

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neurogenic thoracic outlet syndrome (TOS) is a disease of compressive peripheral neuropathy of the upper limb, and its pathogenesis, diagnosis and treatment are often under- or mis-diagnosed.1 It is a syndrome, rather than a disease, with various atypical symptoms due to persistent compression of the neurovascular bundle involving the thoracic outlet and its anatomical structure is very complex, leading to more misdiagnosis.1,2
TOS is generally caused by congenital malformations such as cervical rib, trauma including traffic accidents, and abnormal postures or motions, which lead to compression of nerves and vessels.3 TOS due to abnormal posture including abduction and external rotation of the arm can be prevented simply by posture correction without any surgical management. We report a patient with progressive tingling sensation and intrinsic muscle atrophy of the right hand, which was diagnosed as true neurogenic TOS by electrophysiologic studies.
Go to : 
CASE REPORT
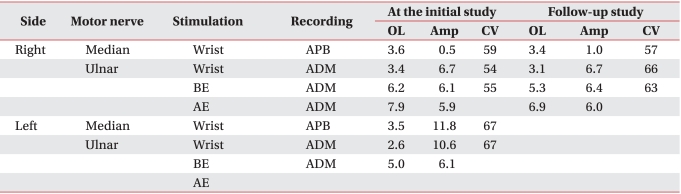
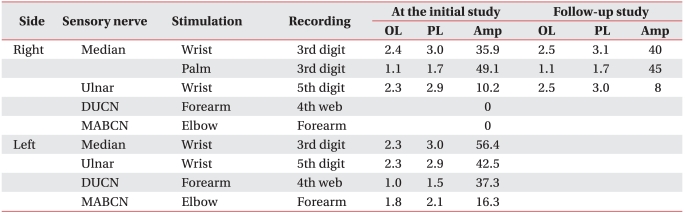
A 30-year-old woman visited the hospital for gradually progressing tingling sensation in her right 5th finger and right shoulder pain, which developed after receiving a cesarean section procedure one year previously. She experienced intermittent pain on her right shoulder and wrist area for 10 years and atrophy of her right hand intrinsic muscles appeared 2 years ago. There was no history of trauma or systemic disease. After recording a detailed history, a chronic sleep habit of abnormal posture with hyperabduction of the right shoulder was revealed. With severe atrophy of the right hand intrinsic muscle (Fig. 1-A), manual muscle testing based on the Medical Research Council grade of right abductor pollicis brevis muscle was decreased to grade 1, abductor digiti minimi muscle and 1st dorsal interosseous muscle, grade 4. Hypesthesia on the right medial arm and forearm, and dorsal and palmar aspect of the ulnar side of the hand and the 4th and 5th fingers was observed (Fig. 1-B). Temperature decrease or edematous change of the right hand was not observed. Provoked test for carpal tunnel syndrome or ulnar neuropathy at the elbow including Phalen test, Froment sign, and Tinel signs of median nerve at the wrist and ulnar nerve at the wrist and elbow were all negative. Loss of radial artery pulse was noticed in Adson's and Wright's test. Roos stress test showed positive findings. Under impression of TOS, nerve conduction studies and needle electromyographic examination were conducted. In a conduction study, decreased amplitude and prolonged latency of compound muscle action potential (CMAP) of median nerve and sensory nerve action potential (SNAP) of ulnar nerve was observed (Fig. 2-A, D). Right ulnar CMAP was within normal range, yet was decreased compared to the left side (Fig. 2-B, C). Dorsal ulnar cutaneous and medial antebrachial cutaneous SNAPs were unobtainable. In needle electromyography, abnormal spontaneous activities and/or large motor unit potentials were observed in C8 and T1 segment innervated muscles including abductor pollicis brevis, abductor digiti minimi, 1st dorsal interosseous, and extensor indicis muscles. Abnormal spontaneous activity was not observed in cervical paravertebral muscles. Additional studies were performed to evaluate the causes of neurogenic TOS and presence of vascular TOS. Cervical rib was not found in plain radiography and abnormal findings were not observed in the neck MRI and arteriogram (Fig. 3-A, B). However, a venogram showed mild compression of the right subcalvian vein around the thoracic outlet during shoulder abduction (Fig. 3-C, D). Due to absence of edema, color change or cold sensation of upper extremity, venous TOS was excluded. She was diagnosed as true neurogenic TOS due to repetitive abnormal sleeping posture with hyperabducted shoulder. Posture correction education and conservative treatment including physical therapy and trigger point injection was performed. She did not complain of any symptom aggravation, and there was no interval change on the follow-up electrophysiologic study after 4 years (Table 1, 2).
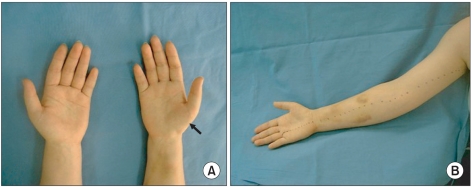 | Fig. 1(A) The right hand thenar muscle was atrophied (arrow). (B) Sensation on the medial side of the arm and forearm and little finger (medial to the dot line) was decreased.
|
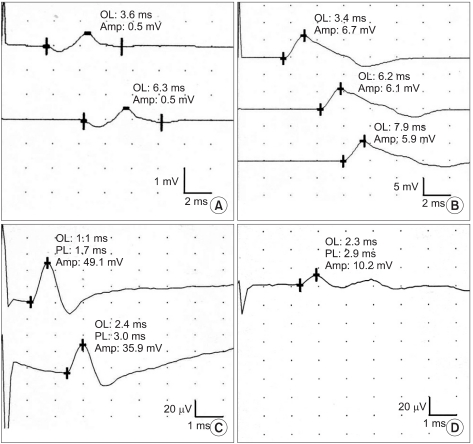 | Fig. 2(A) The right median motor response was of low amplitude. (B) The right ulnar motor response was normal. (C) The right median sensory response was normal. (D) The right ulnar sensory response was of low amplitude.
|
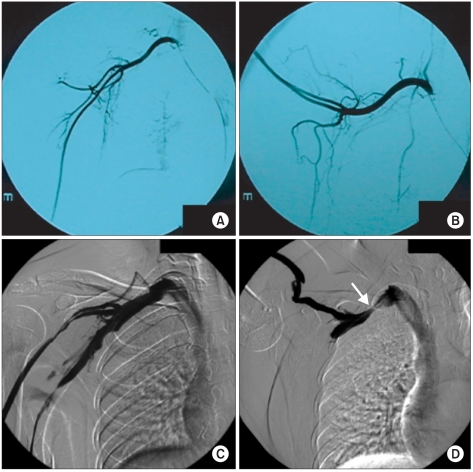 | Fig. 3Arteriogram demonstrated no compression of subclavian artery during shoulder abduction (A, B), but venogram showed compression of the right subcalvian vein around the thoracic out during shoulder abduction (arrow) (C, D).
|
Go to :
DISCUSSION
TOS is a syndrome complex that causes pain, tingling sensation, hypesthesia, muscle atrophy and edematous changes in the upper extremities due to compression of neurovascular bundles in the course of thoracic outlet from neck to axillar region. It is classified into vascular and neurogenic TOS according to the anatomical pathomechanism. Recently, vascular causes are subdivided into arterial or venous TOS and, neurogenic causes into true or disputed neurogenic TOS based on clinical symptoms and studies. Among the classified syndromes, true neurogenic TOS is known to have lower prevalence and can easily be misdiagnosed as cervical intervertebral disc herniation, ulnar neuropathy or carpal tunnel syndrome due to similar clinical findings.4
Le Forestier et al.5 reported 6 patients with true neurogenic TOS whose diagnosis was confirmed by surgery. Among 6 patients, 4 patients were clinically diagnosed as carpal tunnel syndrome, cervical radiculopathy and motor neuron disease before electromyography study and 2 were found to have cervical rib, but the diagnosis of neurogenic TOS was made only after performing electromyography. This requires nerve conduction studies and needle electromyographic examination for the differential diagnosis of true neurogenic TOS from diseases with similar clinical characteristics. In general, nerve conduction studies show a decrease in median CMAP and ulnar SNAP amplitude with normal median sensory and ulnar motor, and needle electromyography typically shows denervation potentials in abductor pollicis brevis and hand intrinsic muscles.6 A recent study emphasizes the importance of medial antebrachial cutaneous sensory conduction. Kothari et al.7 reported that MABCN conduction study is a more sensitive test than ulnar sensory nerve due to the predominant portion of T1 segment. In our case, electrophysiologic studies were compatible with true neurogenic TOS.
Compression of nerves by cervical ribs is known to be one of the common causes of true neurogenic TOS along with trauma, scalene muscle hypertrophy and repetitive motions causing irritation of the nerve. Almeida et al.8 and Katirji and Hardy9 reported a case of true neurogenic TOS in swimmers. In swimmers, scalene muscle hypertrophy due to repetitive use of neck and shoulder muscles was considered to be a cause of nerve compression. Stockstill et al.10 reported high risk of TOS in dentists who require shoulder abduction and external motion in clinical practice. In our case, we observed that patients had a habit of abnormal sleeping posture, with hyper-abduction of the shoulder and was considered the main cause of nerve compression. Unlike previous cases, whose causes were repetitive motions in vocational practice, the cause was due to abnormal posture in everyday life. Correcting an everyday life habit is not a difficult task, and such conservative measures can prevent or even cure disease. Therefore, it is important to fully evaluate the causes. The patient had a correction of sleeping posture and received conservative treatment including physical therapy with levator scapula muscle strengthening and pain control, and trigger point injections. After correction of sleeping posture, pain decreased but there was no change in sensory or muscle strength. Follow-up electrophysiologic studies did not demonstrate any progression of disease. Although we considered 1st rib resection as a treatment plan, our expectation for its effect on chronic nerve damage was low and she also refused surgical treatment. Only conservative management was then taken.
Diagnosis and treatment of TOS is not an easy task. For prevention of symptoms and disease progression, adequate diagnostic and therapeutic measures are required. Several causes of true neurogenic TOS have been reported. Even everyday life postures can be causes, as in our case. It is of importance to be aware of such causes in evaluating true neurogenic TOS, for only mild correction of posture habit can relieve symptoms.
Go to :
 XML Download
XML Download