

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Locoregional recurrence is a major concern after rectal cancer surgery, with associated risk factors including positive circumferential resection margins following total mesorectal excision (TME) [1]. In addition, the lateral compartment, which is identified as the potential site of locoregional recurrence, is not removed during TME [2].
The optimal approach for lymph node metastasis in the lateral compartment is controversial, with neoadjuvant therapy followed by TME being preferred in Western countries [3] and lateral lymph node dissection (LLND) being preferred in Japan [4]. Kusters et al. [5] suggested that both radiotherapy followed by TME and extended surgery with LLND result in a more effective local control compared to TME alone. Recently, a multicenter randomized trial of Japan Clinical Oncology Group (JCOG0212) reported lower rates of local recurrence after mesorectal excision with LLND compared to rates noted after mesorectal excision alone.
Despite these promising results regarding the oncological efficacy of LLND, genitourinary function impairment is a negative factor for the routine adoption of LLND owing to its potential to produce a poor postoperative quality of life (QoL) [6]. Most functional studies are from Japan where neoadjuvant chemoradiotherapy is usually not considered for the treatment of rectal cancer patients. In addition, studies assessing the health-related QoL following LLND are rarely reported. Therefore, this study aimed to evaluate the QoL and genitourinary function following TME with LLND compared to those after TME alone following neoadjuvant chemoradiotherapy in rectal cancer patients.
METHODS
Population
This retrospective comparative study included patients who underwent rectal cancer surgery after neoadjuvant chemoradiotherapy between September 2011 and October 2018 in the National Cancer Center, Korea. The eligibility criteria included histologically proven rectal cancer with the lower margin below the peritoneal reflection. The outcomes were assessed with validated questionnaires at the following 3 time-points; before initiation of neoadjuvant chemoradiotherapy and at 3 months and 1 year postoperatively. The questionnaires were administered by a single study coordinator who also recorded the answers. Informed consent was obtained from all participants. The medical records of the patients were reviewed retrospectively. This study was approved by the Institutional Review Board of National Cancer Center, Korea (No. NCC2020-0042).
Treatment
We have previously described our protocol for preoperative staging and administration of neoadjuvant therapy [7]. The lateral pelvic area was usually included in the radiation target volume. TME with high ligation of the inferior mesenteric vessels was performed at 4 to 8 weeks after completion of neoadjuvant chemoradiotherapy. In case of enlarged lateral lymph nodes (LLNs) with a short-axis diameter of ≥5 mm on initial MRI, LLND was performed with preservation of the autonomic nerves, as described in a previous report [8]. The lateral, medial, cranial, caudal, and dorsal anatomical borders for the extent of LLND are the external iliac artery, pelvic plexus, bifurcation of the common iliac artery, levator ani muscle, and sciatic nerve, respectively. We considered creating a diverting ileostomy in case of lower anastomosis or neoadjuvant chemoradiotherapy. Stoma reversal was performed 3 months postoperatively or 1 month after adjuvant therapy, if indicated, after evaluating the anastomosis with loopogram and sigmoidoscopy.
Questionnaires
In all patients, the QoL was assessed using the European Organization for Research and Treatment of Cancer (EORTC) core quality of life questionnaire (QLQ-C30) and colorectal cancer-specific quality of life questionnaire (QLQ-CR38); urinary function was assessed using the International Prostate Symptom Score (IPSS) questionnaire; sexual function was assessed in male patients using the 5-item version of the International Index of Erectile Function (IIEF-5) questionnaire.
The EORTC QLQ-C30, which evaluates the QoL of cancer patients, is composed of 5 functional scales (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (fatigue, nausea and vomiting, and pain), 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and a global health status scale [9].
The EORTC QLQ-CR38, which complements the QLQ-C30 and evaluates the QoL of colorectal cancer patients, includes 4 functional scales (body image, sexual functioning, sexual enjoyment, and future perspective) and 8 symptom scales (micturition problems, gastrointestinal symptoms, chemotherapy side effects, problems with defecation, stoma-related problems, male sexual problems, female sexual problems, and weight loss) [10]. In both the EORTC QLQ-C30 and QLQ-CR38, higher scores on the functional scales and global health status scale represent better health-related QoL, while higher scores on the symptom scales or items represent worse health-related QoL. A difference of ≥10 points is regarded as clinically important [11].
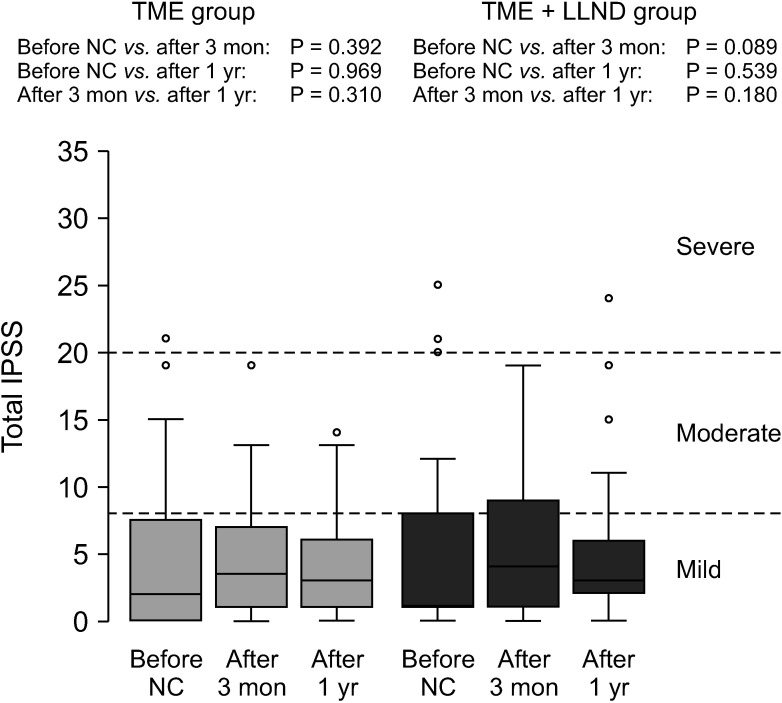
The IPSS evaluates the urinary function and consists of 7 items, including incomplete emptying, frequency, intermittency, urgency, weak stream, straining, and nocturia. The total score was categorized as mild (0–7), moderate (8–19), or severe (20–35) dysfunction. The IPSS was also used for measuring the QoL related to the urinary symptoms, and the scores ranged from 0 (delighted) to 6 (terrible) [12].
The IIEF-5 evaluates male sexual function and consists of 5 items, including erection confidence, maintenance ability, maintenance frequency, erection firmness, and sexual satisfaction. The total score ranged from 5 to 25, and a score of ≤21 indicated abnormal function [13].
Statistical analysis
To compare the characteristics between the 2 groups, the t-test or Wilcoxon rank-sum test was used for the continuous variables and Pearson chi-square test or Fisher exact test was used for the categorical variables, as appropriate. The scores for each questionnaire were presented as the median with range (minimum–maximum) or interquartile range (Q1–Q3) for the continuous variables and as the frequency with proportion for the categorical variables. The differences between the 2 groups were tested using Wilcoxon rank-sum test, Pearson chi-square test, or Fisher exact test, as appropriate. Wilcoxon signed-rank test was used to evaluate the significant changes in the continuous scores within a group over the study period. The IPSS was assessed using univariable and multivariable logistic regression with clinical factors. Multivariable analysis was performed with a backward elimination method. All results were considered statistically significant when the 2-sided P-value was less than 0.05. Statistical analyses were performed using SAS software, ver. 9.4 (SAS Institute Inc., Cary, NC, USA) and R software, ver. 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org).
RESULTS
Among patients who received neoadjuvant chemoradiotherapy for rectal cancer, 425 patients underwent TME alone and 128 underwent TME with LLND in National Cancer Center, Korea between September 2011 and October 2018.
During the study period, 67 male patients answered the IIEF-5 questionnaire, which is applicable to sexually active patients [14], before initiation of neoadjuvant chemoradiotherapy, and at 3 months and 1 year postoperatively. A total of 36 patients (27 in the TME alone group and 9 in the TME with LLND group) reported sexual activity before initiation of neoadjuvant chemoradiotherapy. Among them, 14 patients—11 (40.7%) in the TME alone group and 3 (33.3%) in the TME with LLND group—maintained sexual activity at 1 year postoperatively. Owing to the small number of sexually active patients according to the IIEF-5, this study included patients with the results of the EORTC QLQ-C30, QLQ-CR38, and IPSS at all 3 evaluation time-points.
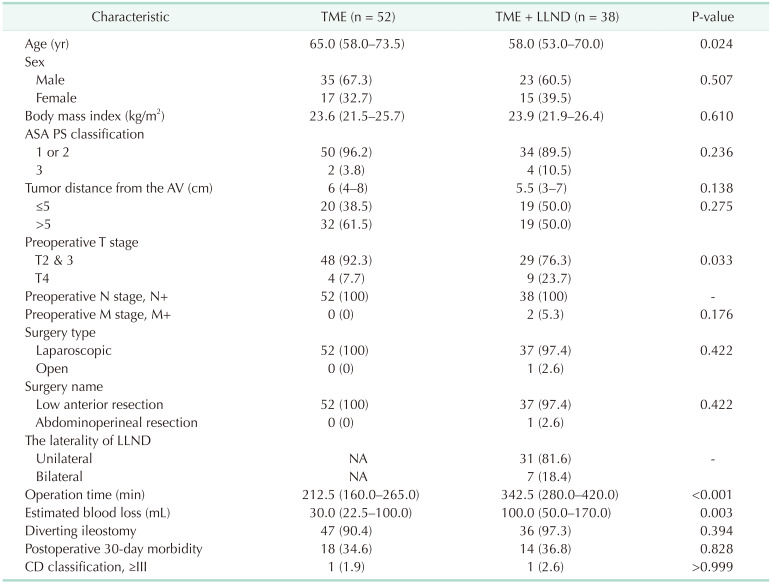
Thus, the study included 52 patients who underwent TME alone and 38 patients who underwent TME with LLND. All these patients completed the EORTC QLQ-C30, QLQ-CR38, and IPSS questionnaire at all 3 evaluation time-points. The patient characteristics are shown in Table 1. The patients in the TME with LLND group were significantly younger (P = 0.024), while the incidence of clinical T4 stage disease (P = 0.033) and estimated blood loss (P = 0.003) were higher and the operation time was longer (P < 0.001) than those noted in the TME alone group. In the TME with LLND group, 31 patients underwent unilateral LLND and 7 patients underwent bilateral LLND. The hypogastric nerve was sacrificed in 1 of the patients who underwent unilateral LLND and none of the patients who underwent bilateral LLND. Postoperative 30-day mortality did not occur in any of the patients included in this study. The overall postoperative 30-day morbidity was similar between the groups. 2 Patients (1 in each group) had complications with a Clavien-Dindo classification of III or IV.
Quality of life based on the EORTC QLQ-C30
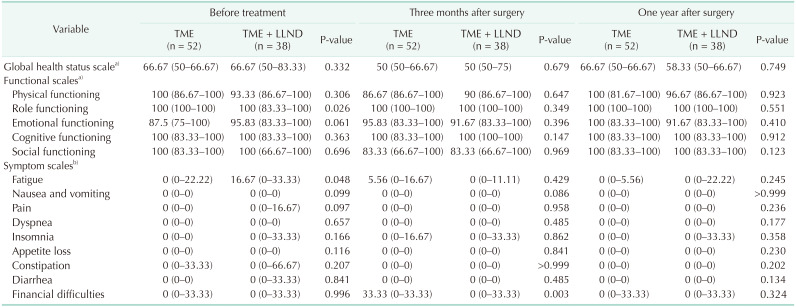
All 90 patients completed the EORTC QLQ-C30 at all 3 evaluation time-points. The role functioning and fatigue scale scores were significantly worse in the TME with LLND group before neoadjuvant chemoradiotherapy (P = 0.026 and P = 0.048, respectively) (Table 2). At 3 months postoperatively, a significantly greater number of patients reported the financial impact of the disease in the TME group (P = 0.003). At 1 year postoperatively, there was no significant difference between the groups with respect to all the scales.
Quality of life based on the EORTC QLQ-CR38
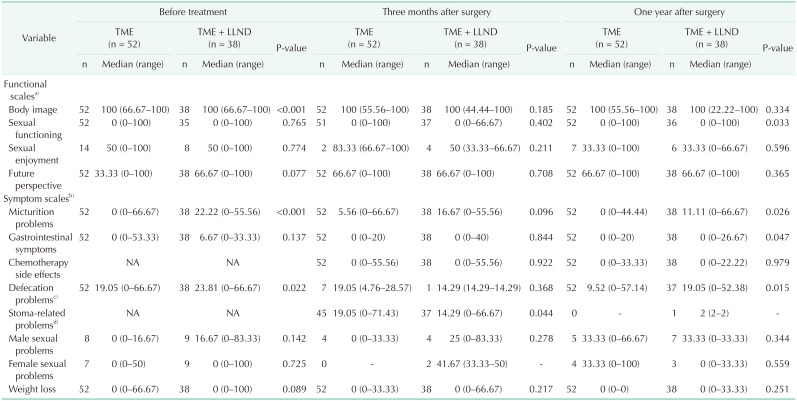
The scales of chemotherapy side effects and stoma-related problems were not evaluated before the administration of neoadjuvant chemoradiotherapy. At 1 year postoperatively, only 1 patient who underwent Hartmann operation maintained a stoma. Owing to the small number of sexually active patients (7 patients in the TME alone group and 12 in the TME with LLND group at 1 year postoperatively), valid statistical analyses for the QoL scales of sexual enjoyment and male/female sexual problems could not be performed (Table 3).
In the TME with LLND group, the score for the scale of perceived body image was significantly worse before the administration of neoadjuvant chemoradiotherapy (P < 0.001). The score for the scale of micturition problems was significantly worse before the administration of neoadjuvant chemoradiotherapy (P < 0.001) and at 1 year postoperatively (P = 0.026). The score for the scale of defecation problems was also significantly worse before the administration of neoadjuvant chemoradiotherapy (P = 0.022) and at 1 year postoperatively (P = 0.015).
Urinary function based on the IPSS
Significant differences were not noted between the groups when comparing the total score, severity score, and QoL score related to urinary symptoms (Table 4). Both groups showed no significant changes in the IPSS at 1 year postoperatively (Fig. 1).
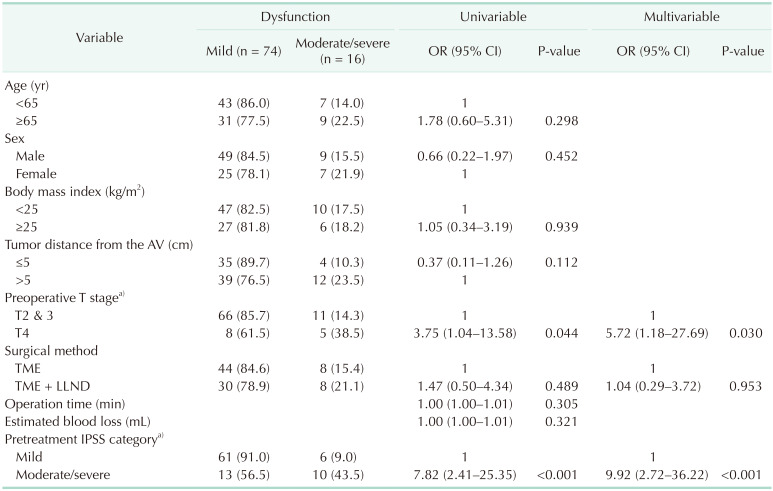
Based on the IPSS at 1 year postoperatively, disease severity was classified as mild vs. moderate/severe dysfunction, and univariable and multivariable logistic regression analyses were performed (Table 5). The results showed that the clinical T stage (odds ratio [OR], 5.72; 95% confidence interval [CI], 1.18–27.69; P = 0.030) and pretreatment IPSS category (OR, 9.92; 95% CI, 2.72–36.22; P < 0.001) were significantly associated with postoperative urinary dysfunction.
DISCUSSION
This study assessed the QoL and genitourinary function after TME with LLND compared to those after TME alone in the setting of neoadjuvant chemoradiotherapy for rectal cancer. To the best of our knowledge, this is the first study that evaluated the QoL and urinary function following LLND with validated questionnaires and reported comparable results between the groups. A greater number of patients with T4 stage disease required TME with LLND, which was associated with greater blood loss and longer operation time. Statistical analyses for the sexually-related QoL scales were not valid due to the small number of sexually active patients. Based on the IPSS, the urinary function was comparable between the groups. After adjusting for clinically and statistically significant factors, multivariable analysis showed that LLND was not significantly associated with postoperative urinary dysfunction.
The score for the QoL scale of micturition problems, including frequency and pain while urinating, was worse in the TME with LLND group before the administration of neoadjuvant chemoradiotherapy. This may be because of differences in the prevalence of preoperative conditions, including symptomatic benign prostatic hyperplasia; however, it is also less likely because the TME with LLND group comprised significantly younger patients. Among 5 patients with severe pretreatment urinary dysfunction according to the IPSS, 4 (1 patient who underwent TME alone and 3 patients who underwent TME with unilateral LLND) patients had clinical T4 stage disease (tumors invading the prostate gland) or tumors located in the anterior wall of the rectum on the initial MRI, and their IPSS categories improved postoperatively. In this study, the clinical T stage and preoperative urinary function were identified as the statistically significant predictors of postoperative urinary dysfunction. Thus, the cancer status, including size, location, and invasion, may be associated with the preoperative urinary function and may affect the postoperative urinary function. Moreover, previous studies have reported not only preoperative urinary function but also blood loss and autonomic nerve damage as significant predictors of postoperative urinary dysfunction [1516]. In this study, a greater number of patients with T4 stage disease required TME with LLND, which resulted in more blood loss and longer operation time. Thus, locally advanced cancer may contribute toward worse preoperative urinary function and wider resection may be required, thus, increasing the possibility of bleeding and damage to the autonomic nerves, which may, in turn, worsen the postoperative urinary function.
With respect to the effect of LLND on the postoperative urinary function, a meta-analysis reported 3.70 times higher risk of urinary dysfunction, 2.08 times higher risk of urinary incontinence, and 2.31 times higher risk of urinary retention with LLND [17]. Therefore, in Japan where LLND is indicated for rectal cancer that invades beyond the muscularis propria [4], autonomic nerve-sparing surgery has been suggested to improve the urinary and sexual function outcomes [1819]. Akasu et al. [20] reported the importance of pelvic plexus preservation in maintaining the urogenital function in men when performing LLND. In addition, the recent JCOG0212 trial suggested no significant sexual or urinary function impairment following autonomic nerve-preserving LLND [1415].
Among the patients in the TME with LLND group, the invaded ipsilateral hypogastric nerve was sacrificed in only 1 of the patients who required unilateral LLND, and the patient's urinary function worsened from mild to moderate dysfunction after LLND. Among the patients who underwent bilateral LLND, there was no case in which the hypogastric nerve was sacrificed. As the autonomic nerves were preserved in the other patients, the score for the QoL scale of micturition problems was worse both before and after treatment in the TME with LLND group. However, the median QoL score for micturition problems in the TME with LLND group was the highest before treatment and decreased gradually postoperatively. Considering the higher incidence of T4 stage disease and the worse median QoL score for micturition problems before treatment in the TME with LLND group, the negative impact of LLND is not clear. In addition, the preoperative and postoperative scores on a more specifically developed IPSS questionnaire were comparable between the groups and did not change significantly at 1 year postoperatively in both groups. Multivariate analysis for the postoperative urinary dysfunction also showed that LLND was not a statistically significant predictor. Thus, nerve-sparing LLND may not result in significant impairment of urinary function.
On considering the laterality of LLND, among 7 patients who underwent bilateral LLND, 2 patients developed worsened urinary function, based on the IPSS, from mild dysfunction before treatment to moderate dysfunction after treatment. In addition, only 1 patient (a female patient with clinical T3 stage disease) reported postoperative severe dysfunction. However, she also was in the severe IPSS category before the administration of neoadjuvant chemoradiotherapy. Even with bilateral LLND, it is not clear whether LLND itself results in urinary function impairment.
In addition, among the TME with LLND group, only 1 patient who underwent unilateral LLND still requires changing of the ipsilateral ureteral stent due to ureteral stricture; she had mild urinary dysfunction according to IPSS before and after surgery, possibly due to ureteral stent insertion. The others do not receive ongoing medical treatment or regular intervention.
Previous studies on defecatory dysfunction following LLND reported no significant impairment, and a shorter anastomosis distance from the anal verge was suggested as an independent risk factor [1721]. Studies on low anterior resection syndrome, which is a major concern after rectal cancer surgery and includes a vast spectrum of bowel and anorectal symptoms, reported a shorter anastomosis distance from the anal verge, TME, and neoadjuvant therapy as the independent risk factors [222324]. In this study, the scores for the QoL scale of defecation problems were worse in the TME with LLND group both before and after treatment. However, the median score in the TME with LLND group was the highest before treatment and decreased postoperatively, which may be because of the higher incidence of advanced-stage disease in the TME with LLND group. Therefore, the effect of LLND is not clear.
There are some limitations to this study. First, the response rates for the questionnaires were low owing to retrospective design; hence, the study population was small. Second, sexual functions were not evaluated due to the small number of sexually active patients. However, despite the lack of sexual functional outcomes, this study evaluated the general QoL and showed comparable results between the groups. To the best of our knowledge, previous studies have reported only specific functional outcomes following LLND. Moreover, with the validated questionnaire, this study evaluated urinary function more specifically.
Recently, Ogura et al. [25] reported that in a multicenter pooled analysis of 1,216 consecutive patients, those who had enlarged LLNs of ≥7 mm on pretreatment MRI required LLND with TME after neoadjuvant therapy in order to prevent lateral local recurrence. However, functional studies for LLND in the setting of neoadjuvant chemoradiotherapy are lacking. The results of this study, showing similar QoL with or without autonomic nerve-preserving LLND after neoadjuvant chemoradiotherapy, may be supportive for additional studies conducted in the future.
In conclusion, LLND did not lead to significant impairment of the QoL or urinary function. It was not significantly associated with postoperative urinary dysfunction. The sexual function could not be evaluated in this study owing to the small number of sexually active patients. Larger prospective studies with long-term follow-up are, therefore, required.

 XML Download
XML Download