

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelioid hemangioendothelioma (EHE) is a rare vascular tumor, consisting of cords of epithelioid cells on a background of myxohyaline stroma. The 2002 World Health Organization (WHO) classification described EHEs as lesions with metastatic potential [12]. EHEs can be observed in any site in the human body, with the most common sites being the liver (21%), liver and lungs (18%), lungs (12%), and bones (14%) [3]. These rare borderline vascular tumors have an aggressiveness graded between hemangioma and hepatic hemangiosarcoma [4]. Because many patients with hepatic EHE are asymptomatic, are detected incidentally [5678]. Due to their rarity and protean behavior, the optimal treatment of hepatic EHEs has not yet been standardized [5]. Partial hepatectomy is used to treat patients with unilobar hepatic EHE, although aggressive tumor recurrence has been reported in the literature [910]. To date, only a few patients from Korea have undergone hepatic resection (HR) for hepatic EHE [1112]. The present study investigated the outcomes of HR in patients with hepatic EHE at our center over a 10-year period.
Go to : 
METHODS
Patient selection
The primary liver cancer database at our institution was extensively searched to identify patients diagnosed with hepatic EHE following HR. Of the 11,976 patients who underwent HR for various indications during the 10-year period from January 2009 to December 2018 [13], 11 (0.1%) underwent HR for hepatic EHE. The medical records of these patients were retrospectively reviewed. The study protocol was approved by the Institutional Review Board at Asan Medical Center (No. 2019-1347), which waived the requirement for informed consent due to the retrospective nature of this study. This study was performed in accordance with the ethical guidelines of the World Medical Association Declaration of Helsinki 2013. The patients were followed up until July 2020 by medical record review and with the assistance of the National Health Insurance Service.
Preoperative evaluation, surgical procedures, and postoperative follow-up
Routine preoperative evaluation for primary liver tumors has been described [14]. In general, patients who underwent HR for borderline malignancy were followed up every 3–4 months during the first year after surgery and every 4–8 months thereafter. Patients with recurrent liver tumors were treated as described [14151617].
Pathological evaluation
Formalin-fixed paraffin-embedded tissue samples were immunohistochemically stained with antibodies to CD34 (1:500, QBEND10, Immunotec Inc., Monrovia, CA, USA), CD31 (1:800, JC70, Cell Marque, Rocklin, CA, USA), and coagulator factor VIII-related antigen (FVIII:Ag) (1:2,000, DAKO, Glostrup, Denmark) using a Benchmark autostainer (Ventana Medical System, Tuscon, AZ, USA). Histological features and immunohistochemical profiles for diagnosis of hepatic EHE were based on the 2010 WHO classification of liver tumors [18].
Statistical analysis
Numerical data are presented as means and standard deviations. Continuous variables were compared by 1-way analysis of variance. Survival was estimated using the Kaplan-Meier method. A P-value < 0.05 was regarded as statistically significant. All statistical analyses were performed using IBM SPSS Statistics ver. 22 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
Patient demographics and preoperative diagnosis
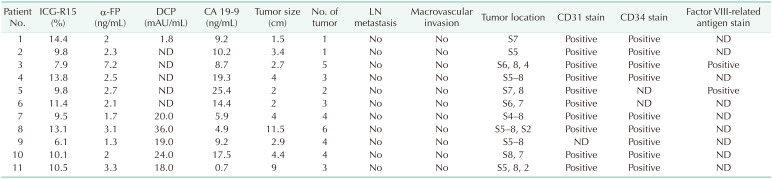
The clinicopathological features of the 11 patients with hepatic EHE are described in Table 1. The 11 patients included 9 females (81.8%) and 2 males (18.2%) with mean age of 43.5 ± 13.6 years. Two patients (18.2%) were positive for hepatitis B virus infection, but none was positive for hepatitis C virus infection or alcoholic liver disease. Only 1 patient reported vague right flank pain, whereas the other 10 patients were asymptomatic at the time of diagnosis. Liver lesions were detected incidentally during routine health screening in 9 patients, during postoperative cancer screening in 1, and during general examination for abdominal pain in 1.
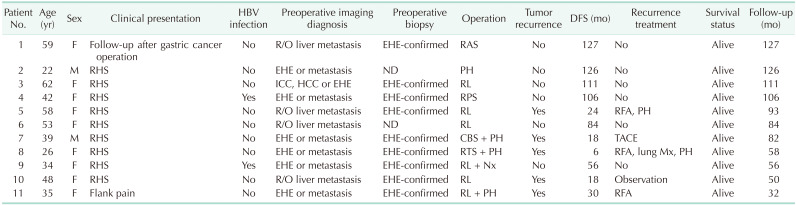
Table 1
Clinical profiles of patients who underwent hepatectomy for hepatic EHE
EHE, epithelioid hemangioendothelioma; DFS, disease-free survival; F, female; M, male; R/O, rule out; RAS, right anterior sectionectomy; RHS, routine health screening; ND, not done; PH, partial hepatectomy; ICC, intrahepatic cholangiocarcinoma; HCC, hepatocellular carcinoma; RL, right hepatectomy; RPS, right posterior sectionectomy; RFA, radiofrequency ablation; CBS, central bisectionectomy; TACE, transarterial chemoembolization; RTS, right trisectionectomy; Nx, nephrectomy; Mx, metastasectomy.
![]()
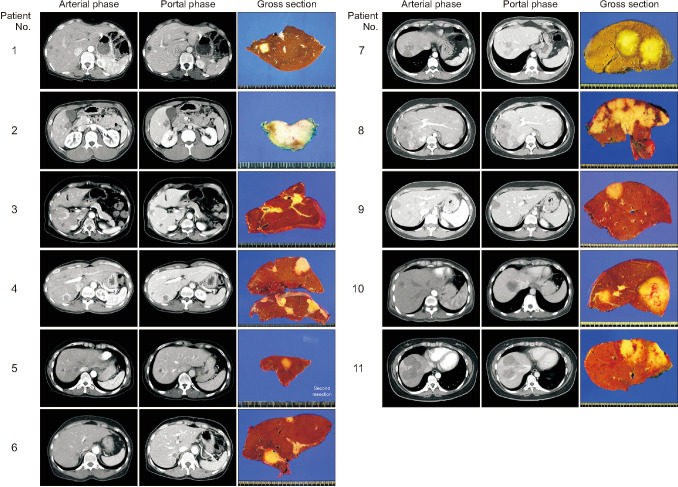
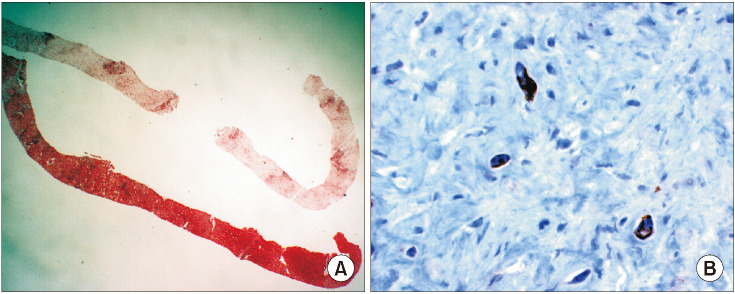
Based on imaging modalities, these patients were preoperatively diagnosed with suspected liver metastasis or EHE (Fig. 1). Nine (81.8%) underwent preoperative liver biopsy, with all 9 diagnosed with hepatic EHE (Fig. 2). One patient was followed up for 5 years after initial liver biopsy and finally underwent HR due to slowly progressive tumor growth.
The mean preoperative serum concentrations of α-FP (2.8 ± 1.6 ng/mL; reference, 7.5 ng/mL), des-γ-carboxy prothrombin (19.8 ± 11.0 mAU/mL; reference, 40 mAU/mL), and for CA 19-9 (11.4 ± 7.1 ng/mL; reference, 37 ng/mL) were within normal ranges. None of these patients presented with abnormal elevation of these tumor markers.
Outcomes after hepatic resection
Preoperative indocyanine green retention tests at 15 minutes yielded a mean of 10.6% ± 2.5% in the 11 patients. One patient underwent preoperative portal vein embolization for right hepatectomy.
The extent of HR was based on the tumor location and size. Six patients underwent right hepatectomy, with 1 each undergoing right anterior sectionectomy, right posterior sectionectomy, central bisectionectomy plus partial hepatectomy, right trisectionectomy plus partial hepatectomy, and partial hepatectomy (Fig. 1). One of the patients who underwent right hepatectomy also underwent concurrent right nephrectomy due to renal cell cancer.
The tumors showed an infiltrating growth pattern into the surrounding liver parenchyma. Low-power magnification showed small numbers of cellular epithelioid or spindle tumor cells within the fibromyxoid stroma. The epithelioid tumor cells contained vacuolated cytoplasm, mimicking signet ring cells. Thin-walled venules contained tufted or micropapillary clusters of epithelioid tumor cells in peritumoral areas. Immunostaining showed that the tumor cells were diffusely positive for CD31, CD34, and FVIII:Ag (Fig. 3, Table 2), resulting in a final diagnosis of hepatic EHE.
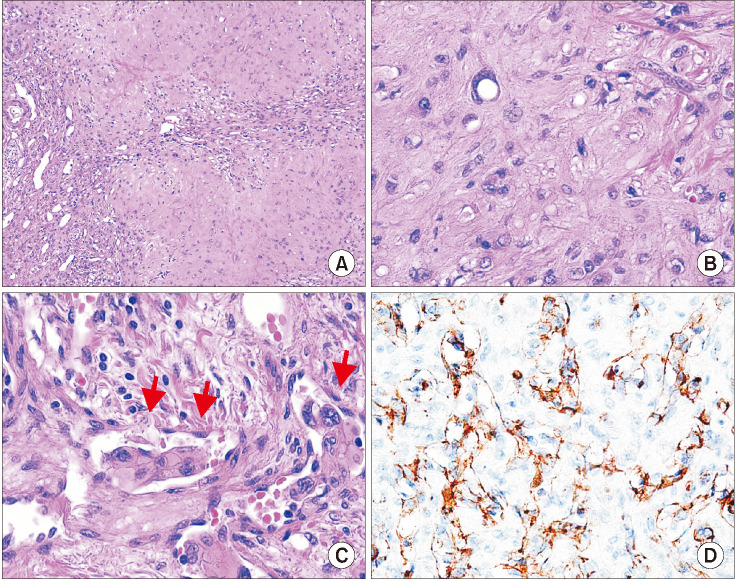 | Fig. 3Microscopic findings of hepatic epithelioid hemangioendothelioma obtained from patient 5, showing (A) few cellular epithelioid or spindle tumor cells on a background of fibromyxoid stroma (H&E staining, ×100), (B) epithelioid tumor cells containing vacuolated cytoplasm (H&E staining, ×400), (C) thin-walled vessels containing clusters of epithelioid tumor cells (arrows; H&E staining, ×400), and (D) tumor cells diffusely positive for CD31 (×400).
|
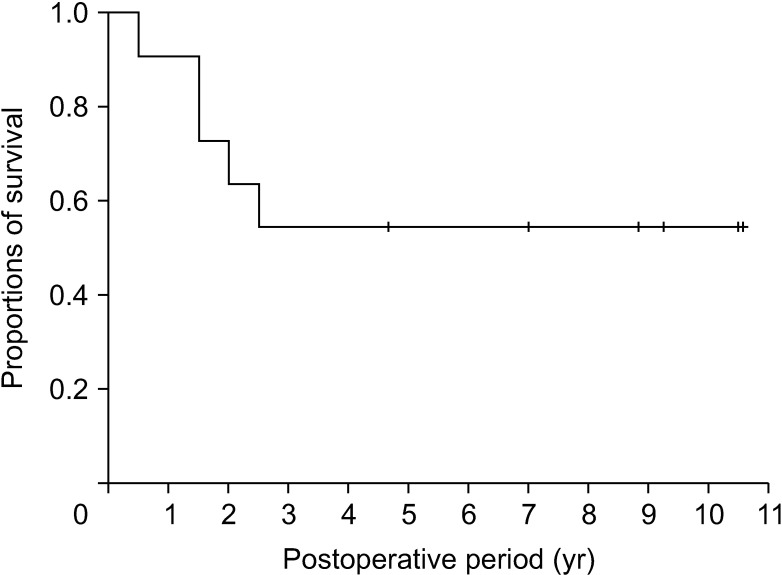
All patients recovered uneventfully from HR without any major complications. During a mean follow-up period of 84.1 ± 32.0 months, 5 patients showed tumor recurrence. The 1-, 3-, 5-, and 10-year disease-free survival rates were 90.9%, 54.5%, 54.5%, and 54.5%, respectively (Fig. 4). The 4 patients with tumor recurrence underwent various treatments, including radiofrequency ablation (RFA), transarterial chemoembolization (TACE), and surgical resection of the liver and lung lesions. One patient with tumor recurrence showed no progression of the tumor and has therefore been closely followed up for 2 years. Currently, all 11 patients are alive and doing well.
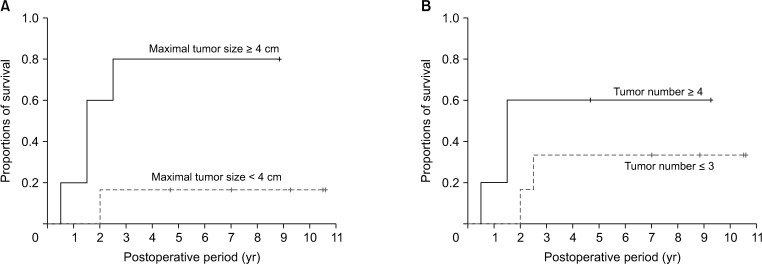
Univariate analysis assessing factors associated with tumor recurrence showed that tumor size ≥ 4 cm was significantly associated with tumor recurrence (P = 0.032), but tumor number ≥ 4 was not related to tumor recurrence (P = 0.24) (Fig. 5).
Go to :
DISCUSSION
Hepatic EHE is a rare borderline vascular tumor, with an aggressiveness graded between that of hemangioma and hepatic hemangiosarcoma [3]. Many hepatic EHEs are detected incidentally because of absence of specific symptoms. Imaging findings of hypovascularity and multiplicity suggest the need for liver biopsy because hepatic EHEs are often confused with liver metastases. Therefore, most of the patients in the present study underwent percutaneous liver biopsy and were diagnosed with hepatic EHE based on histological characteristics and immunohistochemical profiles [18].
Treatments for hepatic EHE can include HR, liver transplantation (LT), chemotherapy, radiotherapy, hormone therapy, RFA, and surveillance alone. Five-year patient survival rates have been reported to be 75% in 22 patients who underwent HR, 20% in 60 patients treated with chemotherapy/ radiotherapy, and 4.5% in 70 patients who underwent surveillance alone [6]. A study of 11 patients who underwent HR and 11 LT recipients reported 5-year patient survival rates of 86% and 73%, respectively [19], whereas a study with 17 patients who underwent HR and 12 patients who underwent TACE reported 3-year patient survival rates of 74.1% and 81.6%, respectively [7]. Two patients with diffuse lesions who received LT and 1 who underwent RFA were alive without recurrence, whereas all 3 patients who underwent HR showed recurrence [20]. In addition, 6 patients opted for observation without treatment.
Although these studies showing similar outcomes following HR, LT, and nonsurgical locoregional treatments, the indications for each treatment modality differed. HR is indicated for resectable intrahepatic lesions, whereas LT and TACE can be considered if the lesions are unresectable. Extrahepatic involvement, such as lymph node metastasis and metastases to other organs, is a contraindication for surgical treatment. Few studies to date have evaluated outcomes of nonsurgical therapies, including systemic/regional chemotherapy, radiotherapy, hormone therapy, and immunotherapy, in patients with hepatic EHE [212223].
Factors prognostic of outcomes after hepatic EHE remain generally undetermined to date. Extrahepatic spread of disease beyond the portal lymph node metastasis was reported to be associated with worse outcomes [23]. Patients with multiple nodules have a worse prognosis than those with single nodules. In contrast, prognosis is not mainly affected by the presence of extrahepatic metastases per se [19]. Worsened overall survival has been observed in patients with hepatic EHEs of >10 cm in diameter and in older patients. The average 1-year and 5-year overall survival rates following various treatment modalities have been reported to range from 88% to 100% and from 23% to 83%, respectively, depending on the biological behavior of the tumor [24]. Because only a few small case series have evaluated the prognostic factors, extrahepatic metastasis remains the only predictor of patient prognosis. The present study found that tumor size ≥ 4 cm was associated with higher tumor recurrence, but tumor number ≥ 4 was not related to tumor recurrence.
This study had several limitations, including its retrospective design and inclusion of a small number of patients treated at a single center. Multicenter studies are needed to evaluate the characteristics of hepatic EHE and to determine the factors predictive of patient prognosis.
In conclusion, hepatic EHE is a rare form of the primary liver tumor and is often misdiagnosed as a metastatic tumor. Because this disease carries malignant potential, HR is indicated if possible. HR plus, when necessary, treatment of recurrence yields favorable overall survival rates in patients with hepatic EHE.
Go to :
 XML Download
XML Download