

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Seasonal influenza poses a huge global burden, affecting children especially under 5 years old, and was responsible for 10 million lower respiratory tract infections (LRTIs), and 35,000 influenza-related pediatric deaths in 2018, worldwide.1 The best prevention strategy is universal vaccination, but its incomplete efficacy and influenza’s yearly variation is problematic.234 Therefore, timely diagnosis is crucial to both prevent the spread, as well as to properly manage these cases.567
Rapid antigen test (RAT), also referred to as rapid influenza diagnostic testing, was introduced in the 1990s as a form of point-of-care testing, characterized by its easy use, fast results (within 10–15 minutes), and low cost.8 Despite its widespread use, RAT can yield false-negative results due to its low sensitivity (64.6% [59.0–70.1%] for influenza A and 52.2% [45.0–59.3%] for influenza B).91011 Therefore, rapid polymerase chain reaction (PCR)-based assays have been developed, with a high sensitivity of 90–100%.12
The Infectious Diseases Society of America began recommending the use of rapid PCR-based assays instead of RATs in outpatient clinics and hospitalized patients in 2018.13 However, as of March 2021, the National Health Insurance Service of Korea does not cover PCR-based assays. Instead, RATs are still widely utilized in emergency departments (EDs) and outpatient clinics during influenza season.
This study aimed to investigate the effect of antiviral treatment timing on RAT-false-negative and RAT-positive influenza patients. Additionally, we sought to determine the risk factors of severe clinical outcomes associated with delayed treatment and evaluate the cost-benefit analysis by several scenarios of antiviral initiation in EDs in Korea.
METHODS
Study design and data collection
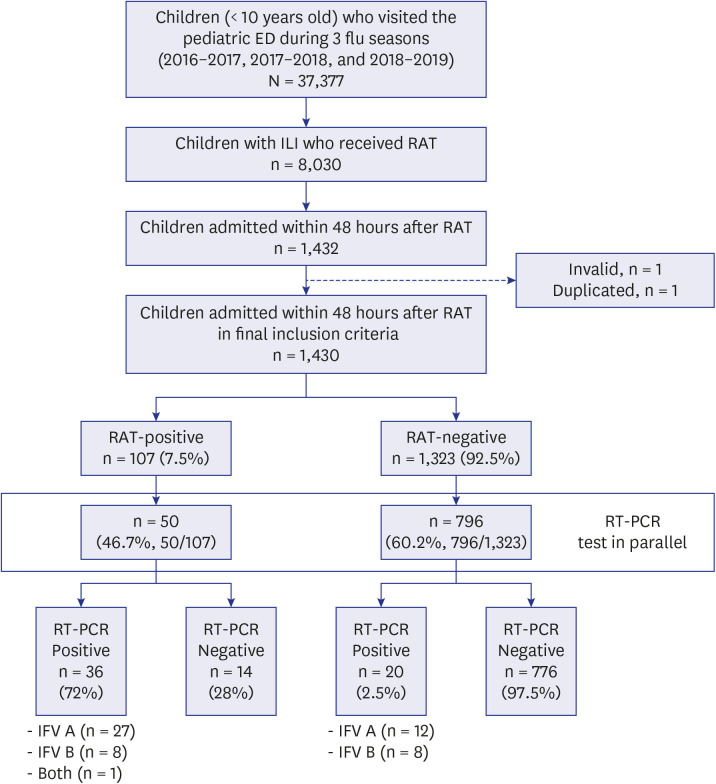
This retrospective observational study was conducted throughout three influenza seasons from 2016–2017 to 2018–2019 at Severance Children’s Hospital in Seoul, Korea. This is a tertiary referral hospital with > 23,000 annual pediatric visits to the ED. Patients included in this study were children under the age of 10 years who were suspected to have influenza-like illness (ILI), who were tested by influenza RAT at the pediatric ED, and were hospitalized within 48 hours. After hospitalization, multiplex respiratory viruses reverse transcription PCR assay was performed at the clinician’s discretion, regardless of the RAT result. Data were extracted from the chart-based electronic database and included age, sex, diagnosis, influenza immunization history, diagnostic methods, details of antiviral prescriptions, and clinical manifestations. A total of 37,377 children visited the ED during the three consecutive influenza seasons, and 8,030 underwent RAT (Fig. 1).
Definitions
ILI in this study was defined as fever (≥ 38°C), with or without respiratory symptoms, lacking an identifiable cause other than influenza. Laboratory-confirmed influenza illness was defined as positive RAT (lateral flow immunoassay, BD Directigen™ EZ Flu A+B; Becton Dickinson, Franklin Lakes, NJ, USA) or positive multiplex PCR (AdvanSure™ RV real-time reverse transcription-PCR; LG Life Sciences, Seoul, Korea). LRTI was defined as the need for oxygen supplementation due to hypoxia (SpO2 < 95%) or pneumonic infiltrations on chest radiograph (lobar consolidation, pleural effusion, acute respiratory distress syndrome, etc.). LRTI was further specified as severe if oxygen supplementation was required for ≥ 24 hours. Severe influenza infection was defined as cases of severe LRTI, or upper respiratory tract infection (URTI) upon ED presentation that progressed to LRTI during the hospitalization. The turnaround time to antiviral treatment (TAT) was defined as the time when the clinician ordered the RAT to when oral oseltamivir or intravenous peramivir was administered to the patient. LRTI, severe LRTI, progression from URTI to LRTI, severe influenza, pediatric intensive care unit (PICU) admission, mechanical ventilation, and 30-day mortality were used as clinical outcome parameters.
Comparison by scenario
To analyze the medical costs and TAT, the scenarios were divided as follows:
• Scenario 1 (RAT-based approach): RAT was performed on all ILI patients, and they were administered oseltamivir if the result was positive.
• Scenario 2 (Empiric treatment-based approach): Antivirals were administered to all ILI patients without testing.
• Scenario 3 (PCR-based approach): PCR-based assay was performed on all ILI patients, and they were administered oseltamivir if the result was positive.
• Scenario 4 (Hybrid approach): RAT was performed on all ILI patients, and they were administered oseltamivir if the result was positive. If RAT was negative, patients were then tested with PCR and treated accordingly.
The cost was calculated only for the diagnosis of influenza and the antiviral treatment.
Influenza epidemics in Korea and vaccination practices
Korea has a temperate climate, and influenza is usually prevalent from winter to late spring. The Korea Disease Control and Prevention Agency issues an annual influenza season advisory when the percentage of ILIs in participating sentinel institutions exceeds the baseline.14 The baseline rate is calculated by adding two standard deviations to the mean percentage of patient visits for ILIs outside influenza season weeks for the previous three seasons. The end of the influenza season is declared by the Korea Disease Control and Prevention Agency when the percentage of ILIs is below the epidemic baseline for three consecutive weeks. The 2016–2017 influenza season was designated from December 8, 2016, to June 2, 2017, the 2017–2018 and 2018–2019 seasons from December 1, 2017, to May 22, 2018, and November 16, 2018, to June 21, 2019, respectively.
National immunization program covers influenza vaccination from age of 6 months to 12 years, and those older than 13 years with risk factors such as chronic lung disease, hemodynamically significant heart disease, immunocompromised state, metabolic disease, long-term aspirin use, and predisposition to aspiration pneumonia. Complete vaccination requires that children under 9 years old who have never been vaccinated with influenza are vaccinated twice with at least 4 weeks interval, and annually thereafter. Inactivated intramuscular vaccines are available (trivalent or tetravalent).
Statistical analysis
Continuous variables were expressed as median (interquartile range) and were compared using the independent t-test. Categorical variables were expressed as frequencies (%) and were compared using the χ2 or Fisher’s exact tests. Cox proportional hazards regression analysis was performed to identify the independent factors associated with clinical outcomes which were adjusted for age, sex, and underlying disease. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and GraphPad Prism version 8.1.2 (GraphPad Software, La Jolla, CA, USA). The linear-by-linear association test was used for the year-trend analysis. Conditional logistic regression models were used to determine the odds ratio for the clinical outcomes. P values < 0.05 are considered significant.
Ethics statement
This study was approved by Institutional Review Board of the Yonsei University College of Medicine (4-2019-0785), and the need for informed consent was waived because of the retrospective nature. This study was conducted in compliance with the Health Insurance Portability & Accountability Act and the Declaration of Helsinki.
RESULTS
Patient characteristics
A total of 1,430 hospitalized children (17.8% underwent RAT) were included in this study. The male-to-female ratio was 1.3:1, and 61.5% were under 2 years of age. About 42.3% of children had been vaccinated against seasonal influenza prior to the ED visit, with the rest (57.7%) having received incomplete or no vaccinations at all. About 38.3% of patients had at least one underlying disease, neurologic disease being the most common (42.6%), followed by prematurity (21.4%), cardiovascular disease (15.2%), and chronic lung disease (13.7%) (Table 1).
Table 1
Clinical characteristics of RAT-positive and RAT-negative groups
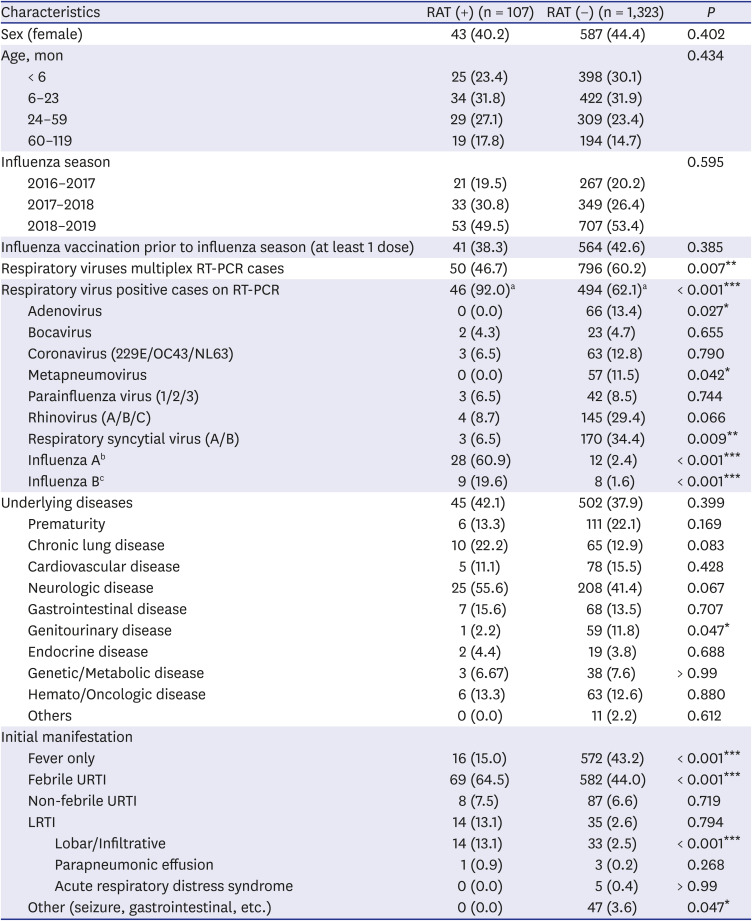
RAT = rapid antigen test, RT-PCR = reverse transcriptase polymerase chain reaction, URTI = upper respiratory tract infection, LRTI = lower respiratory tract infection.
Statistically significant P values were marked with asterisks (*P < 0.05, **P < 0.01, ***P < 0.001).
aThe percentages represent (respiratory virus positivity cases on RT-PCR)/(respiratory viruses multiplex RT-PCR cases).
bA total of 5 cases of co-respiratory viral infection with influenza A were as follows: rhinovirus (n = 2), adenovirus (n = 1), coronavirus (n = 1), and metapneumovirus (n = 1).
cA total of 4 cases of co-respiratory viral infection with influenza B were as follows: adenovirus (n = 1), bocavirus (n = 1), metapneumovirus (n = 1), and respiratory syncytial virus A (n = 1).
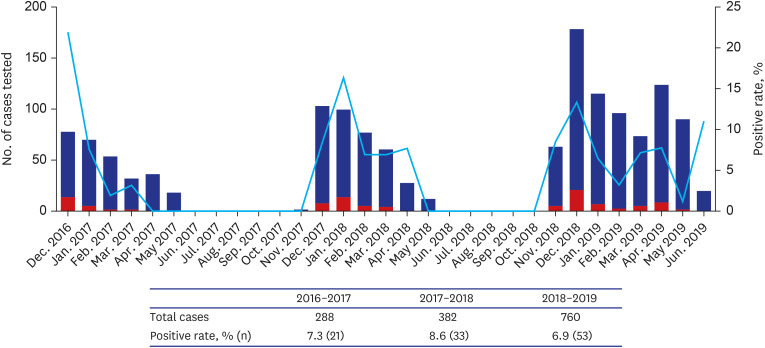
From the total study population who had undergone RAT, 1,323 (92.5%) were negative and 107 (7.5%) were positive for influenza. The number of RAT tested cases increased from 288 in 2016–2017 to 382 and 760 in 2017–2018, and 2018–2019, respectively with a relatively constant positivity rate (7.3% in 2016–2017, 8.6% in 2017–2018, 6.9% in 2018–2019; Fig. 2). There was no significant difference in age, sex, underlying disease, and vaccination status between RAT-positive and RAT-negative patients. However, children in the RAT-negative group were significantly more likely to undergo PCR-based assay than those in the RAT-positive group (60.2% vs. 46.7%, P = 0.007). There was no difference in the co-viral infection rate in the RAT-negative (7/20, 35%) and RAT-positive groups (15/46, 33%) among PCR-confirmed influenza patients (P > 0.99). Regarding initial symptoms, children in the RAT-positive group were about 1.5 times more likely to have febrile upper respiratory symptoms such as cough and rhinorrhea (64.5% vs. 44.0%, P < 0.001), and 5.3 times more likely to have an infiltrative type of LRTIs (13.1% vs. 2.5%, P < 0.001) than those in the RAT-negative group. Contrarily, children in the RAT-negative group were significantly more likely to have only fever (43.2% vs. 15.0%, P < 0.001), or non-respiratory manifestations such as seizures and gastrointestinal symptoms (3.6% vs. 0.0%, P < 0.045) than those in the RAT-positive group. The detailed characteristics of RAT-positive and RAT-negative groups are described in Table 1.
Impact of RAT on initiation of antiviral treatment
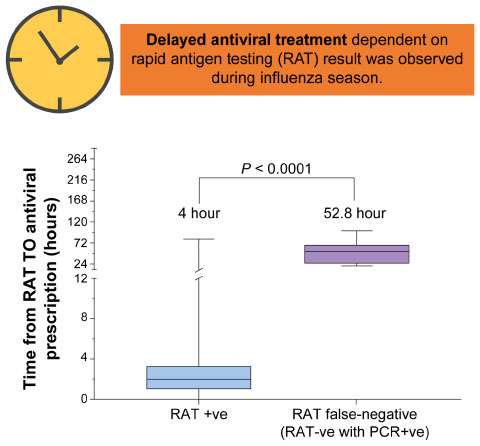
In this sub-analysis, a total of 127 children were included, 107 of whom were RAT-positive and 20 were RAT-false-negative (RAT-negative, PCR-positive). Among them, three patients in the RAT-positive group and 11 patients in the RAT-false-negative group were excluded. Two of these excluded patients had not received antivirals (due to symptom resolution), two had already received antivirals prior to the ED visit, and the remaining patients were missing data regarding treatment. The median TAT of the RAT-positive group was 4 hours (0.1–81.7 hours), which was significantly shorter than the median 52.8 hours (19.2–100.1) of the RAT-false-negative group (P < 0.001) (Fig. 3A). In addition, progression from URTI to LRTI during hospital stay of the RAT-false-negative group was 22.2% (n = 4), which was significantly higher than the 3.0% (n = 3) of the RAT-positive group (P = 0.01). Other clinical outcomes comparing the two groups are described in Supplementary Table 1. Moreover, patients who underwent PCR tests and those who did not undergo the test were compared and reported in Supplementary Table 2. The two groups showed no significant differences in age, gender, and comorbidities, except that in the more recent influenza season, greater number of PCR tests were done.
Fig. 3
(A) TAT difference between the RAT-positive and RAT-false-negative groups. (B, C) Multivariable analysis of the clinical outcomes by TAT (≥ 12 hours and ≥ 24 hours).
TAT = turnaround time to antiviral treatment, RAT = rapid antigen test, PCR = polymerase chain reaction, LRTI = lower respiratory tract infection, IFV = influenza virus, PICU = pediatric intensive care unit, OR = odds ratio, CI = confidence interval.
Statistically significant P values were marked with asterisks (*P < 0.05).

Impact of TAT on clinical outcomes
Next, the effect of TAT on clinical outcomes was analyzed. From the 127 children, 13 were excluded from the analysis due to unclear TAT data. In the univariable analysis, the group with a TAT of ≥ 12 hours was 4.6 times more likely to have severe influenza infection than the group with a TAT of < 12 hours (P = 0.018) (not shown). Furthermore, the group with a TAT of > 204 hours was 3.7 times more likely to develop LRTI (P = 0.039), 6.5 times more likely to have severe influenza infection (P = 0.005), 8.1 more likely to require PICU admission (P = 0.045), and 16.3 times more likely to require mechanical ventilation (P = 0.026). In the multivariable logistic regression analysis shown in Fig. 3B and C, after adjusting for age, sex, and underlying diseases, TAT of ≥ 12 hours and ≥ 24 hours were associated with 4.7 times and 6.8 times higher risk of severe influenza infection, respectively (P = 0.024, and P = 0.009, respectively). Other outcome parameters such as PICU admission, mechanical ventilation, LRTI, and severe LRTI, all exhibited increased risk by 8.0, 16.2, 3.6, and 4.2-fold respectively with a TAT of ≥ 24 hours. Only mechanical ventilation showed statistical significance (P = 0.033); However, the number of cases were low (n = 1 in mechanical ventilation, n = 3 in PICU admission); therefore, careful interpretation is needed.
Cost-benefit analysis by scenario
After analyzing the data of 846 patients who underwent RAT and PCR in parallel, the prevalence of true influenza per ILI patient was 6.6%, the sensitivity was 64.2%, and the specificity was 97.5% (assuming PCR testing is the gold standard). After extrapolating these values to the 1,430 total number of patients in our study, 34 were RAT-false-negative, 33 were RAT-false-positive, and 94 patients were assumed to be PCR-confirmed true influenza cases (Supplementary Table 3). Scenario 1 (RAT-based approach) has a short TAT of 4 hours and is fairly cost-beneficial (41,971 KRW/ILI case or 37.6 USD/ILI case), but 34 false-negative cases would not receive antiviral treatment. Scenario 2 (Empiric treatment-based approach) has the advantage of the cheapest medical cost (13,018 KRW/ILI case or 11.7 USD/ILI case) and no TAT (as empiric oseltamivir would be administered to all ILIs without delay). However, from the total of 1,430 patients, if 6.6% were true influenza cases, then 93.4% would be given antivirals unnecessarily according to scenario 2, amounting to 1,336 patients. Scenario 3 (PCR-based approach) treats all the true influenza patients but is time-consuming with a long TAT of 71 hours. In Scenario 4 (Hybrid approach), the TAT is variable from 4 hours to 71 hours and is the least cost-beneficial (209,356 KRW/ILI case or 187.3 USD/ILI case). Additionally, 33 RAT-false-positive patients would be prescribed antivirals unnecessarily (Table 2).
Table 2
Cost-benefit analysis according to influenza diagnosis and treatment scenarios in the ED
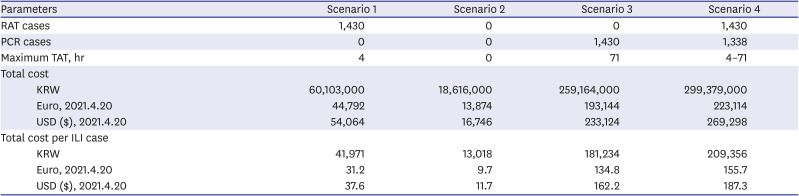
Scenario 1 (RAT-based): All patients undergo RAT. If RAT (+), then given oseltamivir. Scenario 2 (Empiric treatment): All patients receive empiric oseltamivir without testing. Scenario 3 (PCR-based): All patients undergo PCR. If PCR (+), then given oseltamivir. Scenario 4 (Hybrid): All patients take RAT. If RAT (+), then given oseltamivir. If RAT (−), test with PCR and then treat accordingly.
ED = emergency department, RAT = rapid antigen test, PCR = polymerase chain reaction, TAT = turnaround time to antiviral treatment, ILI = influenza-like illness.
DISCUSSION
Our study showed that hospitalized RAT-false-negative pediatric patients with influenza had a significantly longer TAT than RAT-positive patients. Influenza patients who received antivirals within 24 hours after RAT had a lower risk of severe influenza and mechanical ventilation than those who received antivirals later, but there was no difference in the frequencies of PICU admission, LRTI, and severe LRTI. Moreover, although RAT-first and PCR-confirmed hybrid approach showed false-negative case detection, it was less cost-beneficial.
Since the targets are not amplified in RATs, their sensitivity is inherently lower than that of PCR-based assays, leading to false-negative results, which in turn causes problems.812 A delay in the antiviral treatment of RAT-false-negative, hospitalized children was observed, as was its association with poor clinical outcomes. In our study, 2.4% of the patients (n = 20) who underwent RAT and PCR-based assay in parallel tested false-negative. When extrapolating that to the total number of 1,430 patients, 34 would have been falsely labeled as influenza negative. The median TAT of these RAT-false-negative patients was 52.8 hours (19.2–100.1, P < 0.001), which was significantly longer than the RAT-positive patients and was associated with a higher risk of progression from URTI to LRTI (22.2% vs. 3.0%, P = 0.010). Moreover, false-negative patients, in addition to improper antibiotic use, are at an increased risk of nosocomial transmission due to loosening of infection control measures and delaying proper quarantine. Because of these issues, the 2018 Infectious Diseases Society of America clinical guidelines recommend the use of PCR-based assays and not RATs for hospitalized patients during influenza season except when more sensitive molecular assays are not available (strength of recommendation A; quality of evidence, II; both).13 In addition, even if RAT is performed, it is recommended to follow up with a PCR-based assay (strength of recommendation A; quality of evidence, II; both). However, despite these recommendations, our study showed that there may be a delay in antiviral treatment initiation and subsequent risk of nosocomial transmission. Thus, empiric antiviral treatment and preemptive isolation need to be considered until the results of the PCR-based assay are confirmed.14
Early antiviral initiation is crucial for the treatment of influenza, and point-of-care testing helps clinicians make a decision regarding the prescription of antivirals.15161718 Our findings support that early antiviral treatment is associated with a better prognosis in hospitalized children with influenza.1920 Malosh et al.21 found that, in a meta-analysis of oseltamivir efficacy and safety in children, when the antiviral was given within 24 hours of symptom onset, the duration of illness was significantly reduced by 22.8 hours. However, the majority of existing studies on antivirals in children with influenza, including the aforementioned study, compared outcomes based on illness onset. Meanwhile, Coffin et al.20 conducted a retrospective multicenter cohort study using the Pediatric Health Information System database and reported an 18% reduction in duration of hospitalization in children treated with oseltamivir within 24 hours of admission. Our study is unique because we compared the outcomes of hospitalized children based on the time of the antiviral administration in the ED. We found that the risk of severe influenza infection was significantly reduced when antivirals were administered earlier, based on the time when RAT was performed (within 12 and 24 hours, respectively), irrespective of disease onset. However, there were no significant differences in other clinical outcomes such as PICU admission, LRTI, and severe LRTI. This is likely due to the low number of cases or inherent bias due to the retrospective nature of our study. There is a need for larger, well-designed studies to evaluate these outcomes.
The economic cost ranges from $11.7–$187.3 per ILI patient depending on the scenario, the greatest difference being 16-fold between the empiric and hybrid approaches. In the case of the RAT-based approach, the TAT is as short as 4 hours, and the cost is 20% of that of hybrid approach, which is the least cost-beneficial. However, 33 false-positive and 34 false-negative cases occurred based on the extrapolation, who either received unnecessary antiviral treatment or were subject to a higher risk of nosocomial transmission. On the other hand, in the case of the empiric treatment approach, the majority of non-influenza patients (93.4%, n = 1,336) would unnecessarily receive antivirals, despite its least economic cost. In addition, antiviral exposure may increase the risk of emerging antiviral-resistant strains and adverse reaction in children who do not require antiviral agents.2223 The hybrid approach was shown to be able to diagnose the false-negative patients of the RAT-based approach at a later time, at a 16-fold increased cost than the empiric approach. This suggests that the hybrid approach may be less cost-beneficial. Thus, for more appropriate antiviral treatment and nosocomial infection prevention and control, the introduction of a rapid PCR-based assay in Korea for ILI inpatients during the influenza season needs to be considered, as well as an analysis for its cost-effectiveness.24
This study had several limitations. Firstly, the PCR-based assay was not uniformly conducted on all patients. However, more than half of the patients (59.2%, n = 846) underwent PCR-based assay as well as RAT and based on this, the false-positive and false-negative rates were estimated for all patients. Secondly, the RAT-false-positive rate was 28% in those who underwent PCR test and RAT, simultaneously. However, we do not think that the RAT false positive rate influenced our primary outcome, because our primary objective was to investigate how delayed the actual antiviral initiation was, according to the actual RAT results. Nevertheless, this limitation has the potential to influence the secondary outcomes wherein we analyzed the clinical outcomes. Therefore, to more accurately analyze the clinical outcomes according to the initiation of antiviral agents in Korea, additional PCR-based research is needed. Thirdly, in our definition of ILI, we included patients with only fever, while the term is widely known to refer to fever accompanied by other respiratory symptoms. Nonetheless, in Korea, RAT is often performed in children who only presents with fever during influenza seasons. In our study, although fever with upper respiratory symptoms, such as cough and rhinorrhea, were the most common, 14.3% of laboratory-confirmed influenza patients had fever only. Also, from past prospective studies, it was observed that the positive predictive value of fever alone was 65–79%, which is lower than that of fever and cough of 64–83%, although this is relatively high.25 However, it is still necessary to be cautious about the possibility of false-positive cases due to indiscriminate use of RAT. Also, we collected data from single-center tertiary referral hospital, so more severe cases of ILI with comorbidities are likely to be reported than for the general population. Finally, this study was a retrospective one, and the numbers of study patients were insufficient to statistically compare critically severe outcomes, such as the PICU hospitalization.
Despite the aforementioned limitations, to our knowledge, this study is the first study to elucidate the association between delayed antiviral treatment and severe clinical outcomes other than antibiotic cessation and ED length of stay. Moreover, the cost-benefit analysis was evaluated based on different scenarios. Although the RAT-based approach is practical, it has a clear limitation of false-negativity due to low sensitivity when applied to children in the ED.
In conclusion, delayed antiviral treatment was observed in RAT-false-negative, pediatric patients with influenza. Further studies regarding the accuracy and usefulness of rapid PCR-based tests and also cost benefit analysis should be conducted. Until its implementation in Korea, our findings support the current guideline that children with influenza, suspected of having severe or progressive infection, should be treated immediately regardless of the RAT result.
 XML Download
XML Download