

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Stable angina is a clinical manifestation of transient myocardial ischemia that is usually caused by obstructive coronary artery disease (CAD). Myocardial ischemia plays a central role in the pathophysiology of angina pectoris and serves as a key target for the development of antianginal therapy. Various therapeutic modalities, including medications, percutaneous coronary intervention (PCI), and coronary artery bypass graft surgery (CABG) are available for the management of stable angina.1)2) However, the choice for the optimal therapy in stable angina remains difficult, requiring multifaceted approaches with the integration of evidence and individual preferences.
PCI has been developed to treat obstructive CAD and has become a mainstream therapy for patients with stable angina. The major goals of PCI are to relieve angina symptoms, prevent future myocardial infarction (MI), and improve survival. Numerous studies have compared the effects of PCI to those of medical therapy on major adverse cardiac events in a variety of clinical situations. PCI certainly improves symptoms and quality of life in patients with severe angina; however, it does not prevent MI or death in those with stable angina.3) Although the aim of PCI is to eliminate ischemia-producing lesions, a significant proportion of patients undergoing PCI have residual myocardial ischemia due to incomplete revascularization. There has been an increasing interest in complete revascularization (CR). Some studies have shown better outcomes with CR compared to incomplete revascularization, emphasizing the importance of a functionally CR strategy, the so-called “functional angioplasty”.4)5)6)7) To date, however, there is no agreed definition of functional angioplasty, and there is still uncertainty surrounding whether this approach prevents future coronary events. This article reviews the literature regarding myocardial ischemia, the history of PCI guidance, possible explanations, and provides some insights into the appropriate PCI strategy.
DEFINITIONS
Myocardial ischemia is traditionally defined as an imbalance between myocardial oxygen demand and supply to maintain normal cardiac function.8) It may be simply defined as electromechanical dysfunction of the heart caused by insufficient blood supply. Acute ischemia results in a typical sequence of events, beginning with metabolic disturbances and followed by wall motion abnormalities, electrocardiographic changes, and chest pain.9) A number of medical conditions, including obstructive CAD, microvascular disease, anemia, aortic valve disease, and many more can induce myocardial ischemia, leading to myocardial dysfunction with a disruption of the electrical and contractile integrity.
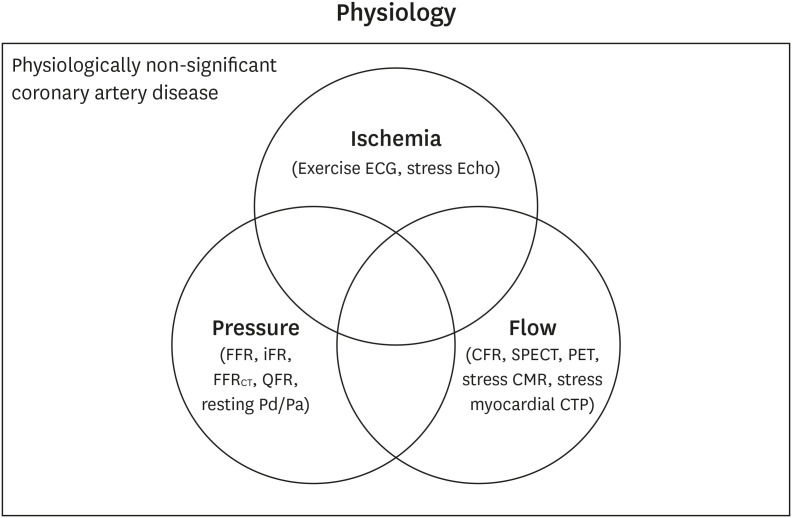
Various diagnostic tools have been developed to estimate the presence, extent, and severity of myocardial ischemia in patients with suspected angina (Supplementary Table 1).10) The detection of inducible myocardial ischemia relies on physiologic testing during exertional or pharmacological stress (Figure 1). The electrical and mechanical effects of an oxygen demand/supply mismatch are key indicators of ischemia for the affected myocardium, and transient reversible abnormalities on electrocardiography or regional wall motion during stress are direct evidence of inducible myocardial ischemia.11) In contrast, anatomic stenosis, coronary flow, and coronary pressure are indirect parameters for myocardial ischemia, and the surrogates of inducible myocardial ischemia. Nevertheless, these indexes have been used to detect and quantify inducible myocardial ischemia in daily clinical practice because a fully satisfying index does not yet exist.10)12)
Figure 1
Physiologic indices to define the presence of myocardial ischemia. Various diagnostic methods are used for the physiological assessment of CAD. The area in circles represents physiologically significant CAD, and the complement of the circled area physiologically non-significant CAD. Electrocardiographic and regional wall motion abnormalities during stress are a direct evidence of inducible myocardial ischemia, whereas changes in coronary flow or coronary perfusion pressure during stress are surrogates for inducible myocardial ischemia.
CAD = coronary artery disease; CFR = coronary flow reserve; CMR = cardiovascular magnetic resonance imaging; CTP = computed tomography perfusion; ECG = electrocardiography; Echo = echocardiography; FFR = fractional flow reserve; FFRCT = fractional flow reserve derived from coronary computed tomography angiography; iFR = instantaneous wave-free ratio; Pa = aortic pressure; Pd = distal coronary artery pressure; PET = positron emission tomography; SPECT = single-photon emission computed tomography; QFR = quantitative flow ratio.
PCI is used to treat stenotic lesions responsible for myocardial ischemia, and CR is considered a desirable goal of PCI. Although there are no accepted criteria for the completeness of revascularization,13) it might be ideally defined as the successful treatment of all ischemia-producing lesions without residual inducible myocardial ischemia. Therefore, it seems to be reasonable to define functional angioplasty as the absence of post-PCI inducible myocardial ischemia assessed by the reference standards for myocardial ischemia (Table 1).
Table 1
Proposed definitions

REFERENCE STANDARDS FOR MYOCARDIAL ISCHEMIA
Coronary angiography has been regarded as the gold standard for the diagnosis of CAD. Significant CAD was arbitrarily defined as diameter stenosis of at least 50% by early pioneers of CABG,14)15)16) and the cutoff values of 50% or 70% for diameter stenosis were subsequently adopted by most clinical studies.16)17)18) Interestingly, the results of early randomized trials showed the clinical benefit of CABG over medical therapy for patients with ≥50% stenosis of the left main coronary artery16) or ≥50%17) (or 70%18)) stenosis of other major coronary arteries. Furthermore, physiologic studies revealed a 50% stenosis of epicardial coronary arteries to be the ischemic threshold for the impedance of an increase in coronary flow in response to an augmented myocardial demand,19)20) supporting stenosis of at least 50% in an epicardial coronary artery as an indicator of significant CAD.
Numerous studies used a cutoff of 50% luminal diameter stenosis as the reference standard for myocardial ischemia to investigate the validity of noninvasive diagnostic tests with a wide range of sensitivity and specificity (Table 2, Supplementary Table 2). In these studies, the performance of noninvasive diagnostic tests was estimated on their ability to identify significant CAD with ≥50% stenosis. However, a 50% diameter stenosis was already recognized to be insufficient to decrease blood flow in early experimental studies.19)21)22) Ischemia remains undetectable under resting conditions in stable patients with severely stenosed CAD, and the induction of ischemia requires maximal cardiac workload.20) Gould et al.19) examined coronary flow in canine coronary stenotic arteries at rest and in hyperemic conditions and provided an elegant method of determining the presence of significant CAD, which is the basis for current pharmacologic stress tests, including fractional flow reserve (FFR), myocardial perfusion single-photon emission computed tomography (SPECT), and cardiac positron emission tomography (PET).
Table 2
Diagnostic performance of noninvasive tests according to reference standards
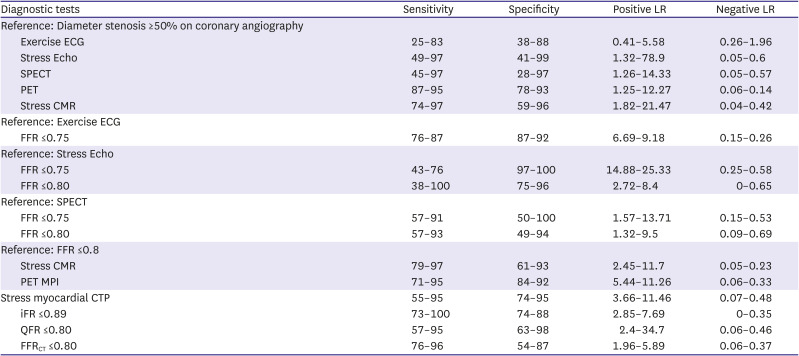
CMR = cardiovascular magnetic resonance imaging; CTP = computed tomography perfusion; ECG = electrocardiography; Echo = echocardiography; FFR = fractional flow reserve; FFRCT = fractional flow reserve derived from coronary computed tomography angiography; iFR = instantaneous wave-free ratio; LR = likelihood ratio; PET MPI = positron emission tomography myocardial perfusion imaging; QFR = quantitative flow ratio; SPECT = single-photon emission computed tomography.
FFR has been introduced to assess the hemodynamic significance of coronary artery stenosis and to overcome the limitations of the anatomical approach as a method of CAD diagnosis. It is well validated against various noninvasive stress tests and recommended to guide the treatment strategy in stable CAD.2)23) However, the threshold of inducible myocardial ischemia depends on both maximal stress flow and the coronary flow reserve,24) with some discrepancy between FFR and noninvasive stress tests (Table 2, Supplementary Table 3). There is only a moderate correlation between FFR and the coronary flow reserve, showing discordance in approximately 30–40% of coronary stenotic lesions.25) Nevertheless, FFR has been used as the reference standard of functionally significant CAD upon which new diagnostic tests are evaluated. For example, the cutoff values of the myocardial flow reserve by PET were derived against FFR, showing a diagnostic accuracy of about 80% in detecting significant CAD.26)27) Interestingly, a similar agreement between the two methods was also observed with PET as the standard reference.28) However, these kinds of studies raise a concern about the validation cycle because FFR is a surrogate marker of ischemia (Figure 2). The performance of a diagnostic test depends on its reference standard, leading to differences in the rate of diagnostic accuracy. Autoregulation maintains stable coronary flow across a wide range of perfusion pressures, and an FFR value of ≤0.8 may not necessarily induce electromechanical dysfunction of the heart.29)30)31) In this regard, the hallmarks of inducible myocardial ischemia such as electrocardiographic changes and regional wall motion abnormalities seem to be more reliable and clinically relevant as the reference standard to define ischemia-producing lesions.
Figure 2
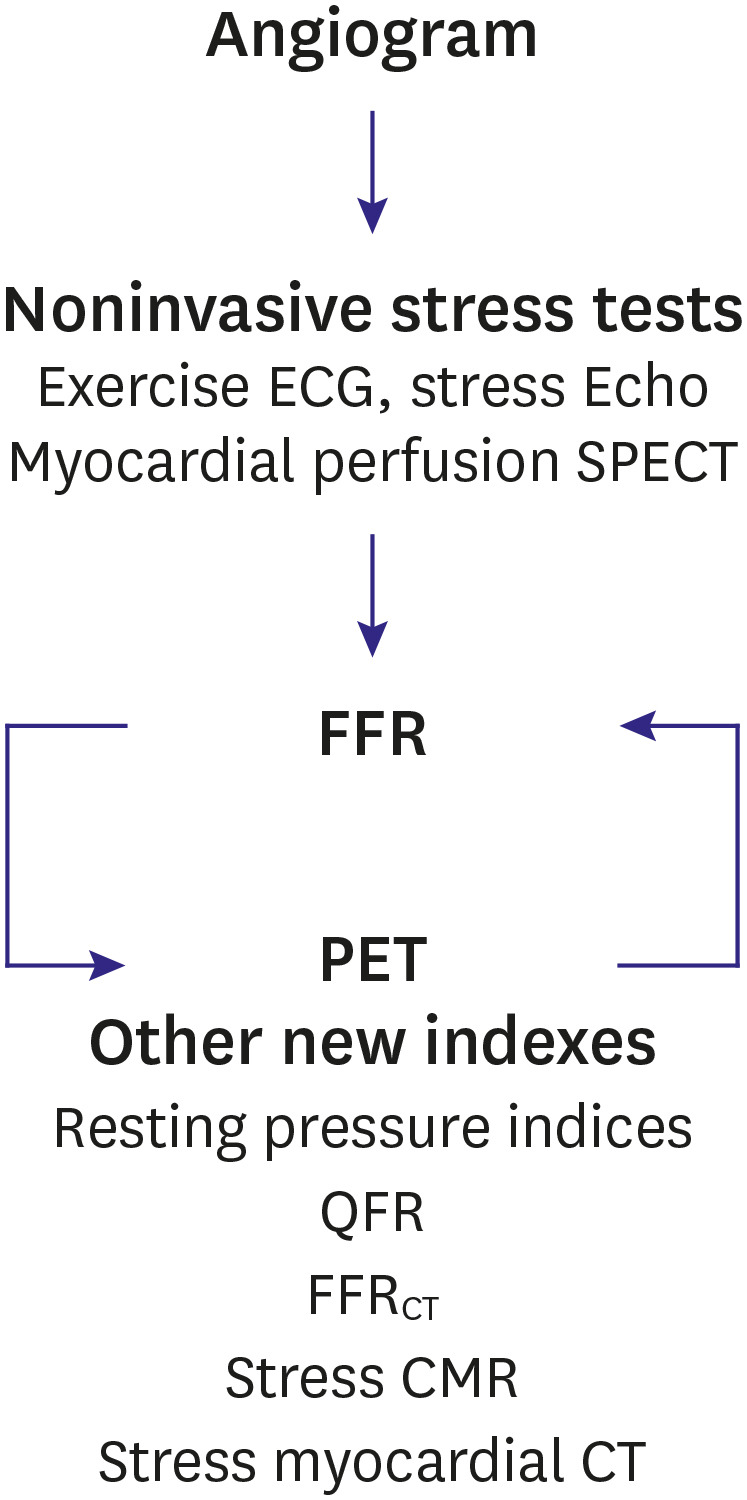
Timeline of the reference standards for the assessment of myocardial ischemia. The gold standard for the diagnosis of myocardial ischemia has been changed over the past several decades. Although FFR is a surrogate for inducible myocardial ischemia, it is nowadays used as a reference standard to evaluate the diagnostic performance of new ischemic indices.
CMR = cardiovascular magnetic resonance imaging; CTP = computed tomography perfusion; ECG = electrocardiography; Echo = echocardiography; FFR = fractional flow reserve; FFRCT = fractional flow reserve derived from coronary computed tomography angiography; PET = positron emission tomography; SPECT = single-photon emission computed tomography; QFR = quantitative flow ratio.
GUIDANCE AND ITS EFFECT ON OUTCOME AFTER PERCUTANEOUS CORONARY INTERVENTION
The guidance of appropriate PCI in stable angina remains a challenge despite a considerable effort to detect clinically significant CAD. Early studies were based on clinical symptoms and the severity of angiographic stenosis. Anatomically, CAD with diameter stenosis ≥50% was initially constructed to be eligible for PCI,32)33) which was derived from the CABG trials.16)17) In subsequent studies, left main coronary artery stenosis ≥50% was generally accepted to be hemodynamically significant. However, more strict criteria of 50–70% stenosis with or without additional evidence of ischemia were adopted to define significant CAD in other major coronary arteries.34) On the other hand, the limitation of anatomic stenosis has long been recognized with the discordance between stenosis, physiology, and symptoms. Thus, the need for improved tools to guide PCI has been raised.
Angiographic criteria for PCI have evolved from anatomic stenosis to anatomic stenosis with physiologic evidence of flow limitation. Various approaches have been developed to assist with the diagnosis of significant CAD and to guide the PCI strategy (Table 3, Supplementary Table 4). Numerous studies comparing PCI with medical therapy have reported similar rates of all-cause mortality and MI, irrespective of the criteria of myocardial ischemia. In other words, the types of PCI guidance did not affect subsequent hard clinical events, suggesting that PCI outcomes may not depend on the methods to evaluate the lesion severity. Furthermore, revascularization trials comparing different types of drug-eluting stents revealed that hard outcomes were similar among PCI devices regardless of the study protocol used to define ischemia.35)
Table 3
Trials comparing treatment strategies in stable CAD and their guidance
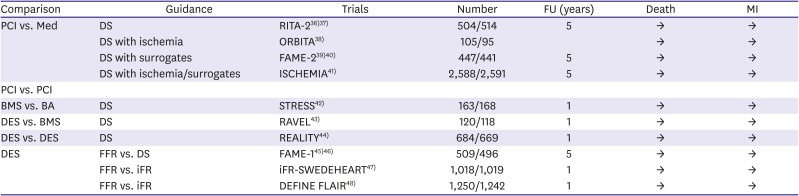
| Comparison | Guidance | Trials | Number | FU (years) | Death | MI |
|---|---|---|---|---|---|---|
| PCI vs. Med | DS | RITA-236)37) | 504/514 | 5 | → | → |
| DS with ischemia | ORBITA38) | 105/95 | → | → | ||
| DS with surrogates | FAME-239)40) | 447/441 | 5 | → | → | |
| DS with ischemia/surrogates | ISCHEMIA41) | 2,588/2,591 | 5 | → | → | |
| PCI vs. PCI | ||||||
| BMS vs. BA | DS | STRESS42) | 163/168 | 1 | → | → |
| DES vs. BMS | DS | RAVEL43) | 120/118 | 1 | → | → |
| DES vs. DES | DS | REALITY44) | 684/669 | 1 | → | → |
| DES | FFR vs. DS | FAME-145)46) | 509/496 | 5 | → | → |
| FFR vs. iFR | iFR-SWEDEHEART47) | 1,018/1,019 | 1 | → | → | |
| FFR vs. iFR | DEFINE FLAIR48) | 1,250/1,242 | 1 | → | → |
→ (arrow) indicates no statistical difference between the treatment strategies.
BA = balloon angioplasty; BMS = bare-metal stent; CAD = coronary artery disease; DES = drug-eluting stent; DS = diameter stenosis; FFR = fractional flow reserve; FU = follow-up; iFR = instantaneous wave-free ratio; Med = medical treatment; MI = myocardial infarction; PCI = percutaneous coronary intervention.
Nowadays, FFR is increasingly used to detect significant CAD and justify PCI in the cardiac catheterization laboratory. FFR was validated by outcome trials, showing that lesions with FFR values of ≤0.80 benefit from PCI.39)45) However, the advantage was primarily driven by reductions in soft endpoints, including repeat revascularization. There were no differences in hard clinical outcomes between angiography-guided PCI and FFR-guided PCI. Furthermore, instantaneous wave-free ratio (iFR)-guided PCI versus FFR-guided PCI showed similar outcomes despite the limitation of resting pressure-derived indexes as surrogates of inducible ischemia.47)48) Although repeat revascularization is an important component in the evaluation of PCI guidance, trial outcomes should focus on hard endpoints such as death and MI. There is no evidence so far that one guidance is superior to another in reducing hard outcomes after PCI. Additional work will be necessary to find a better method to guide PCI for individual patients, thus allowing for an appropriate therapeutic choice in a particular situation.
PLAUSIBLE EXPLANATIONS FOR THE OBSERVED FINDINGS
PCI improves both prognosis and symptoms in patients with acute coronary syndrome. However, the role of PCI in those with stable angina has been controversial. PCI does not provide a greater survival benefit than medical therapy. There is no significant effect of PCI on the incidence of total MI.3) Whether PCI reduces the risk of spontaneous MI still remains unclear.39)41)49)50) Although the prognostic impact of procedural MI is weaker than that of spontaneous MI,51)52)53) infarct size is considered as the key determinant of prognosis in both situations.54) There is no doubt that a large procedural MI is significantly associated with subsequent mortality.55)56)57) Collaterals at the onset of MI mitigate the extent of myocardial damage with smaller MI.58)59)60) Patients with severe CAD are more likely to have good collaterals and experience less severe MI after acute thrombotic occlusion.61) Accordingly, the small reduction in spontaneous MI with PCI for severe stenotic lesions is likely to be offset by an increase in a large procedural MI with a similar prognostic impact, and the net effect of clinically significant MI might be neutral with no reduction in all-cause mortality from PCI.
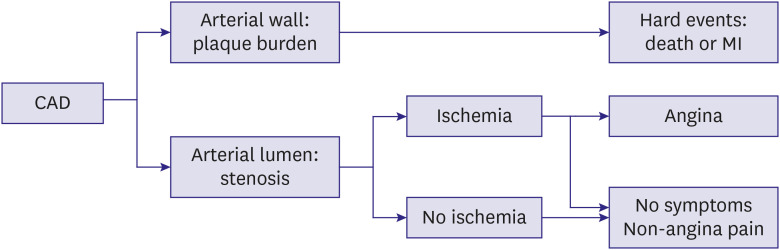
Although anti-ischemic medical therapy does relieve angina symptoms, it does not protect against death or MI.62)63)64) The Surgical Treatment for Ischemic Heart Failure (STICH) trial revealed that neither the presence nor the extent of ischemia was associated with mortality, challenging the concept that ischemia helps to guide decisions regarding revascularization.65) Moreover, in the International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHEMIA) trial, adverse clinical events were more associated with the extent of CAD based on diameter stenosis ≥50% than with the severity of myocardial ischemia.41) Atherosclerotic plaque burden rather than the stenosis severity has been shown to be the main predictor of cardiovascular events,66)67)68)69) supporting the idea that plaque vulnerability, but not inducible ischemia, drives acute coronary events. Obstructive CAD causes angina by stress-induced ischemia, whereas any atherosclerotic plaque could lead to acute coronary syndrome by abrupt thrombotic occlusion (Figure 3). In fact, patients do not die from inducible myocardial ischemia but from acute myocardial ischemia and its complications.38) Taking the available evidence into account, PCI seems to be a method of symptomatic therapy that does not alter the atherosclerotic biological process.70) These findings may help explain why the hard outcomes among patients receiving PCI and those among patients receiving medical therapy are similar regardless of the chosen PCI guidance.
Figure 3
Key determinants of clinical manifestations in CAD. CAD is manifested with either acute coronary syndrome or chronic coronary syndrome. Acute coronary events leading to death or MI are primarily determined by atherosclerotic plaque burden, whereas angina symptoms are determined by the degree of luminal stenosis (ischemia-causing stenosis).
CAD = coronary artery disease; MI = myocardial infarction.
FUTURE PERSPECTIVES
Physiology-guided PCI has been recommended under the assumption that the relief of ischemia-producing lesions improves clinical outcomes.1)2) However, PCI guided by surrogate markers or ischemia has failed to change the hard outcomes, questioning the validity of this approach.3) Indeed, hard outcomes depend on the atherosclerotic burden rather than the severity of ischemia.41)66)67)68)69) Physiologic markers may just reflect the underlying atherosclerotic burden, requiring a pathophysiology-based approach that is separated into anginal symptoms and future coronary events.
PCI plays a role in the symptomatic improvement of patients with stable angina. Although the Objective Randomized Blinded Investigation with optimal medical Therapy of Angioplasty in stable angina (ORBITA) trial questioned the antianginal effects of PCI,38) it has an additive antianginal effect through the correction of regional ischemia, particularly in patients with severe symptoms.71)72) However, it is unclear which method of physiologic testing confers greater benefits for angina control from PCI. The ORBITA trial revealed that the greater the ischemia on the stress echocardiogram, the greater the angina relief from PCI beyond placebo. However, there was no relationship between FFR values and placebo-controlled angina improvement.73) Ischemia, rather than surrogates, is the cause of angina symptoms, suggesting that ischemia might better predict symptomatic relief after PCI than surrogates. Anatomy and physiology assess fundamentally different features of CAD, which are actually complementary in PCI decision-making. Angiographic findings are critically important in guiding revascularization strategies because PCI is technically influenced by the anatomic complexity of the CAD. FFR is also helpful in searching for the symptom-causing lesion, especially in patients with intermediate and ambiguous lesions. Therefore, a comprehensive approach would be needed to identify patients most likely to benefit from PCI.
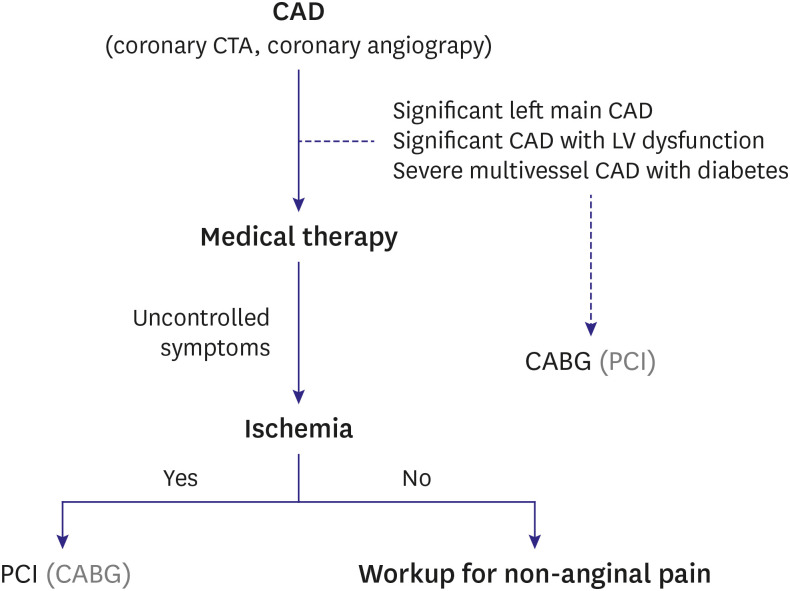
Finally, ischemic pain thresholds vary from person to person.74)75)76) Although some patients experience typical angina without any evidence of ischemia, others do not experience chest pain despite the presence of ischemia. It remains unknown whether PCI of non-ischemia-producing stenosis improves angina in patients with low pain thresholds. However, ischemia plays a pivotal role in angina, and PCI of ischemia-producing lesions might be a valid option in patients with severe angina. Ideally, PCI should be reserved for patients with objective evidence of inducible myocardial ischemia and suitable coronary anatomy who do not respond to optimal medical therapy (Figure 4).
Figure 4
Therapeutic approaches for CAD based on symptoms and ischemia. If patients have significant left main CAD, significant CAD with severe LV dysfunction, or severe multivessel CAD with diabetes, CABG is first recommended. In other cases, medical treatment should be considered the first-line therapeutic option with revascularization therapy (PCI or CABG) reserved for those with medically refractory angina and objective evidence of ischemia. Treatment in parentheses may be considered as an alternative approach in certain types of patients.
CABG = coronary artery bypass graft surgery; CAD = coronary artery disease; CTA = coronary computed tomography angiography; LV = left ventricular; PCI = percutaneous coronary intervention.
CONCLUSIONS
Although PCI does not provide prognostic benefits, it offers symptomatic relief in patients with stable angina. Optimal medical therapy remains essential in the management of stable angina, and symptom-driven functional PCI could be a reasonable approach for patients with unacceptable angina despite medical therapy. Further studies are needed to identify the best marker of the symptomatic benefits derived from PCI.
 XML Download
XML Download