

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is a major cause of morbidity and mortality in Western countries [1] and is the third most common cancer in the Republic of Korea [2]. Although screening can decrease incidence and mortality, CRC screening is only offered to a small portion of the target population worldwide [3]. In 2004, a national cancer screening program for CRC was implemented in Korea. Through this program, all individuals over the age of 50 years can receive an annual fecal occult blood test (FOBT). Any individual who has a positive FOBT result is then offered a colonoscopy examination.
Colonoscopy is a highly effective screening procedure for CRC [4] and can help prevent CRC by detection and removal of precancerous lesions, such as adenomas. Colonoscopy reduces the incidence of CRC, and also reduces mortality by approximately 31%–92%, depending on the population [56789]. The FOBT is inexpensive, widely used for mass screening, and has a high sensitivity in patients with advanced-stage CRC; however, it has a reported sensitivity of only 38.5% in individuals with those stage-T1 CRCs [10]. Although primary screening by colonoscopy is considered a better approach, several issues must be addressed. In particular, when properly performed, colonoscopy is generally safe and accurate, but patients can experience complications or develop interval cancers (cancer during the interval between screening procedures).
The rate of interval CRCs was reported as between 1 per 130 and 1 per 1,000 colonoscopies, thus accounting for 2%–8% of all CRCs [111213141516]. Previous studies reported the rate of interval CRCs in Korea was 7.8%, with an increase over time [17]. The factors responsible for the increasing rate of interval CRC are incomplete resection, failed detection, and aggressive biology of the polyp [141518]. Meticulous inspection of adequately cleaned mucosa and complete removal of preneoplastic lesions are necessary to lower the risk of interval CRC.
In addition, from 2001 to 2005, postcolonoscopy bleeding declined from 6.4 to 2.0 per 1,000 colonoscopies, although the perforation and mortality rates remained stable. A recent meta-analysis reported low overall postcolonoscopy prevalence for perforation (0.5/1,000; 95% confidence interval [CI], 0.4–0.7), bleeding (2.6/1,000; 95% CI, 1.7–3.7), and mortality (2.9/100,000; 95% CI, 1.1–5.5) [19]. Nonetheless, these complications can be serious consequences of the colonoscopy use of a bowel cleansing agent, or use of sedatives.
The participants of the 2018 National Cancer Screening Survey carefully evaluated our screening resources and population screening using colonoscopy to assess the impact on national colonoscopy resources and on complications in patients who are otherwise healthy. According to this survey, which was conducted by the National Cancer Center, about 77% of individuals preferred screening colonoscopies. This suggests that colonoscopy meets one of the requirements of a screening tool, namely that people are willing to use it. However, the most crucial characteristic of a screening colonoscopy program is maintenance of quality in endoscopy units. It is important to use a systematic approach to implement and monitor standards. Colonoscopy programs and units are responsible for quality assurance (QA) [20], and QA strategies are needed to investigate the possible or potential underperformance. Thus, the Executive Board of the Korean Society of Coloproctology (KSCP) commissioned the present Position Statement regarding the certification of accredited endoscopy units for the performance of screening colonoscopies.
METHODS
Colonoscopy specialists representing the KSCP reviewed the published evidence of different quality indicators and adopted a guideline for each that relies on expert consensus about QA strategies for investigating and monitoring potential underperformance. The panel established evidence-based consensus recommendations based on each QA indicator. Indicators lacking evidence were also determined by expert opinions. The authors discussed the contents at a face-to-face conference and amended the manuscript via e-mail. The recommendation is that the Executive Board of the KSCP monitor quality indicators and use them to license individual colonoscopy and endoscopy units. This Position Statement also proposes references for acceptable colonoscopic practice. The text and tables below describe the details of mandatory items in 6 categories to be evaluated for certification of a qualified endoscopy unit: (1) training and competency of the colonoscopist, (2) facilities and equipment, (3) procedure QA parameters, (4) performance quality and auditable outcomes, (5) infection prevention and adequate reprocessing or disinfection of equipment, and (6) sedation and recovery of the patient. Although not a mandatory item, the recommended item and Korean version of the assessment item for the accredited endoscopic unit have been added to Supplementary Tables 1, 2, 3, 4, 5, 6 and Supplementary Data.
THE KSCP GUIDELINE FOR ACCREDITATION OF ENDOSCOPY UNITS
Training and competence of the colonoscopist
A surgeon who is an endoscopy specialist can be considered one of the most advanced gastroenterology and/or gastrointestinal oncologists. These surgeons can provide optimized treatment, from endoscopy to surgery, to patients with precancerous lesions and to those who need palliative care. To become a surgical endoscopist, the KSCP highly recommends that supervised endoscopy training is administered during the residency or fellowship period so that the physician has integrated knowledge on gastroenterology and/or gastrointestinal oncology (Table 1, Supplementary Table 1).
The colonoscopist should be a specialist certified by the KSCP
A colonoscopist who participates in a CRC screening program should be fully trained in colonoscopy, including cecal intubation, biopsy, and polypectomy [2122]. To be considered for credentialing, a colonoscopist must complete a formal 1-year subspecialty training program at a hospital in which 1 certified supervisor is assigned to each trainee. One requirement for achieving competency in endoscopy is the completion of a certain minimum number of colonoscopies. For example, the American Society for Gastrointestinal Endoscopy (ASGE) set the minimum number for assessment of technical competency as 270 supervised colonoscopies [23], and the Korean Society of Gastrointestinal Endoscopy (KSGE) requires 150 procedures at least [24]. Lee et al. [25] found that first-year gastrointestinal fellows reached a cecal intubation rate of 91% after completing 150 colonoscopies and 98% after completing 250 colonoscopies. Another study found that it takes an average of 250 procedures to achieve competence in colonoscopy, based on a cecal intubation rate of 90% and an intubation time of fewer than 15 minutes [26]. On the other hand, the Colonoscopy Academy of the National Cancer Center Korea reported that trainees achieved a 90% cecal intubation rate after performing over 400 colonoscopies [27]. The United Kingdom (UK) Joint Advisory Group on GI Endoscopy replaced its number-based assessment with a combined number and competency assessment. Thus, it requires trainees to perform at least 200 colonoscopies and 200 sigmoidoscopies during their lifetimes, and to achieve a minimum number of procedures that are formally assessed by direct observations of procedural skills [2829]. The Dutch national colorectal cancer screening program (CRCSP) requires a lifetime experience of at least 500 colonoscopies, with at least 200 colonoscopies and 50 polypectomies, as qualification before starting an accreditation program [30]. The KSCP recommends a minimum of 150 successful cecal intubations during 1 year for certification as a colonoscopist. Although it is not a requirement, 100 or more polypectomies over 2 years is recommended for accreditation through the KSCP.
An endoscopy unit for screening colonoscopy should have one or more colonoscopists who performed more than 300 colonoscopies during the last 2 years
According to the ASGE, mastery in endoscopic procedures depends on the continued practice and performance of adequate numbers of procedures. Performance of fewer than 100 colonoscopies in 1 year is associated with a cecal intubation rate less than 90%. The occurrence of adverse events also depends on a colonoscopist's experience. Three population-based studies demonstrated that the occurrence of colonoscopy-related perforation and bleeding increased significantly in endoscopists who performed fewer than 200–300 colonoscopies per year [3132].
The threshold for maintenance of competence varies from 150 to 300 colonoscopies per year, depending on the guideline. Thus, the National Health Service's Bowel Cancer Screening Program in the UK recommends more than 150 screening colonoscopies in addition to non-screening colonoscopies per year. The Dutch CRCSP recommends that colonoscopists perform CRC screening during at least 200 audited colonoscopies per year [30]. The European guideline for QA in CRC screening recommends that each colonoscopist participating in a CRC screening program perform at least 300 procedures per year to ensure a sufficient sample size for assessment of competence [33]. The KSCP recommends the presence of 1 or more colonoscopists who performed more than 300 colonoscopies during the last 2 years in each endoscopy unit.
Colonoscopists should complete a minimum of 12 hours of endoscopy-related education, conferences, and lectures every 3 years
The colonoscopists working within a CRC screening program should have good knowledge of the endoscopic characteristics of a healthy large bowel, its anatomy and physiology, and of disease processes. In addition, they must understand the endoscopy instrument, performance of polypectomy or endoscopic mucosal resection, and management of complications after a procedure. Continuing education is also essential so they understand new developments and can improve their performance. The KSCP recommends that colonoscopists complete a minimum of 12 hours of endoscopy-related education, conferences, and lectures every 3 years.
Endoscopy unit staff should receive maintenance training
Staff participating in a screening colonoscopy program should also learn necessary new procedures. Thus, all endoscopy units should participate in ongoing quality improvement program that includes action plans covering insufficient performance and acquiring knowledge of new developments in endoscopy.
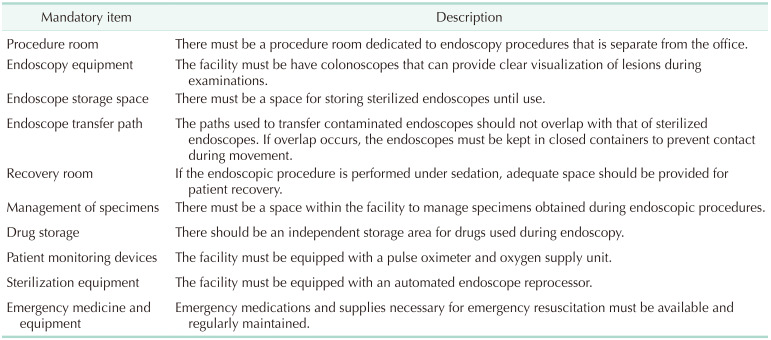
Facilities and equipment
The KSCP considers high-quality and safe endoscopy to depend on adequate maintenance of facilities and equipment and an adequate supply of accessories for a range of specific procedures. However, most existing guidelines do not provide sufficient assessment and accreditation of facilities and equipment. A 1991 guideline for establishing a gastrointestinal endoscopy area briefly referred to the facilities required for endoscopy units [34]. This guideline required a toilet, intravenous equipment, capability for oropharyngeal suction, resuscitation equipment, instrument cabinets, storage area, disinfection of equipment, endoscope and light sources, and electrocautery devices. In 2019, the KSGE published “Accreditation of Qualified Endoscopy Unit,” an update on the guidelines for endoscopy units [35]. This guideline listed 16 mandatory items and 7 recommended items, with each quality indicator classified into 3 categories. The current KSCP guideline lists 10 mandatory items and 13 recommended items for each endoscopy unit. The quality indicators for assessment of an endoscopy unit are classified as endoscopy equipment/accessories, facility/space, and patient monitoring systems (Table 2, Supplementary Table 2).
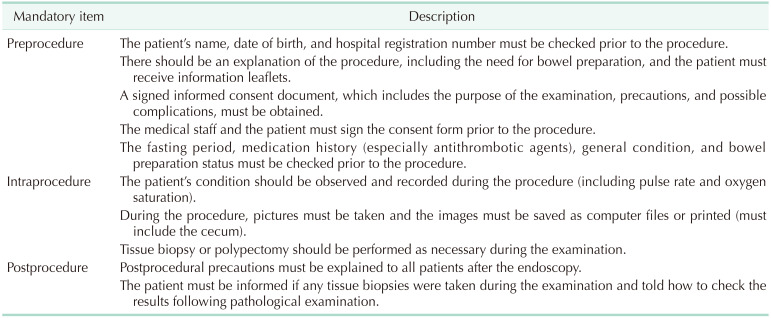
Procedure quality assurance
The large number of endoscopic procedures performed annually indicates the need to perform a QA program of sedation procedures. The monitoring should focus on mitigating patient risk before, during, and immediately after sedation, and should also consider improving procedure outcomes and patient satisfaction (Table 3, Supplementary Table 3).
Effective bowel preparation and other precolonoscopy procedures should be used
The KSCP recommends a precolonoscopy assessment of the patient that includes receipt of appropriate informed consent, a review of the medical history, a physical examination, and assessment of the risks of sedation and based on preexisting medical conditions. Each patient should be stratified by risk for potential complications to improve management of potential problems related to preexisting medical conditions. An objective method, such as the American Society of Anesthesiologists (ASA) physical status classification, should be used to evaluate the general condition of patients [36]. In addition, the ASGE [37] recommends measuring pre-procedural safety based on how frequently certain issues are addressed, including informed consent, completion and documentation of medical history and physical examination, risk assessment, development of a sedation plan, and performance of a procedural pause or “time-out” [38]. The KSGE recommends patient identification, informed consent, and documentation of preprocedural risk assessment [35]. Use of medications, including antiplatelet agents or anticoagulants, during the fasting period should be monitored. Specifically, the ASA guidelines state that patients should fast a minimum of 2 hours after ingestion of clear liquids and 6 hours after ingestion of light meals before sedation. The discontinuation of an antiplatelet or anticoagulation agent is decided by the colonoscopist based on the risk of bleeding during the procedure [3739].
The intraprocedure steps should avoid complications while identifying lesions
The intraprocedure time begins with sedation or insertion of the endoscope and ends when the endoscope is removed and the sedation has ended. Following thorough preparation, it is important to monitor the status of a patient during the procedure. The complications from sedatives include phlebitis from intravenous administration, hypoxemia, cardiac arrhythmias, and aspiration. The most common serious problems are cardiopulmonary complications [404142]. The ASGE and ASA guidelines recommend monitoring of pulse rate, blood pressure, and oximetry for early detection of cardiopulmonary complications, such as hypoxemia and respiratory depression [38]. The ASA also recommends use of continuous electrocardiography for patients with significant cardiovascular disease or dysrhythmias. In addition, there should be visual assessment of the patient's ventilatory activity, level of consciousness, and discomfort [43]. The administration and documentation of medications, frequency of using a reversal agent, and rate of early termination because of adverse issues related to sedation are integral quality indicators [44]. Capnography can be used to detect depressed respiratory activity before transient hypoxemia [20]. However, the ASGE concluded there is inadequate data to support the routine use of capnography for patients in moderate sedation [45].
The primary purpose of colonoscopy is the detection and diagnosis of lesions, so complete observation of the colon and abnormalities must be documented. Therefore, images of the cecum and any lesions observed during examination must be saved as a computer file or in a printed version. A tissue biopsy must be performed when there is an abnormal lesion. Storage of 8 photographs of the standard photograph site, including a cecum and tissue biopsy for any lesions, is also recommended as a mandatory part of the procedure by the KSGE [35].
The postprocedure steps should include explanation of results and follow-up of patients
The postprocedural assessment should include following of established discharge criteria, administering proper instructions to the patient, and tracking adverse events. After the sedation has ended and when the discharge criteria are met, the patient should return home. However, before discharge, each patient should be given a description of complications that may occur, from minor symptoms, such as diarrhea and cramping pain, to major symptoms, such as bleeding and perforation [1946]. In addition, the staff should explain the need to contact the hospital if the patient experiences signs or symptoms of delayed adverse events that require immediate medical attention. Patients should also be provided with written discharge instructions that include diet and activity restrictions, an explanation of biopsy results, information about follow-up appointments, and any medication changes.
Performance quality and auditable outcomes
Several indicators of performance quality should be measured
A quality indicator is an outcome measure supported by sufficient evidence to be strongly recommended as a quality standard. These include cecal intubation rate, withdrawal time, adenoma detection rate, polyp detection rate, quality of bowel preparation, polyp retrieval rate, overall colonoscopy perforation rate, and postpolypectomy bleeding rate. An auditable outcome is a result that should be measured, but is not a quality standard because existing evidence is insufficient. These include sedation level, comfort level, postcolonoscopy CRC, unplanned admission rate, and use of reversal drugs [47]. To be certified, the endoscopy report must describe the information used for auditing the quality indicators. Thus, an endoscopy report must include the date of examination, general characteristics of the patient (name, sex, age, registration number), name of the colonoscopist, drug use, purpose of the examination, bowel preparation state, documentation of cecal intubation and biopsy, predicted diagnosis, and examination time (including insertion time and observation time). When describing a lesion, its location, shape, and size should be reported, and the type of endoscopic procedure and retrieval success should be recorded [48]. Monthly records should be examined to identify the rate of complications, including perforation or bleeding. Use of these reports and documents allows assessment of the major quality indicators (Table 4).
The cecal intubation rate should be at least 95%
A successful cecal intubation is defined as insertion of the endoscope tip to a point proximal to the ileocecal valve so that the entire cecal pole (including the medial wall) can be visualized and examined. The KSCP recommends that an endoscopist should have a cecal intubation rate of at least 95% during screening colonoscopy of healthy adults. Incomplete procedures, due to poor bowel preparation, obstruction, or severe colitis, and therapeutic colonoscopies should be excluded when determining the cecal intubation rate.
At least 95% of patients should have adequate bowel preparation
Adequate bowel preparation is necessary for a high-quality colonoscopy, and poor bowel cleansing significantly reduces the detection rate of neoplasia and advanced neoplasia [49]. Moreover, adequate bowel preparation is associated with a greater cecal intubation rate [50]. Adequate bowel preparation may be defined as a score of 6 or more on the Boston bowel preparation scale, 7 or less on the Ottawa bowel preparation scale, or “fair or better” on the Aronchick scale. The ASGE recommends that 90% of patients have adequate bowel preparation and the European Society of Gastrointestinal Endoscopy (ESGE) guideline recommends a minimum of 90% and target of 95% [5152]. In the KSGE guideline, a minimum of 80% adequate bowel preparation is recommended [35]. Given the importance of adequate bowel preparation for screening colonoscopy, the KSCP recommends that adequate bowel preparation rate should be achieved by more than 95% of patients (Supplementary Table 4).
The withdrawal time should be 6 minutes or more
Withdrawal time may be considered a less important quality indicator than adenoma detection rate or cecal intubation rate, but was adopted as a performance indicator because it is associated with the adenoma detection rate [5354]. To achieve an adequate adenoma detection rate, guidelines recommend a mean withdrawal time of 6 minutes or more [55]. Some studies suggest a withdrawal time of 11 minutes or longer to increase the detection rate of proximal serrated polyps [56], but others claim that the net inspection time, excluding cleansing and suction time, should be at least 6 minutes [54]. However, because it is difficult to precisely measure inspection time, it is usually estimated based on a mean withdrawal time of 6 minutes or more when used as a supportive measure for adequate identification of pathology in a patient with negative results. The mean withdrawal time is calculated as the sum of the total withdrawal time divided by the number of colonoscopies performed that do not require a procedure (Supplementary Table 4).
The polyp detection rate should be at least 40%
The polyp detection rate, defined as the rate at which 1 or more polyps is detected and removed during colonoscopy, correlates with the adenoma detection rate [5758]. An advantage of recording the polyp detection rate rather than the adenoma detection rate is that it does not require manual entry of pathology data. Thus, many previous studies examined the potential use of the polyp detection rate as a quality indicator because it is measured during the colonoscopy, in contrast to the adenoma detection rate, which requires subsequent analysis. The ASGE recommended adenoma detection rate benchmarks of 25% for males and 15% for females, but did not recommend polyp detection rate as a quality indicator [52]. The ESGE recommended a polyp detection rate of 40% or more as a minor performance measure [59]. Patients who received a colonoscopy from a doctor whose polyp detection rate was more than 30% had a lower incidence of proximal interval cancer than those examined by a doctor whose polyp detection rate was 10% (odds ratio, 0.61; 95% CI, 0.42–0.89) [60]. Another study reported the adenoma detection rate/polyp detection rate ratio was 71.3% and this was unchanged for colonoscopists in different polyp detection rate quartiles [61]. Therefore, the KSCP decided to set a polyp detection rate of 40% or more as a performance quality indicator, and did not use the adenoma detection rate because of the requirement for pathological examination (Supplementary Table 4).
The perforation rate should be below 0.1% and the bleeding rate after polypectomy should be below 0.5%
Most of the quality indicators described above assess the accuracy of the examination and monitor the complication rate (bleeding after polypectomy and perforation) because these are essential for assessment of patient safety and acquisition of reliable results. Bleeding is the most common complication of polypectomy, and about 5% of colonoscopic perforations are fatal. Therefore, documentation of adverse events, such as perforation with or without a procedure, bleeding after polypectomy, readmission, and mortality is important. The ESGE guideline suggested a complication rate less than 0.5%, but did not suggest minima for bleeding rate or perforation rate [48]. On the other hand, the ASGE guideline recommended that the bleeding rate after polypectomy should be below 1%, and that the perforation rate should be below 0.2% for all colonoscopies and below 0.1% for screening colonoscopies. The UK guideline recommended that the bleeding rate should be less than 0.5% and the perforation rate after polypectomy should be less than 0.2% [62]. The KSGE guideline did not establish an appropriate endpoint for the complication rate, and it was recommended to describe monthly statistics of patients who received a blood transfusion, hospitalization, or surgery due to a complication [35]. The KSCP recommends a perforation rate below 0.1% and a moderate or severe bleeding rate after polypectomy less than 0.5%. Moderate or severe bleeding is defined as bleeding that necessitates an intervention or operation (Supplementary Table 4).
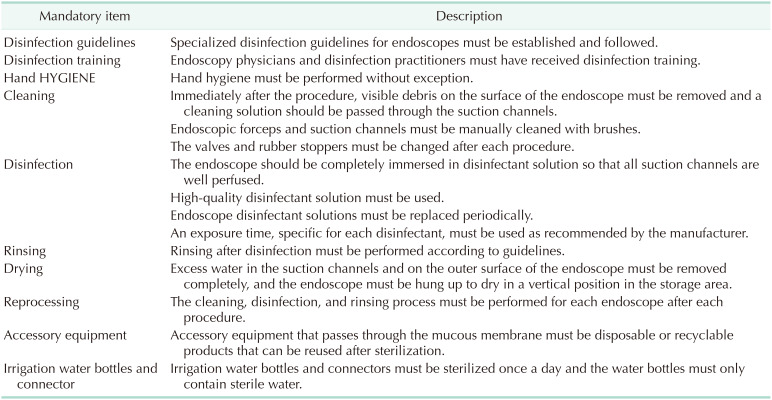
Infection prevention and disinfection of equipment
Procedures used for cleaning and disinfecting equipment should be recorded in a ledger
Several studies reported infections due to inadequate reprocessing of endoscopes and other instruments [6364], although there are no reliable data on the incidence of endoscope-associated infections. It is essential to use high-quality procedures to ensure prevention of infection so that screening colonoscopy procedures are safe. Hence, several consensus guidelines recommend use of a disinfection and reprocessing protocol to prevent infections and use of infection control professionals [3565666768]. The endoscopy room should have written policies and procedures for infection prevention that reflect the current standard guidelines (Table 5).
In the Republic of Korea, 4 organizations certified an “Endoscope cleaning and disinfection guideline,” and the KSCP prepared “Disinfecting guidelines for endoscopy cleaning and disinfection” [69]. According to these written policies, endoscope handling should be performed by qualified practitioners with specific training and experience, and reprocessing should be performed immediately after examination. Immediately after an endoscopy procedure, foreign substances on the outer surface of the endoscope should be wiped off and a detergent solution with suction should be used to clean the inside of the aspiration channel. The insufflation/infusion button, aspiration button, and forceps plug should be detached from the endoscope before cleaning. Then, the interior of the aspiration and forceps channels should be cleaned with a brush.
After manual precleaning of the endoscope, it should be cleaned and disinfected using an automated endoscope reprocessor [30]. The solution used in this process should be a high-quality disinfectant/sterilizing agent capable of destroying all vegetative microorganisms, mycobacteria, small or nonlipid viruses, medium or lipid viruses, fungal spores and some, but not all, bacterial spores. The disinfectant should be routinely tested to ensure the minimum effective concentration of the active ingredient. Strict adherence to the manufacturer's requirements for the reprocessor is critical for the maintenance of appropriate disinfection. Irrigation and drying after disinfection should also be performed in accordance with the instructions.
All of these procedures should be recorded in a “Process Cleaning and Disinfection Management Ledger.” Each unit should have a designated sequence for the safe physical movement of dirty endoscopes and other equipment. The instrument used in the mucosa (e.g., biopsy forceps, polypectomy snares, knives for gastrointestinal treatment, and puncture needles) are in the category of high infection risk. Thus, these instruments must be disposable or sterilized before reuse. For reusable products, sufficient cleaning and sterilization according to the manufacturer's instructions are required. The safety of the colonoscopist and others involved in the procedure must also be protected. Gloves and an impervious gown should be worn by each staff member who is directly engaged in patient care during the procedure.
Sedation and recovery of the patient
All patients should provide informed consent
Sedation during colonoscopy relieves the patient's anxiety, and diminishes the pain, discomfort, and memory of the examination, thereby improving patient tolerance. Despite the benefits of sedation, adverse events such as cardiopulmonary dysfunction can occur depending on patient characteristics and procedural variables. Therefore, the patient should provide informed consent for administration of sedation following a discussion of the benefits and risks (Table 6).
Patients with sedation should be monitored before, during, and after colonoscopy
Conscious sedation, in which a patient can respond to verbal or light tactile stimulation while maintaining spontaneous breathing and cardiovascular function, is the goal for endoscopic procedures. Achieving conscious sedation may vary depending on the characteristics of the patient and the doses and types of sedatives. Thus, it is essential to assess a patient's level of consciousness and vital signs before the procedure begins, after administration of sedative-analgesic agents, during initial recovery, and just before discharge. At a minimum, there should be monitoring of heart rate, pulse oximetry, and visual assessment of ventilatory activity. Assessment of blood pressure should be performed before injection of the sedative agent(s) and during the initial recovery. During colonoscopy, electrical assessment of blood pressure is not recommended because it can interfere with the sedation and may reduce patient comfort. The KSGE guideline recommended a pulse oximetry as an essential device for monitoring, and mentioned that vital signs including oxygen saturation should be recorded during a procedure [35]. The ASGE guideline recommends use of minimal patient monitoring so changes in pulse, blood pressure, ventilatory status, cardiac electrical activity, and level of sedation can be detected before any clinically significant events [43]. There is no evidence that capnography during endoscopic procedures with improved the safety of patients during moderate sedation (Table 6) [70].
Rigorous discharge criteria should be followed
Even after the colonoscopy is over, there is a remaining risk of complications due to use of the sedative drugs. The effect of sedative agents may persist due to metabolic delay, so the level of consciousness, blood pressure, pulse rate, and oxygen saturation should be monitored during recovery. Discharge criteria should be used to assess the recovery from sedation, and the patient must be conscious and oriented with normal vital signs before leaving the endoscopy unit. Other guidelines use several discharge criteria to evaluate recovery from sedation, such as the modified Aldrete score and the Post-Anesthetic Discharge Scoring System (PADSS) [7172]. A score of 8 or higher on the modified Aldrete score and of 9 or higher on the PADSS indicate the patient can be discharged [727374].
An antidote for midazolam should be available
Moderate sedation regimens typically use a benzodiazepine. Most endoscopists favor midazolam because patients experience a rapid onset of action and rapid recovery after withdrawal, and because of its high amnestic properties and the availability of antagonists [75]. Flumazenil is a specific benzodiazepine antagonist that should be readily available in every endoscopy unit (Supplementary Table 6).
The endoscopy unit should have expertise in the use of propofol
Sedation using propofol can provide a faster recovery and discharge, a more rapid sedation and ambulation, and improved patient satisfaction [76]. However, propofol has a narrow therapeutic window, and there is risk for complications if it is not administered appropriately. The main adverse effects are disturbances in cardiopulmonary physiology, such as bradycardia, hypotension, and hypoxemia [77]. Hence, additional training and monitoring may be needed to allow the safe administration of propofol. The KSCP recommends that at least one person in an endoscopy unit has expertise in the use of propofol for sedation (Supplementary Table 6).
CONCLUSION
The guidelines presented here aim to establish an optimal standard level of performance for endoscopy units and individual colonoscopists who perform screening colonoscopies. Furthermore, this Position Statement provides guidance on measuring clinical outcomes and the area(s) of performance that influence those outcomes. Ultimately, this statement can be refined toward evidence-based best practice. The next step is to implement these key performance measures in endoscopy units throughout the Republic of Korea. We recommend individual colonoscopists, as well as the heads of endoscopy units, start implementation of these performance measures without delay.
As these guidelines for screening colonoscopy are implemented, new data on efficacy and safety will allow updating of these guidelines. In particular, we expect that certain guideline performance domains, such as those regarding the facilities and equipment of endoscopy units, will continue to be upgraded as data becomes available.



 XML Download
XML Download