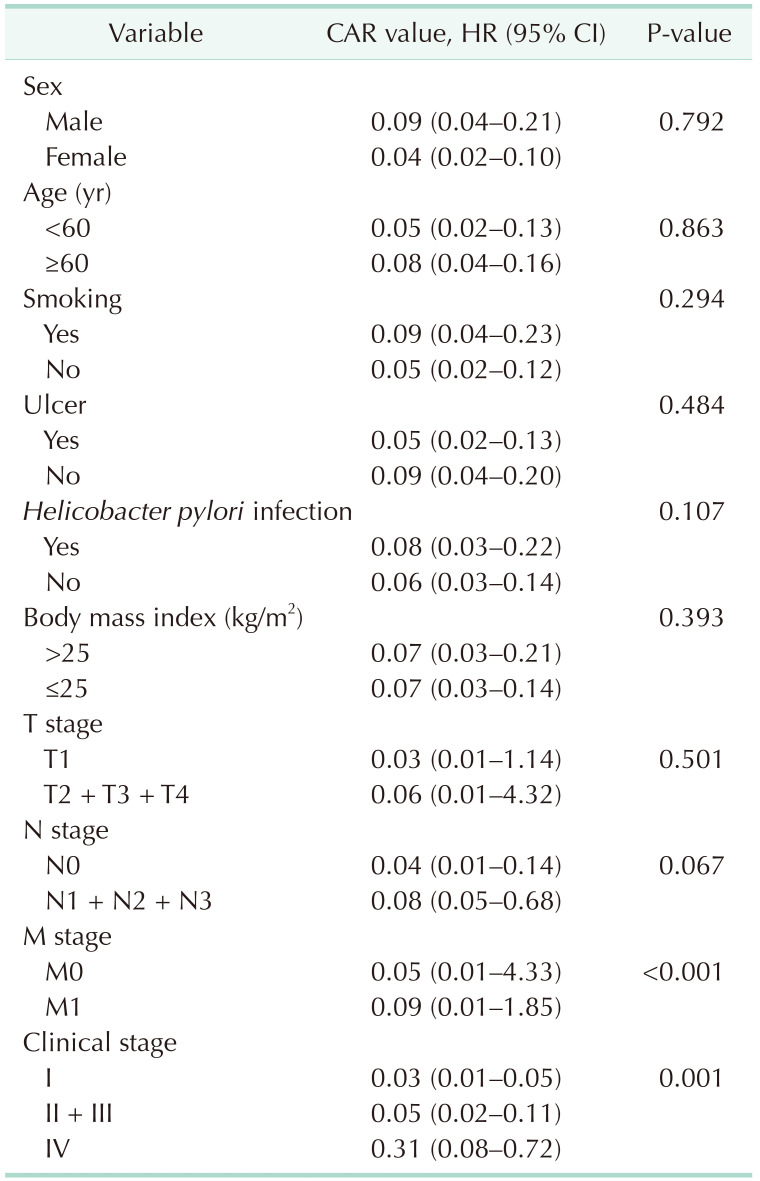
Association of CAR with the clinical features in gastric cancer
The association of CAR with the clinical features of gastric cancer, including patient's age, sex, histological grade, TNM stage, and clinical stage, were analyzed, respectively. As Table 3 showed, CAR value was remarkably increased in patients with M1 stage compared with M0 stage (P < 0.001), and elevated in stage IV compared with stage I and stage II + III (P = 0.001); however, no obvious differences were observed between CAR and other clinical features (P > 0.05).
Discrimination value of CAR in different M stage of gastric cancer
Since there was a significant difference of CAR value in M stage and clinical stage of patients, we further evaluated the discriminate value of CAR in M stage and clinical stage of gastric cancer; the ROC method was used to calculate the AUC of CAR. As Fig. 3 illustrates, CAR could reach a high predictive value in different M stage with the AUC value of 0.809, and the predictive value in the different clinical stage was moderate with the AUC value of 0.679.
 | Fig. 3Discriminated value of C-reactive protein/albumin ratio (CAR) in different TNM stage of gastric cancer. (A) M stage (M0 vs. M1; cutoff: 0.357). (B) Clinical stage (I vs. II + III + IV; cutoff: 0.048). ROC, receiver operating characteristic; FPR, false positive rate; TPR, true positive rate; AUC, area under the curve.
|
Meta-analysis for the prognostic value of CAR in gastric cancer
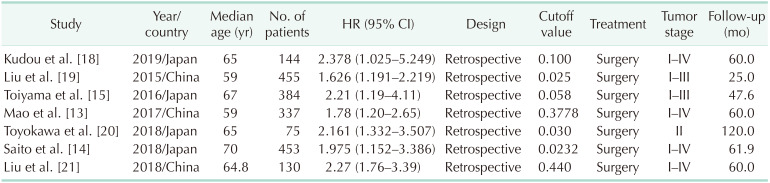
Seven studies [13141518192021] with 1,978 patients that evaluated the prognostic value of CAR in patients with gastric cancer were included in the meta-analysis. The details of included studies are listed in Table 4. All the data of CAR in predicting the prognosis of patients was extracted from multivariate Cox regression. By combing these data with our data, we found that CAR was significantly associated with the survival of patients with gastric cancer (HR, 1.94; 95% CI, 1.67–2.27; Mantel-Haenszel method, I2 = 0, P heterogeneity = 0.891) (Fig. 4A). The subgroup analysis by dividing the cutoff value into <0.1 or >0.1 showed that both of CAR with different cutoff value have significant prognostic value in gastric cancer (both P < 0.05, Mantel-Haenszel method). Meta-regression analysis revealed that no significant difference between these 2 subgroups (P > 0.05) (Fig. 4B), suggesting that different cutoff value did not affect the prognostic value of CAR in patients with gastric cancer. No publish bias was found across these studies (P > 0.05).
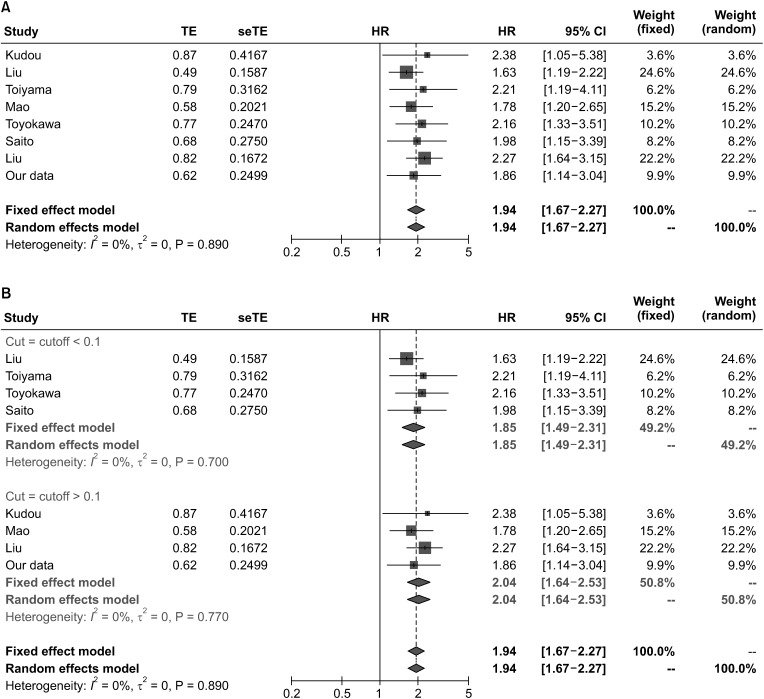 | Fig. 4Forest plot of the Meta analysis. (A) Forest plot of hazard ratio (HR) for the association of CRP/albumin ratio (CAR) with overall survival (OS) in patients with gastric cancers. (B) Forest plot of HR for the association of CAR with OS in gastric cancers with different cutoff values. TE, treatment estimate; seTE, standard error of TE; CI, confidence interval.
|
Go to :
DISCUSSION
The development and progression of cancer is a complicated process, and many factors have been contributed to gastric carcinogenesis. Among them, systemic inflammatory response and nutritional status are 2 important contributors [22]. Evidences showed that CAR was an important inflammation-based prognostic indicator that was associated with the survival of various cancers [2324]. In the present study, we found that CAR was an important prognostic indicator in patients with gastric cancer, which was in agreement with previous studies [131421]. We also found that CAR has a higher prognostic value in predicting the 1-, 3- and 5-year survival of patients. In agreement with previous studies [131521], our results showed that CAR was associated with M stage and clinical stage of gastric cancer, and the discriminate value for the different M stage was higher, suggesting that the CAR might be used to differentiate the M stage of gastric cancer.
Serum CRP is an acute-phase protein and reported to be a sensitive prognostic indicator in a variety of inflammatory diseases and cancers [2526]. A study has shown that reduction of CRP as an early predictor of postoperative complications and a reliable discharge indicator after gastrectomy for gastric cancer [27]. On the other hand, serum albumin level is an indicator of body nutrition status, low albumin level indicates a malnutrition status and often second to patients with gastrointestinal cancers, especially those at an advanced stage [2829]. CAR is calculated based on both serum CRP and albumin level, which is more reliable than single one in predicting the outcome of the malignancy [30]. Although other inflammation-based prognostic indicators, such as NLR and PLR, have been shown to associate with the prognosis in patients with gastric cancer, the present study failed to confirm the prognostic value of them by using multivariate Cox regression analysis. CAR also reflects immune and nutritional status of the patients, while other prognostic indicators such as prognostic nutritional index (PNI) were also found to be associated with the prognosis of the patients with cancers. A previous study reported a comparison of CAR with PNI in 363 cancer and non-cancer patients which showed that PNI and CAR were both useful to predict the long-term survival of patients. Moreover, CAR has better performance than PNI in predicting the short-term survival of patients. These results suggest that these indicators might not stable in predicting the survival of patients with gastric cancer compared with CAR.
TNM stage is one of the most important criteria in predicting the prognosis of patients with various cancers, and many studies reported that inflammation-based prognostic indicators, including NLR, PLR, and CAR, were associated with the TNM stage in gastric cancer. For example, Toiyama et al. [15] reported that CAR was significantly increased in gastric cancer with lymph node metastasis and poor differentiation. Liu et al. [19] observed that CAR was associated with the lymph node metastasis and clinical stage of gastric cancer. A similar result was found in the report of Mao et al. [13]. However, in the present study, we failed to show the association with the clinical features, including the TNM stage, which was similar to the report by Saito et al. [14], indicating that the change of CAR might be independent of the TNM stage. Moreover, our results showed that CAR has a moderate value in discriminating the M stage (M0 and M1) and clinical stage (I and II + III + IV), which may help to identify the patients who are at high risk and provide them proper treatment. In this study, the results indicated that only M stage, but not T stage or N stage, was as in independent prognostic factor in predicting the prognosis of patients. We speculated that the relative sample size might explain these results, and a larger cohort is necessary to verify these results.
As in other studies, our results were based on a single center, which may be subject to several limitations. In order to achieve a more robust conclusion, we conducted a meta-analysis by combing our data with previous studies. As shown from the meta-analysis, including 7 studies with larger gastric cancer patients, CAR was shown to be significantly associated with the survival of patients with gastric cancer, which further confirmed the prognostic value of CAR in these patients. Unlike other novel prognostic biomarkers, CRP and albumin are routine laboratory tests using blood samples in clinical practice. Thus, the results of CAR can be obtained easily and do not add extra costs to the patients, making it an attractive biomarker for the prognosis of gastric cancer. For instance, a patient with high CAR should be considered for surgery or added necessary adjuvant chemotherapy. In addition, the follow-up interval after treatment must be shorter compared with those of low CAR values. Therefore, CAR could be considered as an indicator of simplicity, cheapness, and easy availability in clinical settings.
However, we acknowledged several limitations in the present study, which might reduce the robustness of the conclusion. First, our study was a retrospective design, single-center study, which potentially leads to selection bias. Second, many factors affect the serum levels of CRP and albumin, but we could not adjust these confounding factors in this study. Third, the postoperative therapy was different across the patients, which might also induce bias. Fourth, American Society of Anesthesiologists and Eastern Cooperative Oncology Group were important indicators used to evaluate the patient's condition before surgery; however, due to lack of data in our center, we could not analyze the relation of these scores with the CAR. Therefore, a future larger-scale study with prospective design by addressing the aforementioned issues is warranted to validate our findings.
In conclusion, the present study demonstrates that preoperative CAR is associated with the prognosis of patients with gastric cancer after surgery, which may help to provide proper treatment for patients.
Go to :
 XML Download
XML Download