

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Total hip arthroplasty (THA) is a successful treatment of patients with advanced hip disease, which has been nominated as the operation of the century.1 Nevertheless, it could be an invasive and painful procedure to the patient.2 It involves removal of bone and insertion of an artificial joint. The THA patients should be hospitalized and are anxious about postoperative pain, risk of transfusion, medical cost, duration of rehabilitation, risk of complications, and possibility of poor outcome. Moreover, fast-track protocol have been introduced in THA to reduce the duration of hospital stay worldwide.34 However, this protocol might increase patients’ anxiety and compromise their satisfaction.5
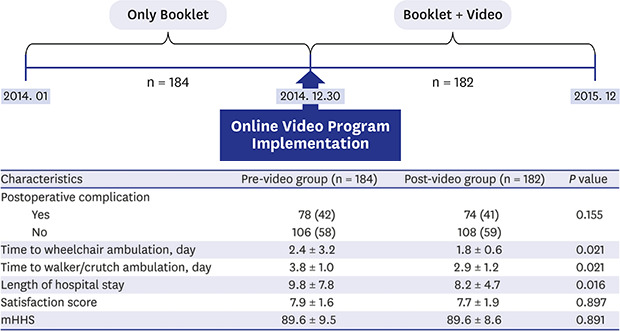
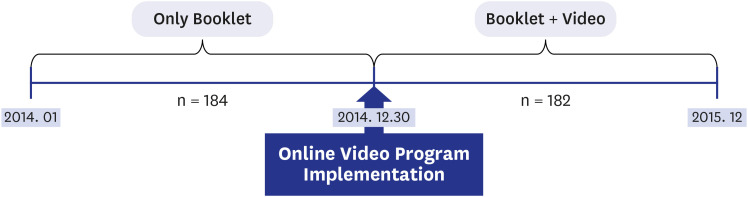
Recently, multimedia tools including online video have been introduced to provide patients with information they want to know. On December 30, 2014, our department implemented an online video program to provide detailed information about the whole process from admission to discharge and postoperative rehabilitation to THA patients.
In this before-after study on the effectiveness of the online video instruction, we compared 1) time to start ambulation, 2) the duration of hospitalization, 3) patients’ satisfaction and 4) clinical outcome at postoperative 6 weeks. Because primary diagnosis of the hip disease and surgeon’s factor might influence these outcomes, we restricted the subjects of this study to patients who were operated due to osteonecrosis of the femoral head (ONFH) by a single surgeon.
Go to : 
METHODS
The present study was approved from the local hospital institutional review board review. From January 2014 to December 2015, 397 patients underwent primary THA due to ONFH by one surgeon at our department. Among them, 31 patients who underwent bilateral THA were excluded. This left 366 patients (366 THAs): 184 patients operated in 2014 (pre-video group) and 182 patients operated in 2015 (post-video group) (Fig. 1).
Once THA was scheduled, the surgeon and physician’s assistant explained the type of anesthesia, surgical procedure, implant to be used, complications of THA, postoperative rehabilitation, duration of hospital stay, expected cost, and time of returning to work and recreational activity, and expected longevity of the prosthesis. While a booklet, which included above information, was given to patients in the pre-video group, a 12-minutes online video (https://hichart.tv/fCCL) was reinforced as well as the booklet in the post-video group. The video could be assessed via various tools: digital monitor of smart bed system in our hospital,6 smart phone or personal computer accessible to internet.
Just before skin incision, 1 gram of tranexamic acid was injected intravenously to reduce bleeding. All THAs were done with a single prosthetic design (Mirabo cup and M stem; Corentec, Cheonan, Korea) and delta-on-delta ceramic articulation (BIOLOX delta; CeramTec, Plochingen, Germany) using Kocher-Langenbeck approach.7 We did not put suction drainage. Patients were encouraged to ambulate on wheelchair 1 day after the operation and to walk with crutches on the postoperative day 2. Patients were advised to discharge when they could walk alone and there was no problem in the wound. The patient’s satisfaction was measured on the postoperative day 5 and the functional outcome was evaluated at postoperative 6-week follow-up.
We retrospectively reviewed the medical records of the 366 patients: 184 patients in the pre-video group and 182 patients in the post-video group, to compare 1) the time to start wheel chair ambulation; 2) the time to start ambulation using walker or crutch; 3) the length of hospital stay; 4) postoperative satisfaction using visual analogue scale from 0 to 10 points; and 5) functional outcome using modified Harris Hip Score (mHHS) between the two groups.
Student's t-test was used for the comparison of numerical variables and χ2 test for the comparison of categorical variables. A P value less than 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
As a retrospective study, this study holds out no additional risk to participants and it is approved by Seoul National University Bundang Hospital Institutional Review Board (IRB No. B-2103/672-101) with the waiver of informed consents.
Go to :
RESULTS
There were no significant differences in patient demographics, stage of ONFH, American Society of Anesthesiologists (ASA) score, Charlson comorbidity index, type of anesthesia, the amount of bleeding, the volume of transfusion.
There were no significant differences in the incidences of systemic complications (pneumonia, deep vein thrombosis/pulmonary embolism, myocardial infarction, and cerebral infarction) and surgical complications (dislocation, infection, periprosthetic fracture, sciatic nerve injury) between the two groups (Table 1).
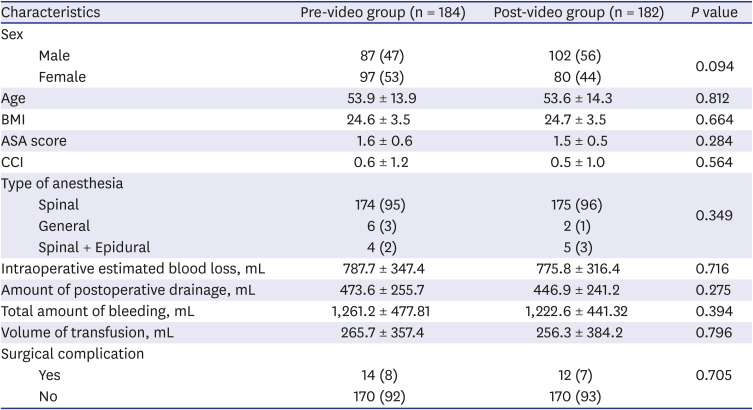
Table 1
Comparison of demographics between pre-video group and post-video group
Age, BMI, ASA score, CCI, amount of bleeding, volume of transfusion are shown in mean ± standard deviation. Sex, type of anesthesia, surgery-related problem are expressed as frequency and percentage.
ASA = American Society of Anesthesiologists, CCI = Charlson comorbidity index, BMI = body mass index.
![]()
In the post-video group, the time to start wheelchair ambulation was faster (1.8 ± 0.6 vs. 2.4 ± 3.2 days, P = 0.021), the time to start walker/crutch ambulation was faster (2.9 ± 1.2 vs. 3.8 ± 1.0 days, P = 0.016), and the duration of hospital stay was shorter (8.2 ± 4.7 vs. 9.9 ±7.8 days, P = 0.001) compared to the pre-video group.
The postoperative satisfaction score (7.8 ± 1.6 vs. 7.7 ± 1.9) and mHHS at postoperative 6 weeks (89.6 ± 9.5 vs. 89.6 ± 8.6) were similar between the two groups (Table 2).
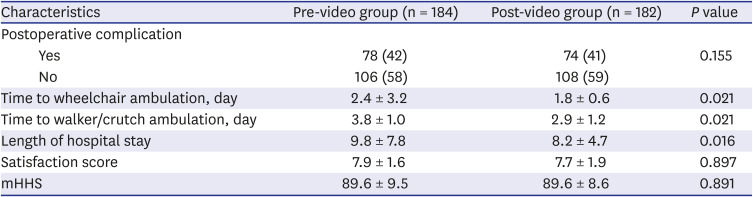
Table 2
Comparison of postoperative data between pre-video group and post-video group
Time to wheelchair ambulation, time to walker/crutch ambulation, length of hospital stay satisfaction score, mHHS are shown in mean ± standard deviation. Postoperative complication is expressed as frequency and percentage.
mHHS = modified Harris Hip Score.
![]()
Go to :
DISCUSSION
Our study showed that preoperative online video instruction expedited ambulation and reduced the duration of hospital stay without compromising patient’s satisfaction and functional outcome after THA.
Patients undergoing surgery are anxious about what will happen during the hospitalization period, the potential complications and outcomes of the surgery.89 Preoperative anxiety had been known to negatively affect the clinical outcome and satisfaction following total knee arthroplasty (TKA).101112
In 2004, McGregor et al.13 reported that preoperative instruction of rehabilitation advice reinforced by a patient information booklet expedited functional recovery and patient’s satisfaction after THA. Moreover, the preoperative class and booklet reduced the hospital stay by 3 days, therapy input required, and consequently the medical cost. The increase of elderly patients undergoing hip arthroplasty furthermore underlines the importance of education throughout the admission and surgery.1415
To date, numerous articles have been published on the effect of preoperative education on alleviating postoperative complications. These approaches incorporated various teaching tools including: DVD/video,1617181920 online education/websites,212223 and booklets/pamphlets 16242526 were incorporated in the preoperative education. In a review of 13 randomized control trials involving a total of 1,017 subjects who underwent THA or TKA,27 educations through these sources appeared to increase knowledge of the surgical procedure reduce anxiety, reduce postoperative pain, decrease length of hospital stay, and reduce the time to return to preoperative functional levels.
Currently, patient instruction is more important than before because fast track procedure, bundled payment, and diagnosis-related group have become popular trends worldwide and THA patients should be discharged shortly after the operation. Patients do not have enough opportunity and time to contact with the medical staff for counseling.282930 Thus, efforts should be made to instruct patients prior to surgery to relieve their anxiety.3132
So far, leaflets and brochures have been used as supplementary materials to instruct patients.33 However, widespread use of smartphones enabled the online delivery of information and audiovisual sources became a teaching strategy for patient education.34
There are limitations in this study. First, it is a retrospective before-after review and there is a risk of unidentified confounders. Second, we included a patient cohort of single disease (ONFH) and our study was done in East Asia. Our results might be otherwise in other patient cohorts.
Preoperative instruction reinforced by an online video can expedite ambulation and reduce hospital stay after THA. We recommend the use of this educational strategy for patients undergoing total joint arthroplasty and other orthopedic surgical procedures.
Go to :
 XML Download
XML Download