

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Total pancreatectomy (TP) is a rare surgical procedure performed only when the disease involves the entire pancreas and no other surgical options are available [12]. Recent studies have reported that mortality and morbidity after TP are comparable to those after partial pancreatectomy [34], and increasing evidence has confirmed its safety [56]. Moreover, TP eliminates postoperative pancreatic fistula, among the most severe complications of partial pancreatectomy [7]. Despite these optimistic findings, surgeons are reluctant to perform TP because of the challenges of postoperative care caused by the complete loss of exocrine and endocrine functions [589] and the poor nutritional status and poor quality of life (QoL) that follow [10111213].
It is well known that lifelong medical treatment and self-management of pancreatic insufficiency are required in TP patients, leading to a substantial impact on QoL [1415]. Advancements in high-dose pancreatic enzyme replacement therapies and education on dietary changes have improved the management of pancreatic exocrine insufficiencies [1617]. Diabetes mellitus (DM) caused by endocrine function insufficiency has been explored to a great extent, and endocrinologists have presented optimal glycemic control treatment strategies with evidence of new insulin formulations, antihyperglycemic medications, and glucose monitoring methods [18]. However, compared to the numerous studies on endocrine function insufficiency, prospective studies are lacking on the consequences of exocrine insufficiency and changes in patient-based QoL and nutritional status that results after TP.
Therefore, this study aimed to prospectively evaluate the short- and long-term consequences of pancreatic exocrine insufficiency after TP as well as nutritional status changes and their associated effects on QoL.
Go to : 
METHODS
Study design
Patients who underwent elective single-stage TP at Seoul National University Hospital between 2008 and 2018 were selected for the study, and those with at least a 1-year follow-up were considered eligible. Excluded were those who underwent remnant TP and those who expired within 1 year after surgery. All patients were prescribed a pancreatic enzyme dose of 40,000–80,000 units and given nutritional education prior to discharge. Insulin dose was determined and titrated with the help of endocrinologists, and after 1-month follow-up or until the dose stabilized, most of the patients continued DM or glycemic control management at clinical centers near their place of residence. The Institutional Review Board at Seoul National University Hospital granted approval of the data collection, storage, and analysis procedures (SNUH 1305-016-486). Written informed consent was obtained.
Data sources and questionnaires
Data were collected prospectively, once preoperatively and at 3 and 12 months postoperatively. Exocrine function, endocrine function, and nutritional status were assessed by the following measurements. Bowel movement frequency was measured to assess exocrine pancreatic function. Nutritional status was evaluated using the Mini Nutritional Assessment (MNA) questionnaire [19] and by measuring relative body weight (RBW), triceps skinfold thickness (TSFT), and serum levels of protein, albumin, and transferrin. The endocrine function was assessed by hemoglobin A1c (HbA1c).
Validated questionnaires were also administered once preoperatively and at 3 and 12 months postoperative. The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30, ver. 3.0) [20], a multidimensional measure containing 30 questions investigating global health status (GHS) and functional symptoms, was employed to assess QoL. The additional pancreatic cancer module (EORTC QLQ-PAN26) [21] was used to assess pancreatic cancer-specific symptoms. Raw scores, the mean of the component items, on the EORTC QLQ-C30 and PAN26 underwent a linear transformation for standardization. Higher scores on the GHS and functioning scales represent better QoL, whereas higher scores on the symptom scale represent more serious symptoms or poorer QoL.
Statistical analysis
Changes in the different values over time were evaluated using repeated-measures analysis of variance. The results are presented as mean ± standard deviation. Two-tailed values of P < 0.050 were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows, ver. 25.0 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
Patient characteristics
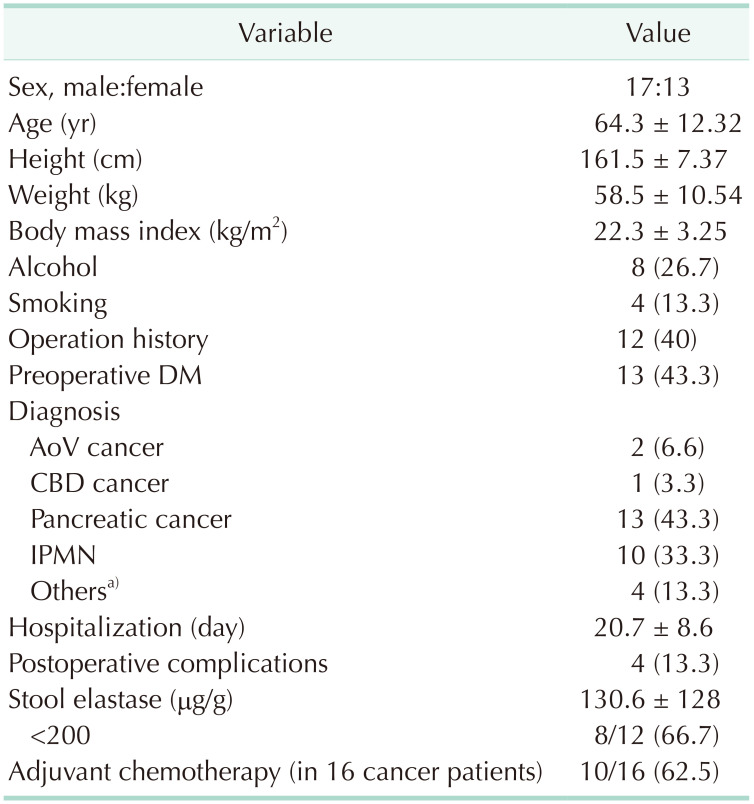
Between 2008 and 2018, a total of 39 patients underwent TP at Seoul National University Hospital. Of them, 4 who underwent remnant TP and 5 who expired within 1 year after surgery were excluded. Three of the 5 patients expired due to disease progression within 1 year after surgery, and the remaining 2 patients died from surgery-related septic shock and liver failure, respectively. Thus, 30 patients who underwent TP were eligible for the study.
The mean patient age was 64.3 years and 17 (56.7%) were male. The mean body weight immediately before surgery was 58.5 kg, while the mean body mass index was 22.3 kg/m2. Of the total 30 patients, 13 (43.3%) had preoperative DM. A stool elastase level < 200 µg/g, which indicates pancreatic exocrine insufficiency, was apparent in 8 of the 12 patients (66.7%) in whom it was determined before surgery; the mean preoperative stool elastase level was 130.6 µg/g. The final pathological diagnosis consisted of 13 pancreatic cancers, 10 intraductal papillary mucinous neoplasms (IPMN), 2 ampullae of Vater (AoV) cancers, 1 common bile duct (CBD) cancer, and 4 noncancerous lesions. Of the 2 patients diagnosed with AoV cancer; 1 underwent TP because of concomitant IPMN, while the other did so because cancer had spread along the main pancreatic duct. The patient diagnosed with CBD cancer underwent TP due to severe pancreatitis that was considered too high risk for pancreatojejunostomy leakage. The other lesions consisted of one mucinous cystic neoplasm, 2 serous cystic neoplasms, and 1 grade-2 neuroendocrine tumor (NET). The patient with NET underwent TP due to positive margins on a frozen section biopsy, and the rest due to huge masses. Postoperative complications occurred in 4 of 30 patients (13.3%), including 2 surgical wound problems; 1 bleeding ulcer, and 1 marginal ulcer. Ten out of 16 cancer patients underwent adjuvant chemotherapy. Patient demographics are shown in Table 1.
Changes in exocrine function
Changes in parameters associated with exocrine function over time are shown in Fig. 1. The RBW was highest preoperatively and decreased significantly over time after surgery (P < 0.001) (Fig 1A). Bowel movement frequency increased over time from 1.96 times per day preoperatively to 3.05 times per day at 1 year after surgery, which meets the definition of diarrhea (Fig. 1B). The mean MNA score was lowest preoperatively, peaked at 3 months of follow-up, and then decreased almost to the preoperative state by 1 year of follow-up (Fig. 1C). The mean TSFT started at 11.1 mm before surgery but decreased to 7.83 mm and 8.13 mm at 3 months and 1 year of follow-up, respectively (Fig. 1D).
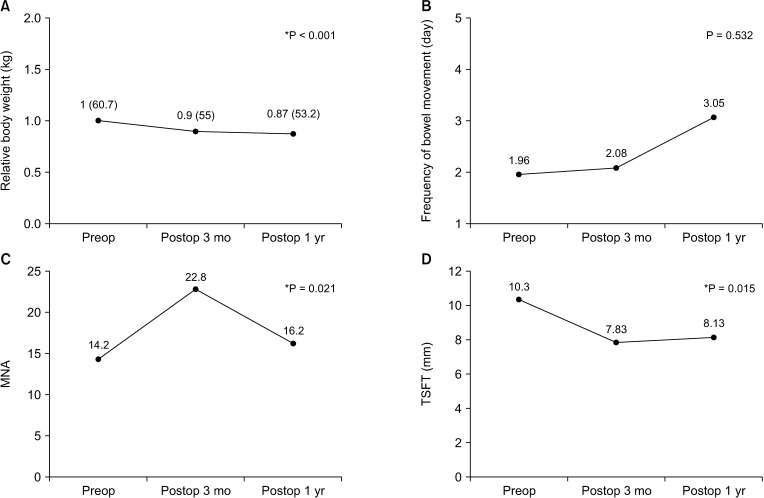 | Fig. 1Changes in exocrine function. (A) Relative body weight was highest preoperatively and continued to decrease over time. (B) Bowel movement frequency increased over time. (C) Mini Nutritional Assessment (MNA) score was lowest preoperatively, peaked at 3 months of follow-up, and then decreased almost to the preoperative state by 1 year of follow-up. (D) Triceps skinfold thickness (TSFT) decreased significantly after surgery. Preop, preoperative; Postop, postoperative. *P < 0.050.
|
Changes in nutritional parameters
Changes in the nutritional parameters over time are shown in Fig. 2. Protein, albumin, and transferrin levels did not differ significantly over time. Although the difference was very small, protein and albumin levels were highest at 3 months of follow-up but decreased to preoperative levels by 1 year of follow-up (Fig. 2A, B). Transferrin levels, on the other hand, was lowest at 3 months of follow-up but increased past the preoperative level at 1 year of follow-up (Fig. 2C).
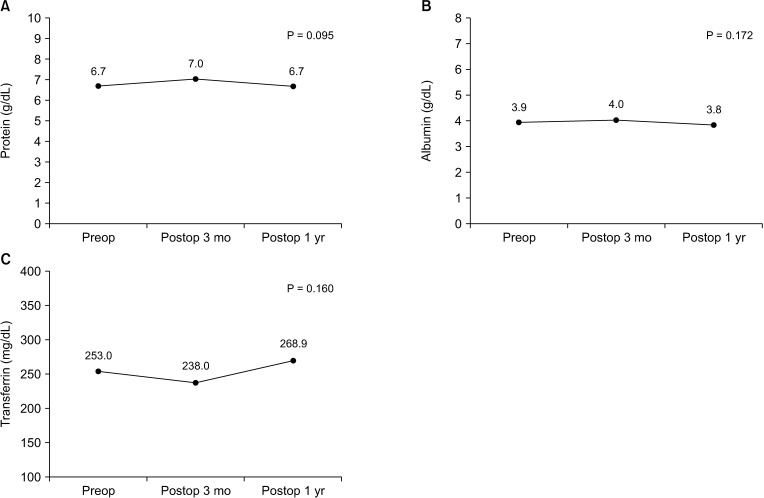 | Fig. 2Changes in nutritional parameters. (A) Protein was highest at 3 months of follow-up but decreased to preoperative levels by 1 year of follow-up. (B) Albumin was highest at 3 months of follow-up but decreased to preoperative levels by 1 year of follow-up. (C) Transferrin was lowest at 3 months of follow-up but increased past the preoperative levels at 1 year of follow-up. Preop, preoperative; Postop, postoperative.
|
Changes in endocrine function
The change in endocrine function, represented by the HbA1c over time, is shown in Fig. 2. The mean HbA1c was 7.2% before TP, and although not statistically different, it increased slightly to 7.9% at 3 months of follow-up and remained at this level until 1 year of follow-up.
Changes in quality of life
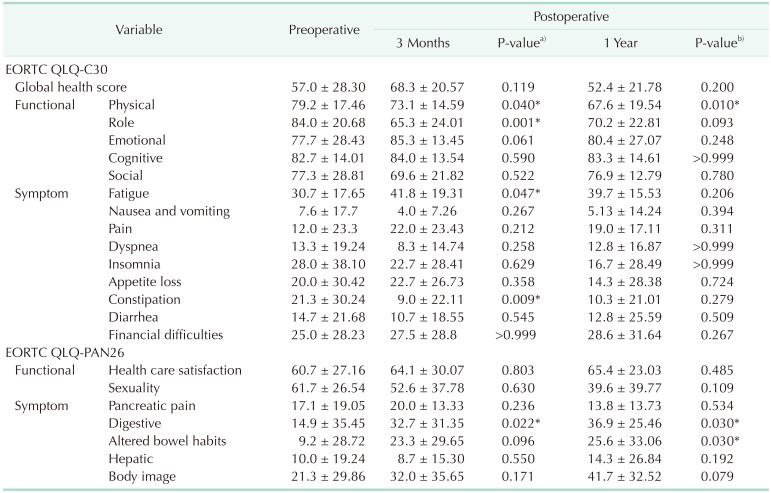
The GHS score and each of the QoL categories, measured by the EORTC QLQ-C30 and PAN26, are summarized in Table 2, while the changes over time are shown in Fig. 3.
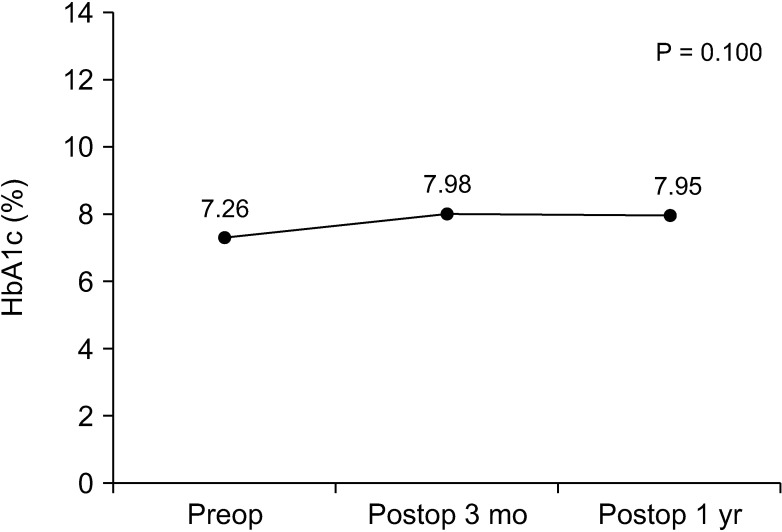 | Fig. 3Changes in endocrine function. Hemoglobin A1c (HbA1c) increased slightly at 3 months and was maintained at this level until 1 year of follow-up. Preop, preoperative; Postop, postoperative.
|
Table 2
Change in patient quality of life
Values are presented as mean ± standard deviation.
EORTC QLQ-C30, European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-PAN26, EORTC QLQ pancreatic cancer module.
a)Comparison of perioperative patients and 3 months postoperative patients; b)comparison of perioperative patients and 1 year postoperative patients.
*P < 0.050 (paired t-test).
![]()
At 3 months after undergoing TP, the GHS showed no significant difference (preoperative, 57.0 vs. 3 months postoperative, 68.3; P = 0.119). The physical function score (79.2 vs. 73.1, P = 0.040) and role function score (84.0 vs. 65.3, P = 0.001) decreased with statistical significance. Patients also presented with worsened symptoms of fatigue (30.7 vs. 41.8, P = 0.047), constipation (21.3 vs. 9.0, P = 0.009), and digestive difficulties (14.9 vs. 32.7, P = 0.022) (Table 2).
By 1 year postoperative, the GHS still showed no significant difference (preoperatively, 57 vs. 1 year postoperatively, 52.4; P = 0.200), and no statistically significant differences were seen in most of the QoL categories. However, poor physical function (79.2 vs. 67.6; P = 0.010) continued even 1 year after surgery. All of the symptoms in the EORTC QLQ-C30 that were significant at 3 months were resolved 1 year after surgery, and the only statistically significant symptoms that persisted on the pancreatic cancer-specific PAN26 module were digestive difficulties (14.9 vs. 36.9; P = 0.030) and altered bowel habits (9.2 vs. 25.6; P = 0.030) (Table 2).
Most of the QoL scores that had decreased at 3 months postoperative significantly improved to postoperative levels by 1 year postoperative. However, symptoms that did not improve even after 1 year postoperative, including digestive difficulties and altered bowel habits, were attributed to pancreatic exocrine function insufficiency (Fig. 4).
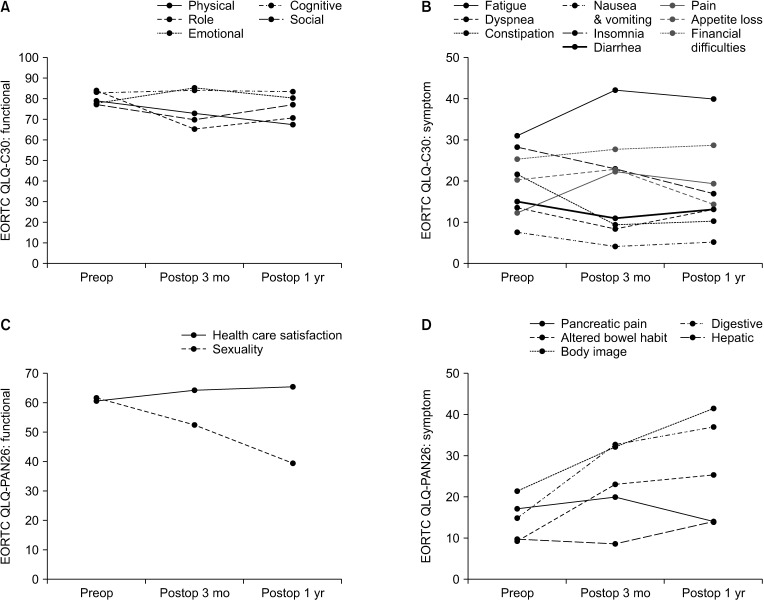 | Fig. 4Changes in quality of life. (A) EORTC QLQ-C30 functional scores showed that the physical function and role function scores decreased at 3 months of follow-up, whereas the role function score recovered after 1 year of follow-up while the physical function score worsened. (B) EORTC QLQ-C30 symptom scores showed that fatigue and constipation worsened at 3 months of follow-up but recovered at 1 year of follow-up. (C) EORTC QLQ-PAN26 functional scores showed no significant differences, but the trend of the sexuality scores seemed to decrease over time. (D) EORTC QLQ-PAN26 symptom scores showed that digestive and altered bowel habit symptoms continued to worsen over time. EORTC QLQ-C30, European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-PAN26, EORTC QLQ pancreatic cancer module; Preop, preoperative; Postop, postoperative.
|
Go to :
DISCUSSION
Many studies have already shown that postoperative outcomes after TP and pancreatoduodenectomy are comparable [34]. Hence, the chief concern in extending resection to the entire pancreas is associated with the inevitable consequences brought about by the apancreatic state. QoL is becoming increasingly important to clinical decision-making in even the most aggressive diseases and in settings in which life expectancy is short. Moreover, studies have shown that QoL is a significant predictor of cancer survival above and beyond demographic and medical factors [2223]. This study assessed which factors affect QoL after TP and to which extent they impact patient QoL over time. Many of the symptoms after TP worsen significantly after 3 months postoperative but then improve to a comparable level at 1 year postoperative. However, poorer physical function and nutrition and symptoms associated with pancreatic exocrine function such as digestive difficulties and altered bowel habits persisted even after 1 year had passed.
Of the existing studies, many reported worse general health perception and physical status of patients who underwent TP versus the matched general population [21011]. A systematic review of 21 studies published between 2005 and 2018 revealed that overall QoL after TP is adversely affected, possibly due to the impact of diarrhea- and DM-related morbidity [13]. A recent nationwide multicenter retrospective cohort study in the Netherlands reported that long-term QoL was lower in patients than in the general population, although the difference was small [12]. On the other hand, studies demonstrate the comparability of QoL before and after TP or with matched healthy control groups. Hartwig et al. [1] found, in a large single-center study, no relevant change in global QoL over time between patients who underwent TP and a matched general population. Stoop et al. [24] demonstrated that overall QoL after surgery was reduced to some extent compared with the general population but did not differ with the self-matched preoperative QoL. Accordingly, the QoL after TP stays worse throughout the postoperative period.
In this study, the GHS scores of the patients in the follow-up period did not differ significantly from the preoperative scores. However, the GHS is based on the results of the EORTC QLQ-C30, a QoL questionnaire for cancer patients in general. The limitation of the GHS score in this study is that it does not reflect factors specific to pancreatic disease or patients who underwent pancreatic resection. Studies are exploring ways to overcome this limitation. Rijssen et al. [25] established a core set of patient-reported outcomes (PROs) in pancreatic cancer selected by both patients and healthcare providers internationally through a Delphi process. The identified 8 core PROs highlight the priorities of patients and healthcare providers in the treatment of pancreatic cancer and are expected to help facilitate the design of future research and prospective studies. Likewise, more studies on pancreas-specific parameters are needed to fully evaluate the QoL of patients with pancreatic disease.
Previous studies have observed that fatigue and gastrointestinal (GI) symptoms, including diarrhea and altered bowel habits, are the most frequently reported symptoms after TP [81213]. Our study also showed that digestive difficulties and altered bowel habits persisted even 1 year after surgery, and bowel movement frequency continued to increase over time, eventually causing diarrhea. Because these symptoms associated with exocrine function persisted even over time, careful management of pancreatic enzyme replacement therapy (PERT) is important. Although the patients in this study were routinely prescribed PERT, the GI symptoms may have persisted or worsened due to the inadequate prescribed dosage or lack of patient compliance. To achieve optimal enzyme replacement therapy, clinicians should routinely prescribe pancreatic enzymes and refer patients to a dietician to help ensure the correct dosage. Dose titration ought to be individualized according to the types of food and medications ingested by each patient [26]. Because compliance is also a crucial factor in the maximal effect of PERT, extensive patient education is also needed [17]. Malabsorption of nutrients after TP is caused by various factors, such as pancreatic enzyme insufficiency, altered bowel habits, neural damage to the celiac and superior mesenteric ganglia, and altered homeostatic balance of GI hormones [27]. Because many factors may be involved, management using PERT alone may be insufficient; thus, further investigations are needed on this issue.
GI symptoms such as diarrhea, altered bowel habits, and digestive difficulties worsen after TP due to altered GI anatomy and exocrine insufficiency, ultimately leading to malnutrition and poor QoL [2728]. In this study, the RBW, TSFT, and MNA scores of the patients were all lower at 3 months and 1 year of follow-up than they were preoperatively. However, although the changes in RBW and TSFT reflect the deteriorating nutritional status of patients over time, the MNA scores showed that the nutritional status had improved by 3 months after surgery and then worsened after 1 year. This points to the limitation of the MNA to accurately reflect the actual nutritional status; thus, more assessment tools for nutritional status that include objective parameters are needed. The MNA was originally designed to evaluate the nutritional status of the geriatric population, and nutritional assessment instruments appropriate for pancreatic resection patients are also needed. This study also showed that most of the patients were already at risk of malnutrition prior to surgery and that the postoperative nutritional status assessed by the MNA questionnaire was comparable. Considering that about half of the patients in this study were diagnosed with pancreatic cancer, it is feasible that their nutritional status was already poor preoperatively due to cancer-related cachexia and anorexia [28]. Because morbidity, mortality, and response to treatment improve with improving nutritional status, nutritional support before and after surgery is of vital importance [29].
Historically, the notion that TP could cause brittle DM was the main reason for the surgeon's reluctance to perform it. However, evidence has shown that DM distress in TP patients is not significantly greater than in patients with type 1 DM [30], and more recent studies have described marked improvement of treatment options for DM in patients after TP [18]. Studies have attributed the improvement of glucose control in TP patients to close monitoring and education for the management of appropriate insulin usage and diet [1618]. In our center, the starting insulin dose and titration dose according to the changes in the patients' general condition and diet, were determined with the consultation of an endocrinologist. The patients were continued to be followed-up by an endocrinologist for a month even after discharge or until the insulin dose stabilized, then referred to clinical centers near the patients' place of residence. For effective glycemic management, consultation and close follow-up with specialized endocrinologists and dieticians, especially in the early period after surgery, are highly recommended.
One of the limitations of this study was that there were insufficient data since some of the patients did not complete the questionnaires or some tests were not performed during follow-up. There was a limitation in the statistical analysis due to the missing data and the consequent small sample size; thus, we could only show trends. Because this was a single-center study including only 30 patients, additional prospective studies with larger study populations or multiple centers are needed to thoroughly explore the QoL of TP patients. As mentioned earlier, another limitation of this study includes lack of parameters specific to pancreatic function. More pancreas-specific questionnaires and objective parameters reflecting pancreatic insufficiency are needed to fully evaluate QoL. Although all patients were prescribed PERT, some chose alternative drugs and others tended to skip doses over time. The PERT was not dose titrated according to each individual's food content and the degree of maldigestion. Emphasis on medication adherence and more research is needed on individualized PERT dose titration depending on each patient's response and experience. And finally, we were unable to fully evaluate endocrine function before and after TP because our main focus was on symptoms associated with exocrine insufficiency and changes in QoL.
The overall GHS score after TP was comparable to the preoperative QoL score. Many of the symptoms significantly worsened after 3 months postoperatively but then improved to a comparable level after 1 year. However, poorer physical function and nutrition and symptoms associated with pancreatic exocrine function, such as digestive difficulties and altered bowel habits, persist even after 1 year. Because nutrition status, physical function, and symptoms produced by exocrine insufficiency continue to deteriorate over time, attention and supportive postoperative management are needed for patients receiving TP, including PERT with dose titration, nutritional support, and education on medication adherence and diet.
Go to :
 XML Download
XML Download