

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) was first reported in Wuhan, China1 and subsequently spurred a global pandemic that is still ongoing. Since the outbreak, several mRNA-based and adenovirus-vectored COVID-19 vaccines have been developed and were proved to be very effective in preventing COVID-19 illness.2 It was predicted that the pandemic would end when the vaccination rate reached a sufficient level and herd immunity was achieved34; however, most countries are having difficulty reaching such a level of vaccination.5 As the COVID-19 pandemic is prolonged, new variants continue to appear.6 The delta variant has been particularly contagious, possibly due to the mutation in the spike protein, and breakthrough infection with this variant has been reported even among fully vaccinated people.78 Since July 2021, the delta variant has become the dominant strain in Korea, accounting for more than 50% of the confirmed COVID-19 cases.9 For more than 3 months, more than 1,000 new COVID-19 cases per day (total population: approximately 52 million) have been confirmed, while the vaccination rate has remained low, at approximately 14% in early August 2021.10
The Korean military is made up of more than 540,000 workers, including soldiers completing 18–21 months of mandatory military service, officers (commissioned, non-commissioned, and warranted), and civilian employees. The daily activities of these workers often involve working and training in confined spaces, and not wearing masks properly during daily exercise; thus, they are considered to be vulnerable to COVID-19. Therefore, the military began mass COVID-19 vaccination on April 28, 2021. In cooperation with the Korea Disease Control and Prevention Agency (KDCA), the military was able to fully vaccinate over 85% of all personnel as of August 8, 2021. However, because almost all trainees that have newly joined the military have been unvaccinated, clusters of COVID-19 infection have occasionally occurred at the training camps despite high vaccination rates. In addition, because military officers commute to work, community infection of COVID-19 continues to occur.
Even though previous studies have shown a decreased effectiveness of COVID-19 vaccines against the delta variant, vaccines remain over 60% effective.11 Additionally, the effectiveness of the vaccines in preventing severe/critical infection and reducing hospitalizations cannot be overemphasized.12 In the current study, to confirm the effectiveness of mass vaccination programs, we analyzed the pattern of confirmed COVID-19 cases in Korean military units. Additionally, trends in the incidence rates of COVID-19 in the military and the entire Korean population were compared.
METHODS
Study design
The Korean military can be classified into four groups: army, navy, air force, and marine corps. Epidemiological investigation data were collected regarding confirmed COVID-19 cases from August 1, 2021 to September 15, 2021 in units belonging to the four military groups. Data were compared for the units that were believed to have achieved herd immunity (i.e., ≥ 70% vaccination) and those that were not believed to have reached herd immunity (< 70% vaccination), including the training camps in which cluster infection occurred. Since the end of July 2021, the average vaccination completion rate of the military personnel has already become over 80%. The number of confirmed cases, locally transmitted cases, and vaccine breakthrough infections, as well as the number of military personnel in the units and the vaccination rates of units, were retrospectively reviewed. In addition, the incidence rates in the military and the entire country of Korea13 were compared.
Diagnostic test of COVID-19 and test of variants
Confirmed COVID-19 cases were defined as those diagnosed by real-time reverse transcriptase-polymerase chain reaction (qPCR) tests of respiratory specimens.14 Tests were conducted in accordance with KDCA guidelines using kits (Real-Q Direct SARS-CoV-2 Detection Kit, Real-Q SARS-CoV-2 Detection Kit by BioSewoom, and STANDARD M nCoV Real-Time Detection Kit; SD BIOSENSOR, Suwon, Korea) and instruments (CFX96; Bio-Rad, Hercules, CA, USA) approved by the Ministry of Food and Drug Safety of the Republic of Korea. The test of COVID-19 variants was performed using a nucleic acid amplification and sequencing method on the spike protein gene region of SARS-CoV-2, from 95 to 681 amino acids of the spike protein. This variant test was conducted by the Armed Forces Medical Research Institute.
Definitions
Participants were considered fully vaccinated two weeks after completion of two doses of vaccination (or one dose for the Ad.26.COV2.S vaccine),15 and breakthrough infection was defined as a case in which a fully vaccinated individual was diagnosed with COVID-19. Locally transmitted cases were defined as cases in which an individual first tested negative on a qPCR test that was performed immediately after close contact with confirmed COVID-19 patients, but then tested positive during isolation. As it was not possible to precisely identify the medical condition of each confirmed case, all cases were reviewed whether the confirmed patient was admitted to the hospital or to non-hospital community treatment centers where patients with mild COVID-19 were isolated.1617 If subjective respiratory symptoms were severe, pneumonia was confirmed by chest X-ray, and if the oxygen saturation level decreased, the patient was hospitalized. The incidence rate was defined as the number of new cases of COVID-19 per one million person-days based on the confirmed date. As KDCA set the target vaccination rate of 70% as the cut-off for lessening social distancing,18 units in which more than 70% of military personnel were fully vaccinated were considered to have achieved herd immunity.
Vaccination strategy in the Korean military
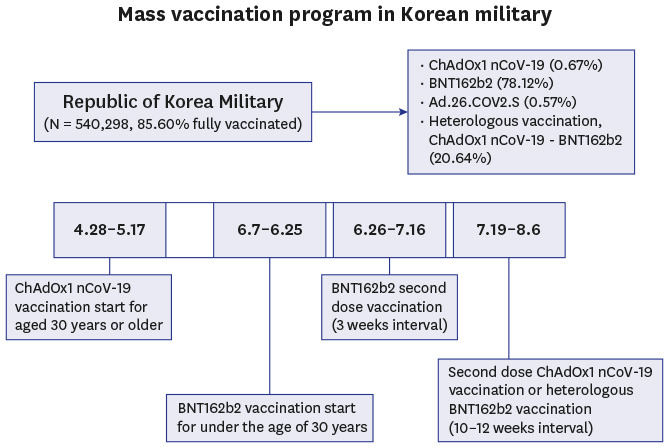
Since the KDCA recommended the ChAdOx1 nCoV-19 vaccination only for those aged 30 years or older because of the risk-benefit analysis for thrombosis with thrombocytopenia syndrome related to the vaccine,19 those under the age of 30 years were administered the BNT162b2 vaccine. The mass vaccination schedule is presented in Fig. 1A. The BNT162b2 vaccine was administered twice, with 3 weeks between doses. In contrast, the ChAdOx1 nCoV-19 vaccine was administered twice, with a recommended 4–12 weeks between doses, but a 10–12-week interval between doses was strongly recommended by the KDCA.20 Instead of the second doses of the ChAdOx1 nCoV-19 vaccine, a heterologous vaccination with the BNT162b2 vaccine could be administered per the individual's choosing. Few employees aged 30 years or older received a single dose of Ad.26.COV2.S vaccine (0.57%, Fig. 1B).
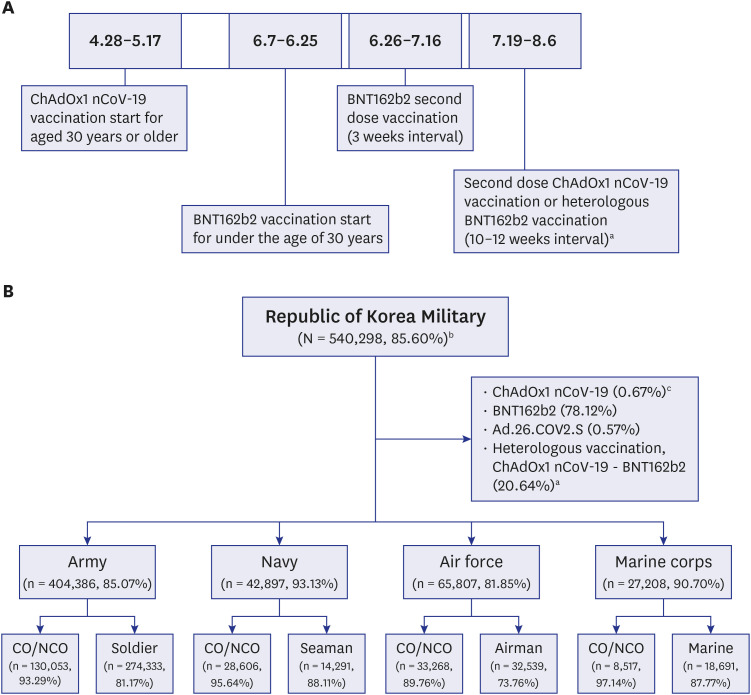
Fig. 1
(A) Mass vaccination program in Korean military. (B) Classification of Korean military and COVID-19 vaccination rates.
COVID-19 = coronavirus disease 2019, CO = commissioned officer, NCO = non-commissioned officer.
aMilitary personnel aged 30 years or older who received the first dose with ChAdOx1 nCoV-19 were given a second dose with ChAdOx1 nCoV-19 or BNT162b2 depending on the individual's choice.
bRates of fully vaccinated personnel; fully vaccinated status was defined as 2 weeks after completion of two doses of the vaccine (or one dose for Ad.26.COV2.S vaccine).
cThe rate of each vaccine on August 17.
![]()
Non-pharmacological intervention (NPI) in the Korean military
Contact tracing was conducted when a confirmed patient with COVID-19 was found in a battalion, and personnel who had close contacts with the individual within 72 hours prior to symptom onset of the confirmed patient were qPCR tested for COVID-19 and isolated. Isolation lasted for 14 days, and if symptoms did not develop, the individuals were released from isolation after a qPCR test on day 13 (1 day before release; total qPCR tests for close contacts = 2) was confirmed to be negative. However, for fully vaccinated individuals, if it was confirmed that the index case was not a delta variant, they were immediately released from isolation. Additionally, personnel in the same battalion who had not been in close contact with the infected individuals could only resume work after they were confirmed to be negative. Therefore, one confirmed COVID-19 often caused more than one battalion to be tested.
All personnel were required to wear masks within the unit, and face-to-face meetings with more than five people were avoided as much as possible. Although soldiers lived on base, military officers commuted to work, but private gatherings of more than five people were prohibited after work for officers. Leaves were allowed for less than 20% of the total members of the unit per day, and in case of more than 5 days of leave, a qPCR test was performed upon returning to the unit. Periodic qPCR test was not performed on asymptomatic personnel unless they had close contact with patients with confirmed COVID-19, per the KDCA guidelines.21
Statistical analysis
The clinical characteristics were compared of units believed to have achieved herd immunity (≥ 70% of their members fully vaccinated) and units believed to have not. Student’s t-tests were used to compare continuous variables, and chi-squared tests were used to compare categorical variables. To confirm the association between the number of confirmed COVID-19 cases in each unit during the observation period and the vaccination rate, a Pearson’s correlation analysis was performed. To explore the association between the rate of fully vaccinated patients among confirmed cases in units and the rate of the delta variant in Korea, a nonparametric Spearman's rank correlation analysis was performed. Statistical significance was set at P < 0.050. The analyses were performed using IBM SPSS Statistics Version 26.0 (SPSS Inc., Chicago, IL, USA) and a plot of the data was constructed using the Coin packages in R version 4.1.1 (R Core Team, Vienna, Austria). Graphs were created using GraphPad Prism 8.0.2.
RESULTS
Association between confirmed COVID-19 cases and the vaccination rates of the units
The classification of the Korean military is presented in Fig. 1B. The vaccination rates listed in this figure are current as of September 15, 2021, when the vaccination rate of the entire military was at 85.60%.
Fig. 2 and Supplementary Table 1 show the association between the number of confirmed COVID-19 cases from August 1 to September 15, 2021, and the vaccination rates of each unit. A total of 39 military units had confirmed cases during this time. There was a statistically significant negative correlation between the two variables (Pearson's r = –0.78, P < 0.001). Of the total of 722 military personnel in the two training camps where cluster infection occurred, 456 of the personnel were trainees, and only 1 of them was fully vaccinated (Supplementary Table 1).
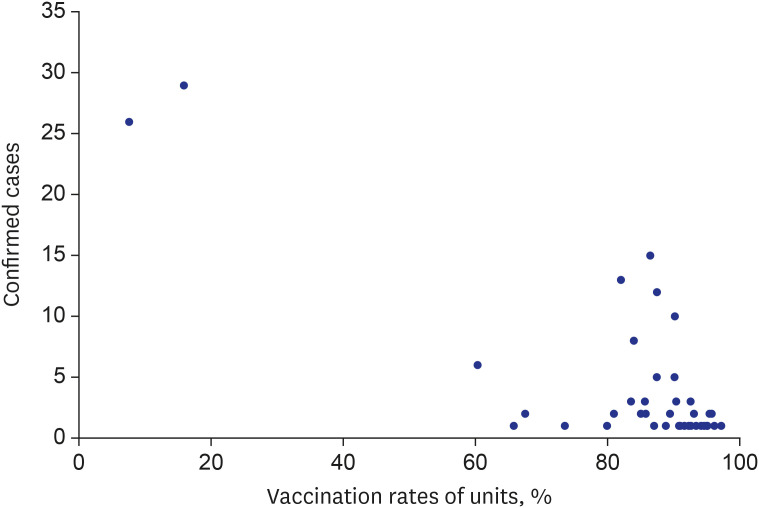
Fig. 2
Association between the number of confirmed COVID-19 cases and the vaccination rates of each military unita from August 1 to September 15, 2021.
COVID-19 = coronavirus disease 2019.
aWith the exception of two units (battalion) where cluster infections occurred, the units with confirmed COVID-19 cases were reviewed on the scale of the corps.
![]()
Comparison of confirmed COVID-19 cases between the units that achieved herd immunity and the units that did not
The military units in which confirmed cases occurred were divided into two groups based on their vaccination rates (< 70% or ≥ 70%) and compared (Table 1). Among the 174 confirmed COVID-19 cases identified within the military (110 [63.22%] in 34 herd immunity units vs. 64 [36.78%] in 5 non-herd immunity units), 40 cases were tested for variants, and 26 cases (65.00%) were identified as delta variants. As for locally transmitted cases, one case (0.91%) was found in the units that had achieved herd immunity and 39 cases (60.94%) were identified in the units that had not achieved herd immunity. The rate of hospitalization of individuals with confirmed cases in the non-herd immunity group (27.08%), was more than double that of the herd immunity group (11.01%). There was no significant difference between the two groups in the number of military personnel in each unit (herd immunity group vs. non-herd immunity group, mean; 11,227.68 vs. 8,211.40; P = 0.641), but units that had achieved herd immunity had a significantly higher mean percentage of officers (49.87% vs. 22.96%; P = 0.013). The mean rate of fully vaccinated personnel in the units that had achieved herd immunity (89.42%) was more than double that of the other group (43.45%; P = 0.024). The mean incidence rate per unit appeared lower in the herd immunity group, but the difference was not statistically significant (cases per million person-days; 13.02 vs. 743.30; P = 0.203). Meanwhile, the mean rate of vaccine breakthrough infection among confirmed COVID-19 cases was higher in herd immunity units (86.76%) than non-herd immunity units (23.33%; P < 0.001).
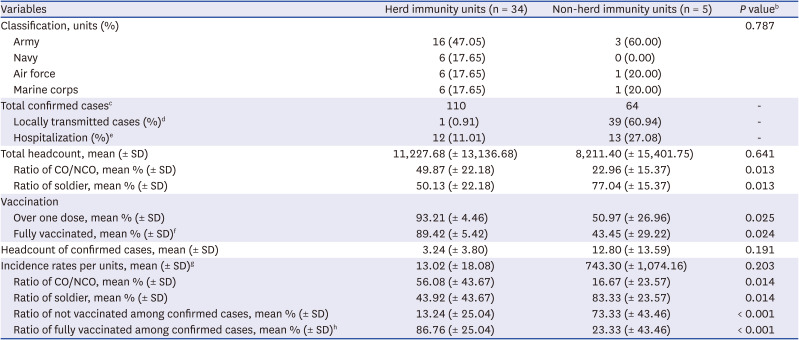
Table 1
Comparison of confirmed COVID-19 cases in units that had and had not achieved herd immunity from August 1 to September 15, 2021a
COVID-19 = coronavirus disease 2019, SD = standard deviation, CO/NCO = commissioned officer/non-commissioned officer.
aIf more than 70% of military personnel were fully vaccinated, the units were considered to have achieved herd immunity.
bStudent’s t test for continuous variables and the χ2 test for categorical variables.
cTotal confirmed, locally transmitted, and hospitalized cases were not the average for each unit, but the total number of cases in each group (herd immunity vs. non-herd immunity). Among the 174 COVID-19 cases in the military, 40 cases were tested for variants, and 26 cases (65.00%) were identified as the delta variants.
dLocally transmitted cases were defined as the close contacts who tested negative via a real-time reverse transcriptase polymerase chain reaction (qPCR) test was performed immediately after contact with a confirmed patient, but became a qPCR test positive during isolation.
eHospitalized cases are defined as confirmed patients admitted to a hospital (not a community treatment center). One within herd immunity group and 16 in non-herd immunity group were missing cases.
fFully vaccinated status was defined as 2 weeks after completion of two doses of vaccination (or one dose for Ad.26.COV2.S vaccine).
gIncidence rates were defined as the number of confirmed COVID-19 cases per one million person-days in each unit.
hSame as the vaccine breakthrough infection cases.
![]()
COVID-19 infections among non-vaccinated personnel were analyzed to determine whether their position as an officer (vs. soldier) affected the likelihood of COVID-19 infection beyond their vaccination status (Supplementary Table 1). Except for units No. 1 and 2, in which cluster infections occurred, the rate of infection of officers in each of the remaining 37 units unit had a mean of 48.42%. Of the 119 confirmed COVID-19 cases, 56 (47.06%) were officers, and among non-vaccinated personnel, 13 (41.94%) of the 31 COVID-19 cases were also officers.
Trends of the confirmed COVID-19 cases in the military units
Fig. 3 shows the daily number of confirmed COVID-19 cases and the weekly rates of breakthrough infection for all military units. In Fig. 3A, except for August 4 and 6, when cluster infections occurred, the percentage of those who were fully vaccinated among the confirmed cases increased over time. There was a statistically significant positive correlation between the increase in the delta variant in Korea22 and the rates of breakthrough infection (Spearman's ρ = 0.86, P = 0.014; Fig. 3B).
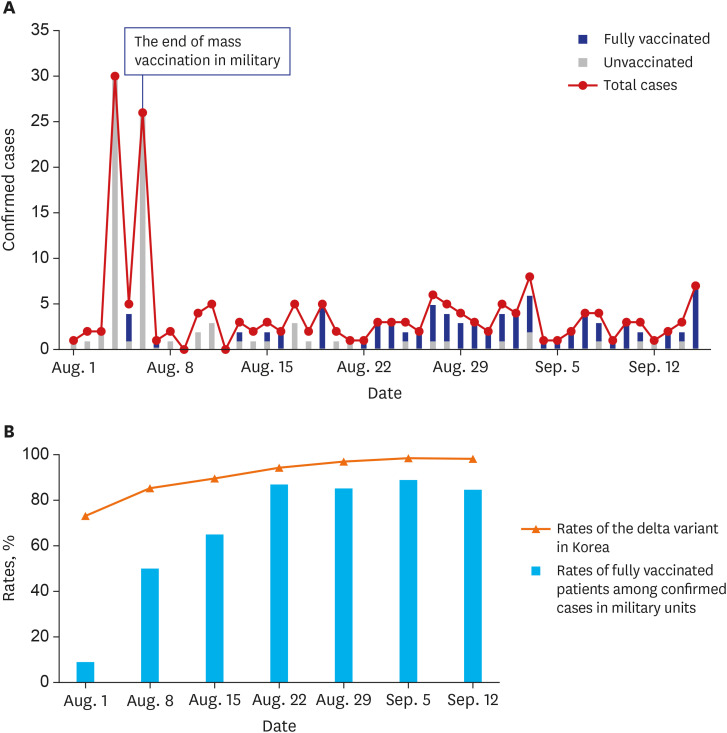
Fig. 3
(A) Trends of the number of confirmed COVID-19 cases by date in military units. (B) The rates of fully vaccinated patients (breakthrough infection)a among weekly confirmed COVID-19 cases in the units.
COVID-19 = coronavirus disease 2019.
aFully vaccinated status was defined as 2 weeks after completion of two doses of the vaccine (or one dose for Ad.26.COV2.S vaccine).
![]()
Comparison of the incidence rates of COVID-19 in the military and in Korean civilians
The incidence rates per one million person-days remained significantly lower in the military than in Korean civilians, averaging 15.12% of the incidence rates of Korean civilians during the observation period (Fig. 4). The percentage of fully vaccinated personnel in the military reached more than 85%, while nationally it gradually increased from 14.05% to 41.36%. Since most of the vaccinated civilians were older than 50, there was a large gap between the COVID-19 incidence rates of the military and Korean civilians aged 20-49 (Supplementary Fig. 1).
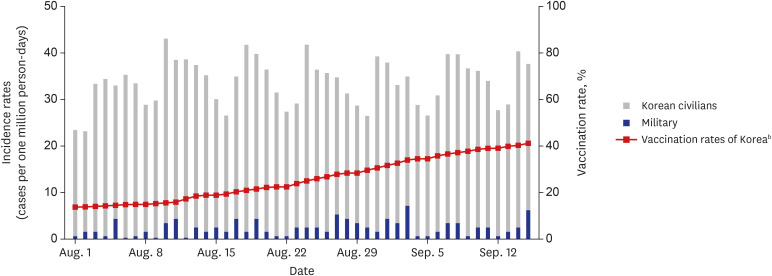
Fig. 4
The comparison of incidence rates of COVID-19 in military units and in Korean civilians.a
COVID-19 = coronavirus disease 2019.
aIn order to identify the effect of mass COVID-19 vaccination, the two cluster infection cases in military units were excluded. Military confirmed cases were excluded from the data of Korea.
bRate of fully vaccinated people in Korea; fully vaccinated status was defined as 2 weeks after completion of two doses of the vaccine (or one dose for Ad.26.COV2.S vaccine).
![]()
Clinical characteristics of index cases for each confirmed case occurrence in units
The characteristics of the 22 index cases, excluding cases that could not be traced, are described in Supplementary Table 2. The vaccinated index cases tended to have fewer symptomatic infections (vaccinated vs. unvaccinated, 40.00% vs. 71.43%; P = 0.361) and higher mean cycle threshold values (E gene, 23.41 vs. 16.37; P = 0.056; RdRp gene, 23.79 vs. 17.63; P = 0.105), but these differences were not statistically significant. Of the 14 cases tested for variants, 12 cases (85.71%) were identified as being the delta variant, and although the ratio of the delta variant in the vaccinated group was higher, it was not statistically significant (vaccinated = 90%, unvaccinated = 75%; P = 0.505).
DISCUSSION
Although the delta variant became dominant during the study period, the current results revealed that the number of confirmed COVID-19 cases in military units remained low following mass vaccination. The incidence rate of COVID-19 infection nationally (vaccination rate of 14.05% in early August) was higher than that of the military, and there was also a large difference between the incidence rates of the military and Korean civilians of similar age groups (aged 20–49). Additionally, results showed that higher vaccination rates were related to a lower number of confirmed COVID-19 cases among the units. By comparing the group of insufficiently vaccinated units to units that were vaccinated at a rate of 70% or higher, the results demonstrated that the vaccine was effective in preventing local transmission events and hospitalization. Although the risk of community exposure may differ between officers with free commuting privileges and soldiers, the likelihood of COVID-19 infection did not differ between the two groups in this study.
Unfortunately, there were cluster infection events in the two training camps that housed unvaccinated trainees under similar living conditions. In the training camps, the routine qPCR tests performed on individuals the day after they joined the training camps were all negative, but a few days later, the index patient developed symptoms and was confirmed to have COVID-19. Additional cases occurred one by one in the isolated cohort after this first infection. After the two cluster infections occurred and because trainees were excluded from the military’s mass vaccination program, it was strongly recommended that new recruits be vaccinated at community vaccination centers before joining the camps. Since September 27, new recruits have been vaccinated, and except for the occasional newly confirmed cases, cluster infection in the military has not occurred. While trainees were vaccinated before recruitment, non-vaccinated military personnel were strongly recommended to become vaccinated by restricting their daily activities through the “COVID-19 pass,” which started in December 2021 as recommended by the Ministry of Health and Welfare.23 Due to this strong recommendation to become vaccinated, each military unit achieved a vaccination rate of more than 85% from then on, including the remaining three units with completed vaccination rates of less than 70% (data not shown).
As shown in Table 1, the ratio of the unvaccinated individuals among confirmed COVID-19 patients in units that achieved herd immunity was significantly lower than that of non-herd immunity units. This suggests that unvaccinated personnel may have been protected due to the indirect effect of those around them having received the vaccine, also known as “herd immunity.”2425
In the first week of August, the proportion of fully vaccinated individuals among confirmed cases was low because the two cluster infection cases occurred in unvaccinated personnel, but the proportion increased over time, which may have been related to the increase in the ratio of the delta variant in Korea (Fig. 3). The rate of COVID-19 infection with the delta variant increased rapidly in Korea and had already reached 100% by mid-September. Similarly, 85.71% of the military COVID-19 patients were identified as having the delta variant during the observation period (data not shown), which implies that breakthrough infection via the delta variant made it difficult to completely prevent COVID-19 in the military,2627 despite the vaccination rate being maintained at 85% or more. However, mass vaccination may have prevented the outbreak of cluster infection.
If sufficient vaccination does indeed prevent cluster infection and reduce the severity of COVID-1928 infection, the level of NPI could be lowered further. Excessive NPI strategies such as social distancing and lockdowns of activities, which are currently being applied, not only increase psychological stress due to the leave regulation of military personnel, but also increase social costs.2930 As more than 70% of the Korean population has been fully vaccinated as of October 24, the KDCA announced that they would be lowering the level of NPI in November 2021.31 The results of this study not only provide evidence for lowering the level of NPI, but also support the justification of mass vaccination in groups similar to military units such as schools and nursing homes. Further research is needed to determine the extent to which NPI may be safe to cost-effectively prevent death by COVID-19.
This study had several limitations. First, because of the retrospective nature of the study, it was difficult to track each confirmed COVID-19 case and determine whether the confirmed patients actually progressed to severe/critical COVID-19, as previously defined.32 Hospitalized cases may have been overestimated because there were cases of hospitalized patients with subjectively severe symptoms or moderate COVID-19 rather than severe/critical COVID-19. This lack of clarity made it difficult to confirm the effect of vaccination on the prevention of severe disease. Second, mass vaccination cannot be said to have been the only contributing factor to the small number of confirmed COVID-19 cases in the units. As members of the Korean military were able to access qPCR testing and subsequently, to isolate faster than civilians, strict NPI in the military might have contributed to reducing local transmission. In addition, most confirmed cases in the military occurred due to community infection, and COVID-19 cases in Korea sharply increased in July 2021 with the rise in the ratio of the delta variant. Because of these changes, the trend of COVID-19 occurrence in the military before and after mass vaccination could not be compared. Lastly, as it was not possible to review the types of vaccines used in each unit, the effectiveness of each type of vaccine could not be compared in the study. Of military personnel aged 30 or older, 94.33% were administered ChAdOx1 nCoV-19-BNT162b2 heterologous vaccines, and all those under 30 years of age were vaccinated with BNT162b2 (Fig. 1B). As the effect of heterologous vaccination was thought to be similar,33 the vaccine effectiveness among military personnel could be expected to be similar.
In conclusion, more than 85% of Korean military personnel were vaccinated after mass vaccination, and the incidence rate of COVID-19 was lower than that among the civilian population in Korea. Additionally, new cluster infections did not occur in the vaccinated units, meaning herd immunity has been achieved. Further research is needed to determine how much the level of NPI can be lowered in the future.
 XML Download
XML Download