

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Traumatic injuries are a leading cause of death, with 5 million deaths reported each year globally. Trauma mortality shows trimodal peaks, and the third peak occurs at a later time after injury, which accounts for 20% of all trauma deaths [1]. Infection is a major cause of death in the third peak, and abdominal trauma is a common cause of unrecognized fatal injuries.
Proper use of antibiotics during abdominal surgery is essential in reducing the incidence of surgical site infection (SSI), and the guidelines for the use of prophylactic antibiotics in elective surgery are well established [2]. However, most studies about the use of antibiotics for abdominal trauma focused on penetrating injuries acquired on the battlefield, and the number of large-scale studies about abdominal trauma is limited [34]. In the current recommendation for penetrating abdominal injury, without bowel perforation, there is no need to prescribe other antibiotics in addition to preoperative prophylactic antibiotics, which should only be administered for 24 hours in the presence of a hollow viscus injury [56].
Numerous surgeons have been empirically using antibiotics. However, no studies have investigated the type of antibiotics and duration of therapy in individuals with abdominal trauma in Korea. Thus, the present study aimed to investigate the status of initial antibiotic therapy in patients with abdominal trauma. This is a pilot study before applying the guidelines about the use of antibiotics for abdominal injuries in Korea [7].
Go to : 
METHODS
From January 2015 to December 2015, we retrospectively analyzed the medical records of patients with solitary abdominal trauma from 17 institutions, including regional trauma centers in South Korea. Injured organ and degree of injury were confirmed by abdominal and pelvic CT or abdominal operation. Both blunt and penetrating abdominal injuries were included. We excluded patients who were dead upon arrival, those aged below 15 years, those who died within 24 hours of admission, and those with non-treatable diseases, such as cancer.
Age, sex, and time from injury to initial antibiotic administration were evaluated. To determine the extent and condition of a patient's injury, the Abbreviated Injury Scale (AIS, 2005; updated 2008) and New Injury Severity Score (NISS) of the abdomen were used to evaluate the injured organs and degree of injury. Initial status of the patient, transfusion confirmation, transfusion rate, initial use of antibiotic, dose of antibiotics, and duration of the initial therapy were investigated upon admission.
Moreover, we assessed the following; whether abdominal surgery and temporary abdominal closure or open abdomen were performed as well as operation time. At the time of surgery, the type of abdominal wound was identified, and the details of the abdominal organ injury were analyzed. The upper gastrointestinal tract includes the stomach, duodenum, and small intestine, and the lower gastrointestinal tract includes the colon and rectum.
The type and extent of wound infection after surgery were investigated. Infection was defined as an infection that occurred within 2 weeks after surgery, and as a case of having an infection through medical records or a consultation with an infectious disease doctor. The types of infection were classified into superficial and deep SSI, organ SSI, and non-SSI, and were configured to allow multiple selections. It was checked whether the causative bacteria were identified, and the method of confirming the strain was investigated. When the initial antibiotic was changed to another antibiotic, we identified when the antibiotic was changed and for what reasons.
Go to :
RESULTS
This study was approved beforehand by Institutional Review Board (IRB) of Gachon University (No. GCIRB2016-117), and the written informed consent was waived by IRB.
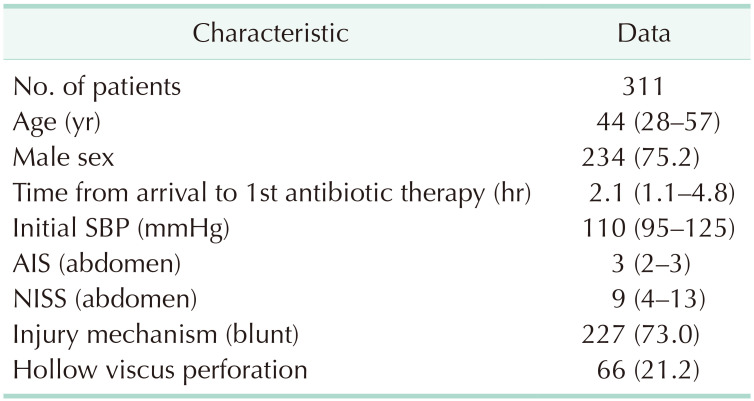
Data of the 311 patients were collected from 17 institutions. The median age of the participants was 44 years, and 75.2% were men. The median abdominal AIS was 3, and the NISS of the abdomen was 9. Approximately 73% of patients (n = 227) presented with blunt trauma. The median interval from arrival to the initial antibiotic treatment was 2.1 hours (Table 1).
The most common injured organ was the mesentery (22.8%), followed by the small intestine (19.0%), liver (18.3%), spleen (16.7%), and kidney (10.3%) (Fig. 1).

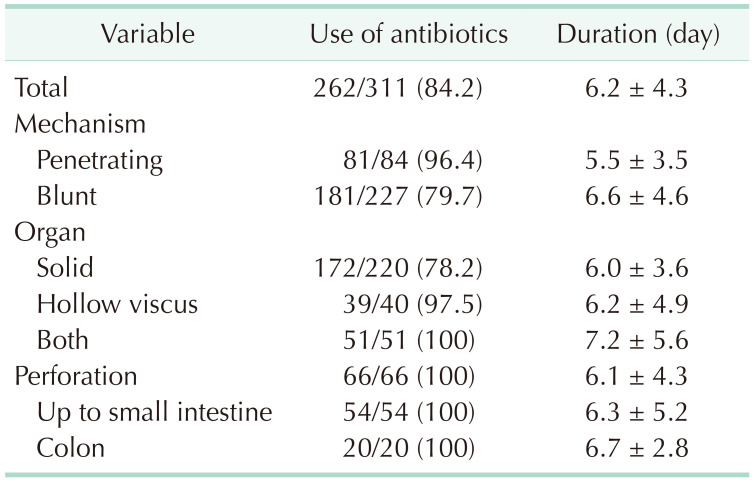
In terms of injury mechanism, the use of antibiotic was initiated in 96.4% of patients with penetrating injury and 79.7% with blunt injury. When classified according to the damaged organs, initially antibiotic therapy was provided to 78.2% of patients with solid organ injury and 97.5% with hollow viscus injury, and antibiotics were used in all cases of both solid and hollow viscus injuries (Table 2).
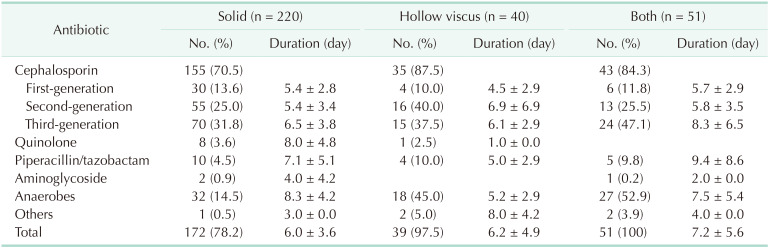
Antibiotics were used in 172 cases of solid organ injuries. Cephalosporin was commonly used in 70.5% of patients with solid organ injuries and 87.5% with hollow viscus injuries. Used cephalosporins were mainly second and third-generation drugs. Antibiotics for anaerobes were used mostly with cephalosporins. Moreover, such a drug is used in 14.5% of solid organ injuries, 45.0% of hollow viscus injuries, and 52.9% of both injuries. The mean day of using antibiotics was 6 days in solid organ injuries, 6.2 days in hollow viscus, and 7.2 days in both injuries (Table 3).
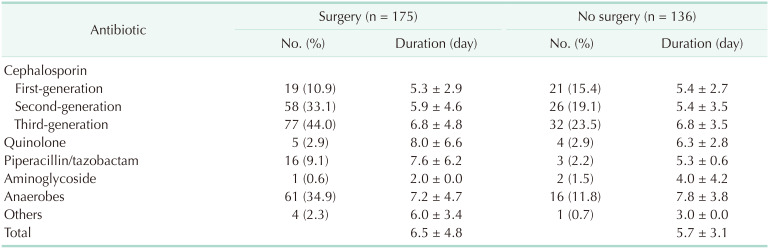
Among the antibiotics, 3rd generation cephalosporin (44.0%) are most commonly used antibiotics followed by 2nd generation cephalosporin (33.1%) (Table 4).
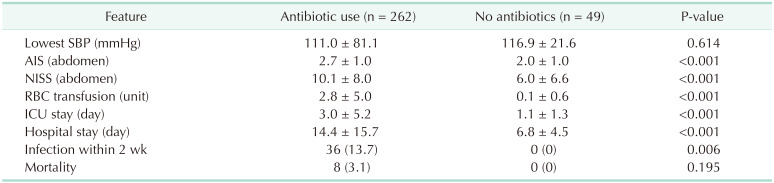
No difference was observed in the lowest systolic blood pressure when using the initial antibiotics and when not using the antibiotics; however, the AIS, NISS, and the amount of RBC transfusions were higher in the group who used antibiotics. Lengths of intensive care unit and hospital stay were longer in the group who used antibiotics (Table 5).
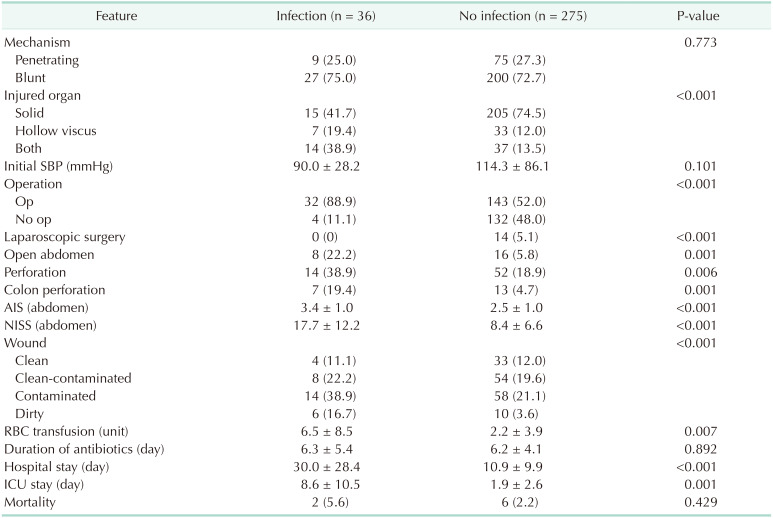
Infection within 2 weeks of admission occurred in 36 cases. Of these, 11 cases were organ space infections, 15 were superficial and deep wound infections, and the other 13 cases were non-SSIs. We compared the clinical manifestations according to the presence or absence of infection. Infection was related to injured organs, the presence or absence of the operation, the presence of open abdomen, the presence of bowel perforation and colon injury, and the degree of abdominal injury and the type of intraabdominal wound (Table 6). There was no infection in all cases (14 cases) with laparoscopic operation.
Go to :
DISCUSSION
We investigated initial antibiotic therapy in patients with isolated abdominal injuries in Korea and analyzed the incidence of infection. Through this study, we found that the rate of antibiotics use in Korea is excessively high and used for a long time, and the time of first administration is delayed. The rate of antibiotic use was 84.2%, and the mean duration was 6.2 days. Antibiotics were used in 79.7% and 96.4% of patients with blunt and penetrating injuries, respectively, and were utilized for a longer period in patients with penetrating injury.
Fullen et al. [8] have assessed the use of prophylactic antibiotics in abdominal injuries in 1972. In this study, the infection rate was lowest in the preoperative group, and the incidence rates of infection were 7% before surgery, 33% during surgery, and 30% after surgery. They have concluded that antibiotics should be administered as soon as possible after abdominal injury. In our data, antibiotics was injected about 6 hours after visit the hospital and used for 6.2 days. However, there was no difference in infection according to duration of antibiotics. We should inject antibiotics in a short time as soon as the patients visit the hospital. Although there have been numerous studies on the use of prophylactic antibiotics in individuals with abdominal trauma and the duration of therapy, only few large-scale prospective randomized trials have been conducted due to the nature of trauma [9101112131415161718].
In several studies and guidelines, the use of antibiotics in patients with blunt abdominal injuries has not been mentioned. In this study, antibiotics were used in 78.2% of patients with solid organ injury. In most guidelines, prophylactic antibiotics should be used only once in cases of penetrating injury if there are no serious infections and utilized within 24 hours in case of bowel perforation [5192021]. However, in this study, antibiotics were used for more than 6 days regardless of the mechanism or type of injured organ. We have been using antibiotics habitually for much longer than the guidelines or general recommendations, even for mild blunt injuries in solid organs. We should shorten the duration of using antibiotics.
Broad-spectrum antibiotics, which can be used against aerobic and anaerobic organisms, are preferred as initial antibiotics [620]. Second-generation cephalosporin is recommended, and third-generation cephalosporin is an alternative [7]. In this study, third-generation cephalosporin was most commonly used (31.5%) and second-generation cephalosporins were used next (25.0%). Therefore, there is a need for us to use appropriate antibiotics in the future.
In hollow viscus injury, the infection rate was high, so antibiotics must be used, but in solid organ injury, the infection rate was 6.8%. The mean score of AIS of the infection group was 3.4, so if an injury is more than 3 points, the use of antibiotics might be considered.
Infection occurred a lot in operation cases, especially in the open abdomen, twice as high (66.7% vs. 33.3%). Conversely, there was no infection in laparoscopic cases (0 of 14). If we are thinking about infection, it is advisable to reduce the open abdomen and perform laparoscopic surgery if possible. In addition, infection rate was high in case of emergency RBC transfusion, we should consider the use of antibiotics in patients requiring emergency transfusion.
This was a retrospective study and has several limitations. We had difficulties in identifying the process of using antibiotics and determining the cause of the infection. It was difficult to combine the data because the types of medical records and the degree of detail differ by institution. We performed a multivariate analysis to identify factors influencing infection, but it was difficult to find a relationship between infection and antibiotic use because there were not enough data on various causes that affect infection after surgery. Although this study did not include all hospitals in Korea, large hospitals including trauma centers participated in the study. The guidelines for the use of antibiotics for abdominal trauma in Korea were recently published [7]. Whether the antibiotics are used according to the guidelines should be confirmed, and the changes in the use of antibiotics and the differences in results must be analyzed through prospective studies.
In conclusion, antibiotics are used extensively and for long duration in patients with abdominal injury in Korea. Second- and third-generation cephalosporin is the most used antibiotics. So, we should consider one-time injection right after visiting hospital in cases with hollow viscus injury and operation. Laparoscopic surgery is better in infection prevention if possible. If severity of injury is high above AIS 3 or in cases with RBC transfusion, we should consider antibiotics use even without hollow viscus injury or operation.
Go to :
 XML Download
XML Download