

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Transplantation using organs from donors with bloodstream infection poses a risk of transmission. It has been shown that there is no need to turn down the kidneys from donors labeled increased risk for disease transmission; however, it is still cautious about using allografts from donors who have already been confirmed to be infected.1 Generally, the transmission is reported in less than 1% of deceased donor donations.2 Besides, several successful transplant cases have been reported from the donors even with virulent pathogens or severe infection.3456
Nevertheless, the fact that donor-derived infections are still associated with high morbidity and mortality makes decision-making difficult.789 And in the RESITRA study, which prospectively searched for bacterial infections, the transmission rate is relatively higher than that of other studies.9 This means that the transmission is affected by reporting; in other words, it may have been underrated.
There is a major limitation in studying transmission as a single-center study. Because donors with bloodstream infections account for only 5% of all donors and a center usually does not receive both organs, it is difficult to know the exact transmission rate.10 Therefore, we aimed to evaluate the transmission rate and transplant outcomes by conducting a multicenter retrospective study from 5 tertiary medical centers, which perform approximately 30% of deceased donor transplant in Korea.
Go to : 
METHODS
Study population
The Korean Network for Organ Sharing (KONOS) is a government-affiliated organization that handles deceased donor organ transplantation data in South Korea. Data were extracted from the database of Tissue and Blood Management Department under KONOS. This database was used to identify recipients who received transplants from donors with abnormal blood culture tests from January 2009 to November 2019. Based on their age, sex, transplant date, and aortic cross-clamp time, patients who underwent kidney and simultaneous pancreas-kidney transplant at Seoul National University Hospital, Severance Hospital, Samsung Medical Center, Seoul St. Mary’s Hospital, and Asan Medical Center were identified. In addition, patients who were not listed in the KONOS database and received transplants from infected donors at these 5 tertiary medical centers were identified additionally. Among them, patients with available microbiology reports were included in the analysis.
Data collection and definition
KONOS data was used only for the identification of the study population and for information about the use of antibiotics in donors. All other data were obtained from the medical record of each hospital.
We collected data, including donors’ age, sex, cause for death, length of intensive care unit stay, recipients’ age, sex, original disease, human leukocyte antigen (HLA) mismatch number, and cold ischemic time. Data on pathogens isolated in donor blood culture, the number of cultures, and susceptibility test results were collected.
After transplantation, the following outcomes were reviewed. Within one year after transplant, all infectious complications and associated pathogens and clinical course of infectious complications were recorded. During the same period, the occurrence of acute rejection and related anti-rejection treatment were reviewed. Graft function at one year, graft, and patient survival were collected.
If the criteria for proven or probable transmission were satisfied, it was confirmed as a transmission event. Proven transmission was defined when there was clear evidence of the same infection disease in the donor and at least one of the recipients. Probable transmission was defined when there was strong evidence suggesting but not proving a disease transmission.11 Further details can be found in the published paper.8 Before transplant, appropriate antimicrobial therapy was defined as when antimicrobial agents susceptible to bacteria or fungi growing in donor blood were used at least 24 hours before organ retrieval. After transplant, appropriate antimicrobial therapy was defined as when used at least 48 hours in recipients. Delayed graft function (DGF) is defined as the need for renal replacement therapy within the first week after transplantation.12
Statistical analysis
Normally distributed continuous variables were expressed as mean ± SD, and non-normally distributed ones were expressed as median and range. Logistic regression modeling was used to explore the factors affecting infectious complications. To compare graft and patient survival between the infected donor group and the non-infected donor group, we matched these two in a 1:3 fashion using the propensity score. Propensity scores were calculated using donor age, sex, recipient age, sex, HLA mismatch, presence of donor-specific antibody, and transplant type. Statistical analyses were performed using SPSS (version 23.0; SPPS Inc., Chicago, IL, USA). A value of P < 0.05 was considered statistically significant.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Seoul National University Hospital, Severance Hospital, Samsung Medical Center, Seoul St. Mary’s Hospital, and Asan Medical Center Institutional Review Board (2002-173-1107). Informed consent was waived for this study by these IRBs.
Go to :
RESULTS
Patients
During the assessed period, a total of 277 deceased donors with abnormal blood culture tests were identified in the KONOS database. Kidney and pancreas allografts from these donors were transplanted in 577 recipients. A total of 179 recipients were confirmed to receive transplants at 5 tertiary centers. Excluding patients with inadequate microbiologic results, 86 recipients who received transplants from 69 donors with positive microbiology results were included in the analysis.
Patient demographics are shown in Table 1. The mean ages of the donors were 43.1 ± 16.4 years, with 63.8% male. The mean length of intensive care unit stay of 69 donors was 12.0 ± 12.6 days, and 47.8% of donors received appropriate antimicrobial agents before retrieval operation. The mean duration of cold ischemia was 245.6 ± 99.9 minutes. 34.9% of recipients received induction therapy with thymoglobulin.
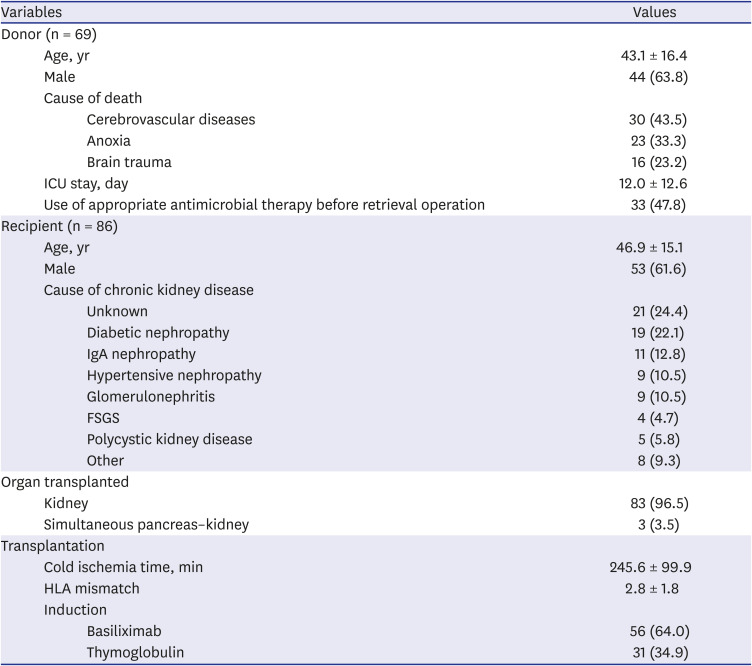
Table 1
Donor, recipient and transplant characteristics
Data are shown as mean ± SD or number (%).
ICU = intensive care unit, IgA = immunoglobulin A, FSGS = focal segmental glomerulosclerosis, HLA = human leukocyte antigen.
![]()
Microbiology
The microbiologic results are summarized in Table 2. All microorganisms were isolated from donors’ blood. Gram-positive bacteria and gram-negative bacteria accounted for 72.0% and 22.7%, respectively. Fungemia was confirmed in 4 donors. Six patients had polymicrobial infections (Candida parapsilosis and Staphylococcus epidermidis; Staphylococcus haemolyticus and Staphylococcus capitis; Enterococcus avium and Candida tropicalis; Enterococcus faecium and Klebsiella pneumoniae; Enterococcus faecium and Staphylococcus aureus; Staphylococcus haemolyticus and Staphylococcus cohnii). Coagulase-negative Staphylococcus was the most common organism isolated in donors’ blood. In 25 donors, two or more cultures were positive; in 25 donors, only one of the multiple blood culture results was positive, and information on the number of cultures was not available in the rest.
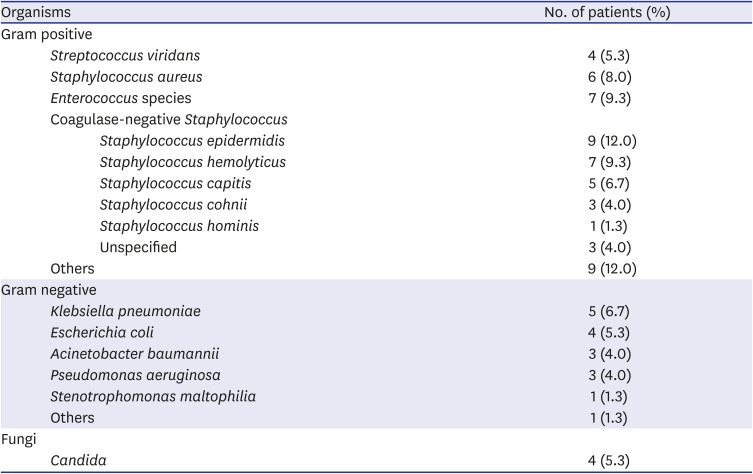
Table 2
List of organisms isolated from donors’ blood
![]()
Outcomes
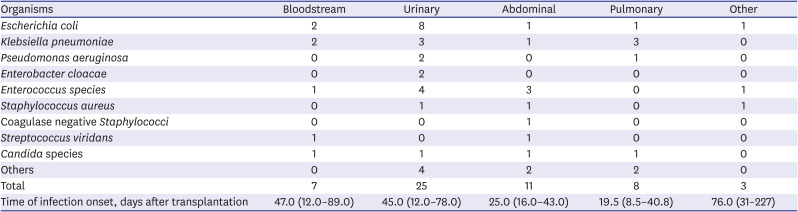
The organisms identified in the recipient within 1 year after transplant are summarized in Table 3. The most common infection site was the urinary tract, and the most frequently identified pathogen was Escherichia coli. The next most frequent site of infection was the abdominal cavity, followed by the pulmonary and bloodstream. Most infectious events occurred early after transplantation (Fig. 1).
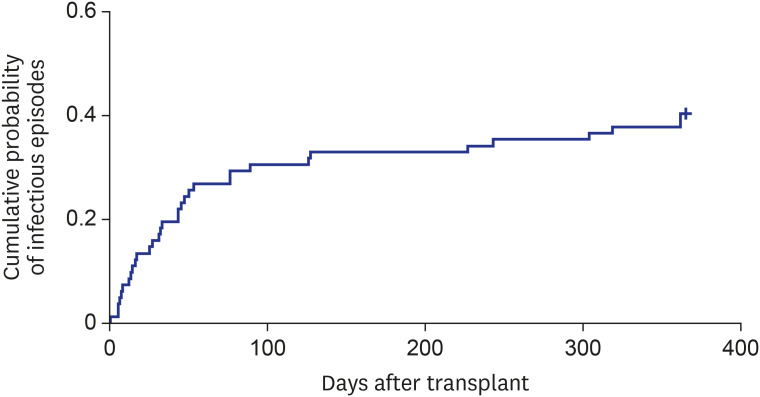 | Fig. 1Kaplan-Meier cumulative probability curve showing the incidence of infectious complications after transplantation.
|
Table 3
Pathogens associated with infectious complications in recipients within 1 year after transplant
![]()
One (1.2%) of the 83 recipients was suspected of bacterial transmission and the fungal transmission was confirmed in 1 (16.7%) of 6 recipients (Table 4). A 58-year-old male (recipient 1) received a kidney from the donor with carbapenem-resistant Acinetobacter baumannii bacteremia and subsequently developed urinary tract infection with the same organism early after transplantation. After 7 days of targeted antibiotic therapy, the infection resolved without clinical sequelae. A 60-year-old male (recipient 2) had received adequate antifungal therapy for seven days due to the candidemia of the donor. However, a month after transplant, persistent candidemia and infected endocarditis developed and required surgical treatment. The patient was followed up for 21 months, the renal function was stable (the last creatinine level was 1.54 mg/dL), and there were no additional infection episodes.
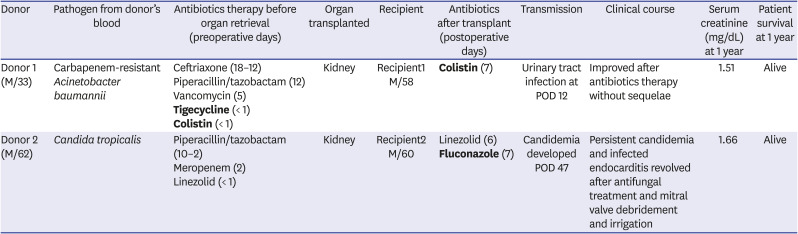
Table 4
Clinical course of the recipients with transmission events
![]()
After propensity matching, the baseline characteristic between the infected donor group and the noninfected donor group is shown in Table 5. One-year outcomes are summarized in Table 6.
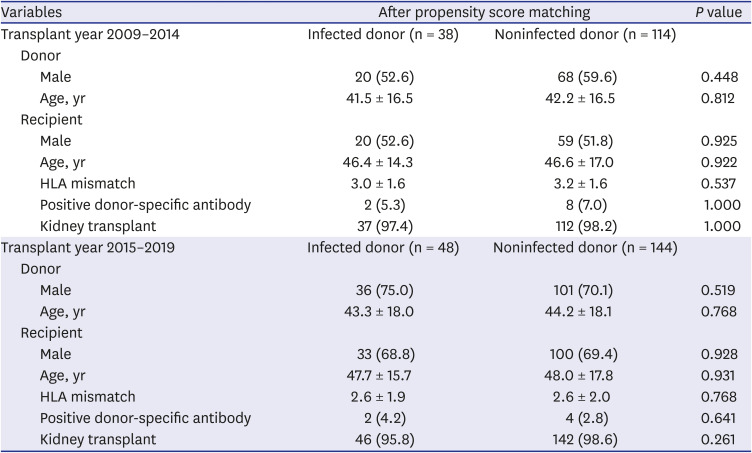
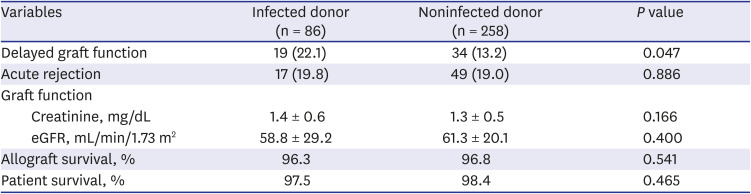
Table 5
Demographic, clinical and immunological data of the studied population
![]()
Table 6
One-year outcomes of recipients from infected donors and non-infected donors
![]()
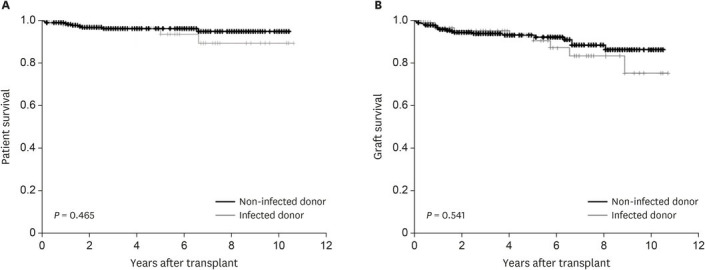
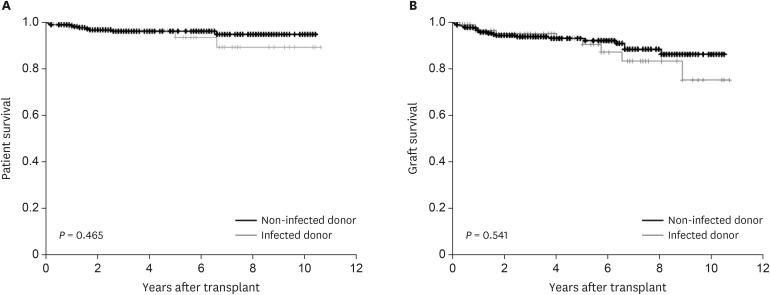
In recipients of organs from infected donors, 22.1% of patients developed DGF after transplant. The mean serum creatinine and evaluated glomerular filtration rate at one year were 1.4 ± 0.9 mg/dL and 58.1 ± 29.6 mL/min/1.73 m2, respectively. Except for the rates of DGF, there were no significant differences in outcomes, including graft survival and patient survival (Fig. 2), between recipients from infected and noninfected donors.
Go to :
DISCUSSION
The shortage of organs is a constant problem in transplantation, and there have been various efforts to increase the donor pool. Infection in donors is not a rare condition, and it is found in about 20% of donors.13 It was found that bacteremia was detected in about 5% of deceased donors,10 and Candida species were detected in preservation fluid in about 0.1% of cases.14 Even if there is an active or suspected infection in the donor, it is recommended to consider the use of allograft based upon the urgency of transplantation for the recipient, the availability of alternative organs, and recipient informed consent.15 However, transmission is still a concern because it is known that transmission is associated with a poor prognosis.78 The biggest obstacle to knowing the exact rate of transmission is that there are many cases where the donor and recipient are in different organizations, and communication between them is limited and not prompt.8 Thus, there may be cases where it is not clear whether it is a transmission or de novo infection.
Although some cases of bacterial transmission are reported, the outcomes of using donors with bacterial infection are mostly favorable. In a study using the United Network for Organ Sharing (UNOS) database, there was no difference in graft survival and patient survival except the occurrence of DGF between recipients who received kidney transplants from blood culture positive donors (n = 3,646) and propensity score-matched recipients from non-blood culture-positive donors.16 In addition, several single-center studies have demonstrated that bacterial transmission is infrequent.171819 Similar to previous studies using the UNOS database, some studies have shown that infectious complications, graft, and patients survival are not significantly different between infected and non-infected donors.1720 The transmission was mostly reported in case reports. Most of them were related to multidrug-resistant pathogens or were not receiving appropriate antimicrobial agents due to unexpected infection.21222324 However, even in the case of multidrug-resistant bacteria, it was emphasized that transmission did not occur if antimicrobial agents were properly used for seven days after the recognition of the donor infection.25 Our study showed the same results. If donors have bloodstream bacterial infection, our study showed that the transmission rate is very rare. Although the use of appropriate antimicrobial agents was in less than half (47.8% before transplant and 39.5% after transplant), no bacterial transmission was reported.
For fungal infections, there is a more lack of data. Although fungal transmission was quite rare, it seemed to be associated with worse results than bacterial transmission.26 In a multicenter study conducted in France, Candida species were detected at the kidney graft site in 0.1% of cases, and 75% of recipients were infected Candida species.14 Most of the recipients with transmitted infections had serious complications such as aneurysms or graft loss. For fungal infections other than Candida species, the incidence is not well known. Most infections are not detected in routine screening; therefore, there have been some cases with serious consequences due to insufficient treatment.242728 If multiple infections occur in recipients received from common donors, it is recommended to share this information immediately, treat patients appropriately, and observe them for an extended period of time. In our study, Candida species was confirmed in the donor's blood, not the graft site, and transmission occurred in 1 (16.7%) of the 6 cases. The recipient received proper antifungal treatment for seven days after transplant; however, the infection was not controlled even with an empirical antifungal agent. Therefore, the patient received surgical treatment due to infected endocarditis.
Our study has some limitations. The first limitation of this study is its retrospective design. The second is the small number of patients, which shows the limitation of the KONOS database. Currently, KONOS database only collects infection data up to the time of transplantation, so patients with confirmed infections after transplantation may have been excluded. Especially for fungal infections, it was difficult to draw definite conclusions because the number of patients was small. Third, there were some cases where central nervous system only grew in one of several donor blood cultures. Although it was not definite whether it was a true pathogen or not, it was considered true pathogens because it was accompanied by fever, and there was no other infection site. Another limitation is that the data on the culture of preservation fluid is not routinely collected in Korea. Previous studies showed that positive preservation fluid culture was associated with an increased risk of transmission.1429 In Korea since the cold ischemic time is short in most cases, it is thought that graft-site infection incidence may be slightly lower, but it has not been accurately evaluated.
In conclusion, using organs from donors with bacteremia seems to be a safe option with a low risk of transmission. However, whether to use organs from donors with fungemia should be cautiously determined.
Go to :
 XML Download
XML Download