

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dysphagia is a major complication known to develop in 37-78% of stroke patients1 which interferes with processes that transfer food material from the oral cavity to the stomach because of neurologic or structural disorders. Decreased laryngeal elevation due to weakened muscles involved in the swallowing process is a main cause of dysphagia in brain-injured patients, which can result in subglottic aspiration while swallowing.
Several methods have been established to treat dysphagia, and neuromuscular electrical stimulation (NMES) is one such method widely applied in the clinical setting. NMES of the pharyngeal area is known to strengthen the swallowing-related muscles by contraction in patients with dysphagia. Burnett et al.2 achieved laryngeal elevation in normal volunteers by stimulating the mylohyoid, geniohyoid, and thyrohyoid muscles using a hooked wire electrode. Leelamanit et al.3 also found that synchronized surface electrical stimulation of the thyrohyoid muscle with swallowing has a therapeutic effect in dysphagia patients who did not improve with conventional treatment. Kim et al.4 applied electrical stimulation to the digastric and thyrohyoid muscles and found that functional dysphagia scale values between pre-treatment and 4 weeks following treatment were 13.20 (43.80-30.60) in the electrical stimulation group and 10.25 (32.75-22.50) in the sham stimulation group.
However, other studies reported that pharyngeal electrical stimulation to the degree of contracting muscles lowers the hyoid bone by contracting the sternohyoid and omohyoid muscles, thereby interfering with the swallowing process.5,6 Humbert et al.6 reported that 'submental (suprahyoid) region-only' stimulation as well as stimulation of 'both submental and laryngeal (infrahyoid) regions simultaneously' at rest lowered the hyoid bone and larynx compared to the position before stimulation among healthy adults. However, paired stimulation of the submental region moved the hyoid bone upward compared to the stimulation of the laryngeal region. Kim and Han7 also reported that the degree of hyoid elevation during stimulation of the suprahyoid area was 66.8% greater than that during liquid swallowing among normal individuals. Based on these past studies, we aimed to evaluate the effect of repetitive NMES of the suprahyoid muscles for treating dysphagia in brain-injured patients with reduced laryngeal elevation.
Go to : 
MATERIALS AND METHODS
Materials
This study had a prospective, non-concurrent control comparative design. Among patients with dysphagia admitted to Seoul National University Hospital between January 2006 and July 2007, twenty-eight individuals (26 stroke and two traumatic brain injury patients) were enrolled who met the following criteria: (1) VFSS showing reduced laryngeal elevation during swallowing (judged by three rehabilitation physicians), (2) VFSS showing supraglottic penetration or subglottic aspiration when swallowing 2 ml of 50% liquid barium (Solotop® suspension 140) solution, and (3) no clinical evidence of vagus or glossopharyngeal nerve palsy in addition to the inclusion criteria from the VitalStim® manual.8
Only conventional dysphagia management (CDM) without electrical stimulation therapy was applied to patients admitted between January 2006 and March 2007 as a control group. Electrical stimulation of suprahyoid muscles (ESSM) was performed on patients between April 2007 and July 2007. Patients who received electrical stimulation also underwent CDM.
Methods
The protocol of this study was approved by the institutional review board of Seoul National University Hospital. The VDS9 and ASHA NOMS swallowing scale (ASHA level)10 were used as parameters for evaluating swallowing function. The VDS (from 0 to 100) was determined using videofluoroscopic analysis, and consisted of several factors such as subglottic aspiration and food residues. This scale was reported to be sensitive and specific for detecting supraglottic penetration and subglottic aspiration, and was considered useful for predicting persistent dysphagia after stroke.11 The ASHA level is a measurement of both the supervision level required and diet level that intuitively reflects a patient's functional status.10
Treatments were performed for 30 minutes per day, 5 days per week for 4 weeks by three experienced occupational therapists who shared treatment protocols. Three rehabilitation physicians with considerable experience in the management of dysphagia (a senior professor, clinical fellow, and second-grade resident physician) determined the VDS and ASHA level before and after treatment with consensus. The VFSS was performed in a manner previously described9 and the VDS was determined while the patients swallowed 2 ml of a 50% liquid barium solution.
Conventional dysphagia management consisted of ice cube training, double swallowing, effortful swallowing, Mendelsohn maneuver, and thermal tactile stimulation. If a patient could not swallow an ice cube without overt aspiration symptoms, ice cube training was excluded from CDM. All patients were sufficiently conscious to perform effortful swallowing and the Mendelsohn maneuver. STIMPLUS DP200® (Cybermedic Corp., Iksan, South Korea) was used for suprahyoid NMES. The stimulation parameters used were 60 Hz of 500 microsecond duration with intermittent stimulation (1 second on and 1 second off) to avoid laryngeal spasms and to simulate normal pharyngeal swallowing. The active electrodes were placed at midpoints between the bilateral edges of the hyoid and chin, whereas the reference electrodes were placed at midpoints between the bilateral mandibular angle and chin (Fig. 1). The locations of active electrodes were at the points considered near to the motor point of the anterior belly of the digastric muscle. This was because we had previously shown that surface electrical stimulation moved the hyoid bone anteriorly and superiorly during stimulation using this electrode geometry in normal volunteers.7 Stimulus intensity was started at 3 mA and increased by 1 mA. When a volunteer expressed discomfort but not pain, we administered the stimulus at this intensity three times to allow adaptation to the electrical stimulus. When a volunteer continued to complain about discomfort or pain, we defined the stimulus intensity used prior to the patient's complaint as the maximal tolerable intensity. We administered stimulation of the maximal tolerable intensity for 30 minutes using a 1 second on/1 second offcycle.

SPSS version 12.0 (Chicago, IL, USA) for Windows was used for statistical analysis. The Mann-Whitney U test was used to confirm that initial swallowing function, patient age, and post-brain injury dysphagia onset were similar between the CDM and ESSM groups. To compare the degree of VDS score changes between the two groups, the Mann-Whitney U test was also used. Fisher's exact test was performed to compare the prevalence of ASHA level improvement in the CDM and ESSM groups. p-values less than 0.05 were considered statistically significant.
Go to :
RESULTS
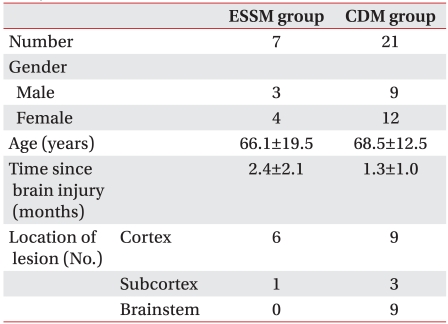
Seven patients were selected from the ESSM group and 21 from the CDM group. The average ages of patients were 66.1±19.5 for the ESSM group and 68.5±12.5 years for CDM group. The pre-treatment VDS was not significantly different (p=0.876) nor was the average patient age between the two groups (p=0.959). The time from brain injury to enrollment in this study was 2.4±2.1 months for the ESSM groups, which tended to be longer than the 1.3±1.0 months for the CDM groups but was not statistically significant (p=0.249). Six patients in the ESSM group and nine in the CDM group had cortical lesions. One patient in the ESSM group and three in the CDM group had subcortical lesions, whereas all nine patients with brainstem lesion in our study were in the CDM group (Table 1). Maximal tolerable intensities varied from 5-12 mA in the ESSM group. Possible side effects of electrical stimulation therapy for dyaphagia including skin burns, pain, cardiovascular problems due to vagus nerve activation, and laryngeal spasm have been reported previously.12,13 In this study, however, no significant side effects were encountered other than transient pain which disappeared immediately after cessation of electrical stimulation.
Videofluoroscopic dysphagia scale (VDS)
The VDS score decreased from 29.8±13.5 to 17.9±7.8 in the ESSM group, and from 29.2±15.5 to 16.6±11.8 in the CDM group (Fig. 2). There was no significant difference between groups (p=0.796, Mann-Whitney U test). One patient in the ESSM group (patient No. 7) showed an increase in VDS score after treatment. This paradoxical VDS increase was caused by a newly developed premature bolus loss during liquid swallowing due to a dental prosthesis, and there were no findings such as motor weakness or dysarthria due to a new brain lesion.
 | Fig. 2VDS and ASHA levels in all patients before and after treatment. (A) VDS in the ESSM group. (B) VDS in the CDM group. (C) Comparison of △VDS between the ESSM and CDM groups. (D) ASHA level in the ESSM group. (E) ASHA level in the CDM group. (F) Comparison of △ASHA level between the ESSM and CDM groups. N.S.: Not significant.
|
ASHA NOMS swallowing level
Six patients (85.7%) in the ESSM group and 14 patients (66.7%) in the CDM group showed improved ASHA levels (Fig. 2), but there was no significant difference observed between the ESSM and CDM groups (p=0.633, Fisher's exact test).
Go to :
DISCUSSION
The use of NMES is becoming popular in clinical settings as several studies have been reported showing that pharyngeal NMES is effective for treating dysphagia in brain-injured patients. Carnaby-Mann and Crary14 performed a meta-analysis to examine the therapeutic effects of pharyngeal NMES on swallowing ability, and concluded that electrical stimulation tended to improve swallowing function. Freed et al.12 and Blumenfeld et al.15 reported that pharyngeal electrical stimulation is superior to CDM, and suggested that possible reasons were increase of local blood flow, reduced edema through decreased extracellular fluid, recruitment of more motor units than volitional contractions, selective activation of type II muscle fibers, and improvement of swallowing function by stimulating the sensory cortex of the cerebrum.15 Furthermore, Gow et al.16 found increased activities in the lateral cerebral cortex (Brodmann area 4, 1, and 2) after pharyngeal electrical stimulation in healthy volunteers which were confirmed by brain MRI and co-registered magnetoencephalography. Although pharyngeal NMES has been performed previously to strengthen swallowing-related muscles and reactivate neural pathways, the exact mechanism by which pharyngeal NMES improves dysphagia is not fully understood. Our study was designed to test whether the elevation of the hyoid bone improves swallowing function by applying electrical stimulation to suprahyoid muscles, whereas the above mentioned studies performed electrical stimulation of the thyrohyoid muscle.
The most likely reasons why repetitive NMES of the suprahyoid muscles in this study had no additive effect include the following. Surface electrical stimulation could be insufficient to strengthen the suprahyoid muscle although we observed anterior and superior displacement of hyoid bone by videofluoroscopy during the electrical stimulation. Suiter et al.17 found that stimulation at high frequencies such as 80 Hz can be inadequate for recruiting motor units involved in the swallowing process because the response of submental muscles to electrical stimulation is frequency-specific. Another study revealed that low frequency stimulation below 5 Hz is useful to treat dysphagia.18 Thus, the 60 Hz stimulation that we used in this study may not have been adequate. Since the ASHA level tended to increase more in the ESSM group than in the CDM group, electrical stimulation may be effective for improving swallowing function although there was no statistically significant difference. However, because this study included patients in the subacute phase (early stage of brain injury), spontaneous neurologic recovery might have masked the therapeutic effects. Although we selected the patients with similar post-onset periods of brain injury as a control group, limitations associated with adjusting for the effects of spontaneous neurologic recovery still remained.
When Type 1 error was assumed to be 0.05, the power of this study was found to be low when determined using the PASS 2008 (NCSS, Utah, USA) because of the small sample size. Other limitations of this study included using a non-concurrent control group instead of a concurrent one, not checking suprahyoid muscle activity by electromyography during swallowing before or after treatment, and not comparing hyoid bone elevation and epiglottic rotation using a quantitative method by analyzing the videofluoroscopic results before or after treatment. Therefore, to explore the effect of repetitive NMES of the suprahyoid muscles on dysphagia more thoroughly, studies with a larger sample size and concurrent control group need to be conducted using quantitative methods.
Go to :
CONCLUSION
Although repetitive NMES of the suprahyoid muscles did not further improve swallowing functions in patients with dysphagia and decreased laryngeal elevation, more patients had an improved ASHA level in the ESSM group than in the CDM group. Further studies with a larger sample size and concurrent control group are required to comprehensively establish the effects of repetitive NMES of the suprahyoid muscles on patients with dysphagia.
Go to :
 XML Download
XML Download