

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In diffuse large B-cell lymphoma (DLBCL), bone marrow involvement (BMI) has the important clinical implication as a component of the Ann Arbor staging and clinical risk-stratification index including the International Prognostic Index (IPI).12 For many years, unilateral bone marrow (BM) trephination has been regarded as the gold standard for the evaluation of BMI in patients with DLBCL.34 The extent of lymphoma cell infiltration in the BM is a highly significant negative prognostic factor.5 However, BM trephination biopsy has some limitations of, namely, low sensitivity to patchy or focal BM involvement, inter-observers’ flexibility, and technical problems such as inappropriately obtained specimens.6
Recent studies demonstrated that 18F-FDG positron emission tomography-computed tomography (PET/CT) possesses adequate sensitivity for the detection of BMI in patients with DLBCL.789 PET/CT is a non-invasive assessment for detecting BMI, seen as focal areas of FDG uptake, often with no morphological abnormality on corresponding CT images.10 The National Comprehensive Cancer Network (NCCN) and European Society for Medical Oncology (ESMO) guidelines also recommended that BM trephination biopsy is not necessary if the PET/CT scan demonstrates BMI and that the therapeutic modalities should not be changed.10111213 Our previous studies reported that high metabolic tumor volume, which indicates the extent of malignant lymphoid cell infiltration in the BM, had negative prognostic outcome compared with other clinical risk factors.1415 On the contrary, as 18F-FDG is not a tumor-specific contrast agent, it might accumulate in extra nodal sites in patients with other benign conditions.15 These characteristics could lead to a false positive result. The pitfalls of PET/CT interpretation in BMI might be associated with the definition of marrow involvement (focal vs. diffuse infiltration) without taking into considerations the anatomic variations or inflammatory physiology in DLBCL.16
Most of the patients with lymphoproliferative disorder can be diagnosed by histomorphology or cytomorphology.1718 However, the morphological features in 5–15% of patients are not typical and can be difficult to diagnose.18 In such cases, the immunoglobulin gene rearrangements could be useful for determining the clonality of lymphoproliferative tissues.18 The detection of lymphoid clonality by immunoglobulin gene rearrangement is an important method in the diagnosis of and in predicting the prognosis of lymphoid malignancy.1920 Because the immunoglobulin heavy chain (IgH) gene rearranged when malignant B lymphoid cells were developing, IgH gene is considered the most valuable gene target for detecting B-cell clonality in previous studies.2122 Immunoglobulin gene rearrangement analysis performed by polymerase chain reaction (PCR) test such as the BIOMED-2 multi target PCR approach has been a helpful method for detecting the clonality of B-cell lymphoid malignancy, and the detection rates of PCR analysis increased with the combined use of immunoglobulin gene rearrangement.232425 However, only a few studies have evaluated the accuracy of PCR analysis for molecular staging and focused on adjusting the results based on the clinical outcome.262728
The aim of this prospective cohort study was to determine whether molecular analysis of immunoglobulin heavy chain (IgH) genes and PET/CT could increase the diagnostic accuracy or predict the survival outcome compared to conventional trephination biopsy in the rituximab-containing treatment of DLBCL.
METHODS
Patients’ characteristics
Patients diagnosed with de novo DLBCL between January 2017 and May 2018 were enrolled from a single institution. Patients (a) aged 19 years or older with a confirmed diagnosis of DLBCL according to the 2016 World Health Organization (WHO) criteria; (b) who underwent PET/CT, IgH gene arrangement PCR assessment, and unilateral trephination BM biopsy at diagnosis; and (c) with no malignancy other than lymphoma at the time of diagnosis, were included in the cohort.
Of note, patients with primary central nervous system involvement or who refused to participate in the study after the diagnosis were excluded. Clinical parameters, including age at diagnosis, sex, histology, Ann Arbor staging, IPI, initial rituximab-containing treatment schedule, date of relapse, date of death, or documented date of last visit, were collected. Morphologic BM involvement was used to classify Ann arbor stage IV at diagnosis. This study was approved by the institutional review board, and all patients provided a written informed consent.
Patients received six cycles of rituximab (R) with cyclophosphamide, vincristine, doxorubicin, and prednisolone (CHOP) chemotherapy in standard doses every 3 weeks. Those with stage I received three cycles of R-CHOP chemotherapy prior to the administration of involved-field radiation therapy (IFRT).
Morphologic BMI by BM trephination biopsy
BM trephination section biopsy and aspirate smears from DLBCL patients who had positive morphologic BMI (mBMI) were reviewed by an experienced hematopathologist in accordance with the WHO criteria. Based on the results of the morphological examination and immunohistochemistry, the extent of lymphoma cell infiltration and histology of the lymphoid infiltrates suggested an mBMI. Concordant mBMI was defined as BM involving mostly large non-cleaved DLBCL cells. Disconcordant mBMI was defined as BM involving mostly small and low-grade lymphoma cells.5
18F-FDG PET/CT and image analysis
All patients underwent 18F-FDG PET/CT with a PET/CT system Discovery ST scanner (GE Healthcare) at initial diagnosis. After fasting for 6 hours, 18F-FDG was injected intravenously (calculated dose: 7.4 MBq per kg), and the patients’ serum glucose levels were evaluated. CT scan was performed from the skull base to the proximal thighs. The transmission data were obtained 60 minutes after the injection of 18F-FDG with a low-dose CT using the following imaging parameters: rotation time (0.8 s), slice thickness (3.75 mm), automated from 10 to 130 mA, 120 kV, and a 50-cm field of view (FOV) with a 512 × 512 matrix. PET emission acquisition was performed in the same anatomic locations immediately after the CT scan using the following parameters: axial FOV (15.7 cm) with a 128 × 128 matrix. The examinations were reconstructed according to the conventional iterative algorithm. The CT data were applied for attenuation correction. PET/CT images were evaluated and confirmed visually with standardized uptake value by consensus of two experienced nuclear medicine physicians. The normal FDG BM uptake was determined when it was lower than or corresponding to that in the liver. Focal FDG BM uptake was visually defined as one or several focal bone uptakes in PET images with or without bone lesion in CT images and when it was higher than that in the liver and lower than that in the brain. We subdivided Focal FDG BM uptake into cases with iliac crest bone uptake and without iliac crest bone uptake. Diffuse FDG uptake in the BM was visually categorized as diffuse heterogenous FDG uptake higher than that of normal liver without focal lesions. Diffuse homogenous FDG BM uptake with other benign condition such as inflammation or severe anemia was excluded.
Clonal gene rearrangements by PCR analysis
DNA was extracted from the BM aspirations and Formalin-Fixed Paraffin-Embedded tissue specimens submitted for unilateral trephination biopsy which was conducted at the time of DLBCL diagnosis. QIAamp® DNA mini Kit (QIAGEN, Valencia, LA, USA) was used to isolate the DNA from BM samples in accordance with the manufacturer’s instructions. The quantity of the extracted DNA was assessed using a spectrophotometric system (NanoDropTM ND-1000, NanoDrop Technologies, Wilmington, DE, USA).
The clonality of B-cell neoplasms was examined by conducting a BIOMED-2 clonality assay, while the IgH clonal gene rearrangements were detected using the IdentiClone IGH Gene Clonality Assay (Invivoscribe Technologies, San Diego, CA, USA) following the manufacturer’s instructions. The PCR IGH multiplex PCR reactions, such as VH-JH gene rearrangement and DH-JH gene rearrangement, were used to evaluate the IGH clonality (V, variable; D, diversity; and J, joining gene segments, respectively). The product of PCR reaction was diluted with Hi-Di TM Formamide (Applied Biosystems, Foster city, CA, USA) and distilled water. The sample was analyzed by laser-induced fluorescence capillary electrophoresis using Genetic Analyzer 3000 (Applied Biosystems) following the manufacturer’s instructions. Monoclonality was defined as the occurrence of one distinct peak within the expected size ranges as per the BIOMED-2 protocol and the largest peak being at least three times higher than the third largest peak in the polyclonal background.1829
Statistical analysis
Data analysis was performed using SPSS software version 26.0. and R software version 3.1.0. Clinical characteristics and diagnostic assessments were analyzed using the chi-square tests for categorical variables, and two-sided Student’s t-test was used for analyzing the quantitative variables. When analyzing diagnostic assessments, morphologic BMI was taken as the reference standard.30 The parallel test was used to determine sensitivity, specificity of IgH PCR or PET/CT, the serial test was used to determine sensitivity and specificity of combined IgH PCR and PET/CT for detecting BMI. The receivers operating characteristic for detecting PET BMI was measured using the area under the curve, Youden indexes, and optimal cut-off value. Positive predictive value and negative predictive value (NPV) for detecting BMI were assessed based on Bayes’ rule. Progression-free survival (PFS) was the primary endpoint of this study and was calculated from the date of diagnosis of DLBCL to the date of disease progression, relapse, death, or last follow-up. The secondary endpoint was overall survival (OS), which was calculated from the period of DLBCL diagnosis to the date of death or last follow-up. The Kaplan-Meier method was used to analyze the PFS and OS. Breslow test and log rank test were used to compare the survival outcomes. Cox regression models and Breslow test were used for the multivariate analysis of various independent prognostic factors. P values of less than 0.05 were considered significant.
Ethics statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the Chonnam National University Hwasun Hospital on 10 December 2019 (IRB No. CNUHH-2019-210). Informed consent was obtained from all subjects involved in the study
RESULTS
Patients’ characteristics
Ninety-four patients with de novo DLBCL were eligible. With the median age of 66.0 years (range: 24–85 years), 16 (17.0%) patients were diagnosed with stage I, 28 (29.8%) with stage II, 24 (25.5%) with stage III, and 26 (27.7%) with stage IV disease. Based on IPI risk classification, 35 (37.2%) patients were classified as the low-risk group, 23 (24.5%) as the low-to-intermediate-risk group, 20 (21.3%) as the high-to-intermediate risk group, and 16 (17.0%) as the high-risk group, respectively. Positive mBMI using trephination section biopsy was detected in 9 patients (9.6%; concordant mBMI = 6 and disconcordant mBMI = 3), while IgH clonality (IgH BMI) was detected in 21 patients (22.3%). On the other hand, positive BM 18F-FDG PET uptake (PET BMI) was observed in 16 patients (17.0%). Among those with positive PET BMI, 11 patients had a focal type (68.8%, 11/16; focal with iliac crest lesion = 1 and focal without iliac crest lesion = 10) and 5 (31.2%) had a diffuse type. In addition, 5 patients with positive PET BMI were concordant with conventional mBMI and 6 patients were with positive IgH clonality. All patients were basically treated with six cycles of R-CHOP chemotherapy, except 8 (8.5%) patients with stage I who were treated with IFRT after three cycles of R-CHOP. Other details of the clinical characteristics were summarized in Table 1. The distribution classification of patients with BMI is shown in Table 2. The distribution of patients with PET BMI is shown in Table 3. Fig. 1 described the examples of PET/CT images with different pattern of FDG BM uptakes in patients with DLBCL.
Table 1
Clinical characteristics of DLBCL patients (n = 94)
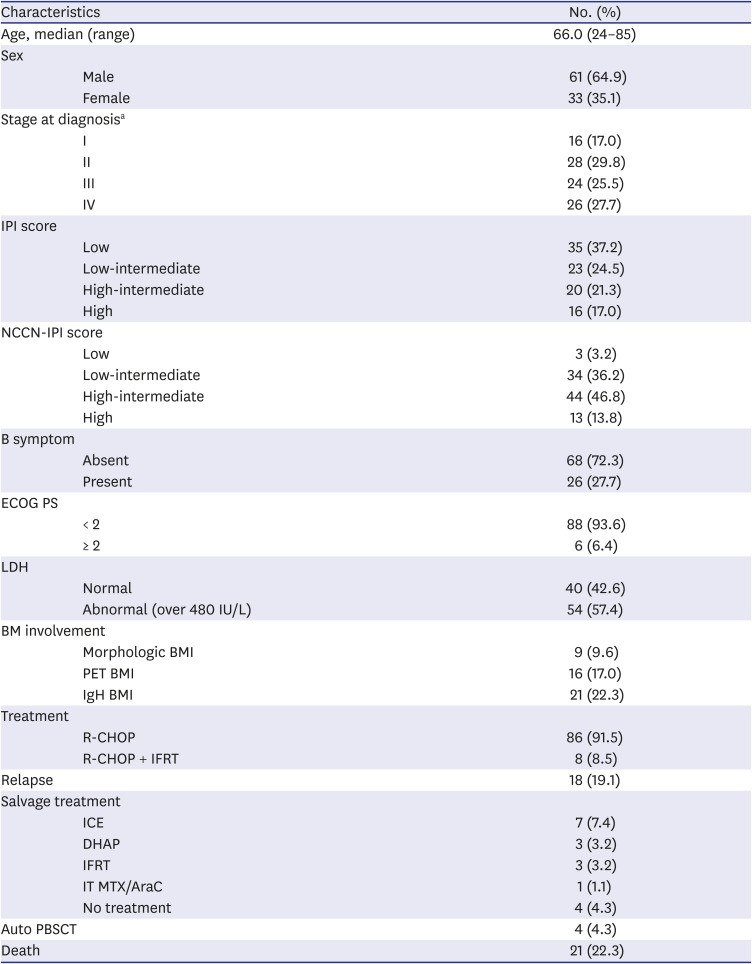
DLBCL = diffuse large B-cell lymphoma, IPI = international prognostic score, NCCN-IPI = National Comprehensive Cancer Network-IPI, ECOG PS = Eastern Cooperative Oncology Group performance score, LDH = lactate dehydrogenase, BMI = bone marrow involvement, PET = positron emission tomography, IgH = immunoglobulin heavy chain gene rearrangement, R-CHOP = rituximab with cyclophosphamide, doxorubicin, vincristine, and prednisone, IFRT = involved-field radiation therapy, ICE = etoposide, carboplatin, and ifosfamide, DHAP = dexamethasone, cisplatin and cytarabine, IT MTX/AraC = intrathecal methotrexate and cytarabine, Auto PBSCT = autologous peripheral blood stem cell transplantation.
aMorphologic BM involvement was used to classified Ann arbor stage IV at diagnosis.
Table 2
Distribution of patients whose bone marrow was assessed by PET/CT, IgH gene rearrangement PCR, and unilateral trephination BM biopsy
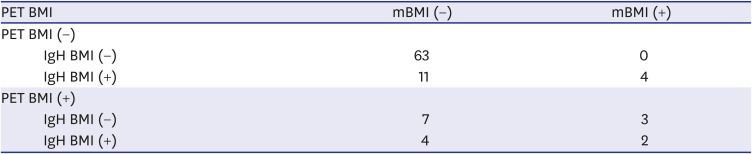
| PET BMI | mBMI (−) | mBMI (+) | |
|---|---|---|---|
| PET BMI (−) | |||
| IgH BMI (−) | 63 | 0 | |
| IgH BMI (+) | 11 | 4 | |
| PET BMI (+) | |||
| IgH BMI (−) | 7 | 3 | |
| IgH BMI (+) | 4 | 2 | |
Table 3
Distribution of patients with PET BMI

| PET BMI | mBMI (−) | mBMI (+) |
|---|---|---|
| Focal FDG BM uptake with iliac crest | 0 | 1 |
| Focal FDG BM uptake without iliac crest | 9 | 1 |
| Diffuse FDG BM uptake | 2 | 3 |
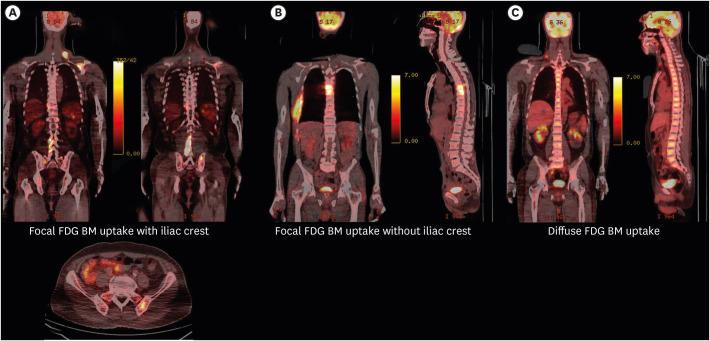
Fig. 1
Case example of PET/CT images showing FDG BM uptake in DLBCL patients. (A) Coronal images show focal increased marrow FDG uptake with iliac crest. (B) Coronal and sagittal image show focal increased FDG BM uptake in T6-T7 vertebrae without iliac crest. (C) Coronal and sagittal images show diffuse increased FDG BM uptake.
FDG = fluorodeoxyglucose F 18, PET/CT = positron emission tomography-computed tomography, DLBCL = diffuse large B-cell lymphoma.
Detection of BMI by PET/CT and IgH rearrangement
Among 16 patients with PET BMI, five patients (31.3%, focal with iliac crest lesion = 1, focal without iliac crest lesion = 1, and diffuse uptake = 3) with PET BMI were concordant with those of patients with mBMI. However, 11 patients (68.8%) with PET BMI did not match with conventional mBMI including 9 patients with focal metabolic involvements of BM and 2 patients with diffuse uptakes. In contrast, four patients (44.4%) with positive mBMI were not detected BMI based on PET/CT assessment. Particularly, these discordant patients had low standard uptake values at BM sites compared to those with the involved systemic lymphoma lesions. However, these four discordant patients were detected positive IgH BMI by PCR rearrangement. Based on clonal gene rearrangement, 21 patients showed the positive clonal rearrangement. Six out of 9 patients (66.7%) with conventional mBMI were concordant with IgH rearrangement. 15 patients without conventional mBMI were detected with the IgH clonality and associated with advanced stage. In addition, 63 patients with negative IgH BMI were concordant with negative PET BMI. The diagnostic accuracy of IgH BMI was 80.9% and the sensitivity, specificity, and NPV were 66.7%, 82.4%, and 92.7%, respectively. The diagnostic accuracy of PET/CT assessment was 82.0% with the sensitivity, specificity, and NPV of 55.6%, 87.1%, and 91.0%, respectively. Either IgH rearrangement PCR or PET/CT showed the high NPV. The combined assessment of IgH rearrangement and PET/CT could increase the diagnostic accuracy (87.2%) with the specificity of 97.0% (Table 4).
Table 4
Assessment of bone marrow involvement

PPV = positive predictive value, NPV = negative predictive value, CI = confidence interval, IgH = immunoglobulin heavy chain gene rearrangement, PCR = polymerase chain reaction, PET/CT = positron emission tomography-computed tomography.
aValues shown in Table 2 were used for calculations as standard formulas for sensitivity, specificity, PPV, NPV.
bTo evaluate the optimal cut-off value for PET/CT for detecting BMI, receiver operating characteristic analysis was performed using the area under the curve, Youden indexes. Optimal cut-off value was 1.0mCi and the area under the curve was 0.708.
cParallel test was used to determine sensitivity, specificity of IgH PCR or PET/CT. Serial test was used to determine sensitivity and specificity of combined IgH PCR and PET/CT for detecting BMI.
d95% CI and their P values for NPV were shown in Table 4.
Clinical correlation according to the results of the combined detection of PET/CT and IgH rearrangement
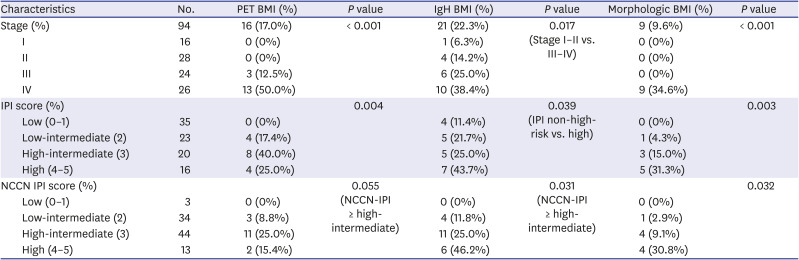
A clinical correlation was found between positive mBMI and IPI (P = 0.003), NCCN-IPI risk groups (P = 0.032). A significant difference of positivity was observed in PET BMI status depending on clinical stages (P < 0.001). Moreover, a clinical correlation was also found between positive PET BMI and IPI risk groups (P = 0.004). A significant difference of the IgH BMI status was observed between patients with Stage I–II (5 of 47 patients; 10.6%) and those with stage III–IV (16 of 47 patients; 30.0%, P = 0.017). The detection of IgH BMI was significantly increased in high-risk patients, depending on the IPI risk classification (IPI non-high risk vs high risk, P = 0.039) in Table 5.
Table 5
Clinical characteristics of 94 patients with DLBCL according to the PET BMI and IgH BMI, mBMI status
Survival outcomes based on PET/CT and IgH arrangement assessment
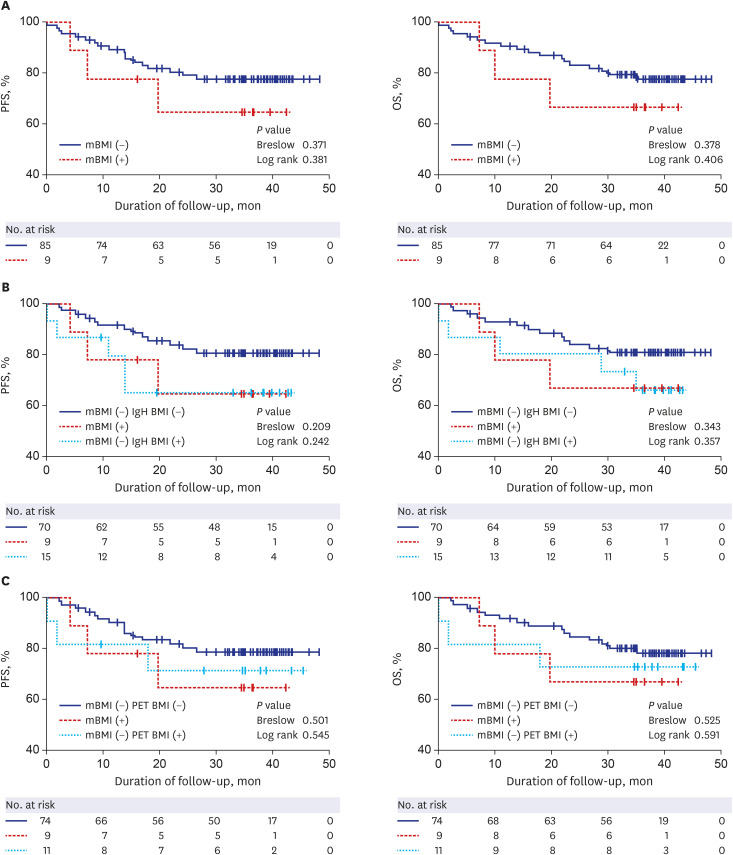
The median duration of follow-up was 35.2 months (range: 22.96–47.4). During the follow-up, 18 patients (19.1%) experienced disease progression and 21 (22.3%) expired. In the whole population, the estimated 3-year PFS was 76.6 ± 4.4%, and the estimated 3-year OS was 76.6 ± 4.5%, respectively. Patients with conventional mBMI showed relatively poor PFS and OS compared with those without mBMI (P > 0.05; Fig. 2A). The survival of patients (n = 15) with negative mBMI and positive IgH BMI were similar to patients (n = 9) with positive mBMI (P > 0.05; Fig. 2B). Patients (n = 11) with PET BMI (+) and mBMI (−) were associated with shorter survival outcome than those (n = 74) with mBMI (−) and PET BMI (−) (P > 0.05; Fig. 2C).
Fig. 2
Kaplan-Meier survival curves of patients with diffuse large B-cell lymphoma according to the bone marrow involvement status assessed by (A) BM biopsy; (B) combined assessment with polymerase chain reaction-based clonality and morphology; (C) combined assessment with PET/CT and morphology. Survival panels present the 3-year PFS curves (left) and 3-year OS curves (right). Statistical differences were calculated using the Breslow test and log rank test.
PFS = progression-free survival, mBMI = morphologic bone marrow involvement, IgH BMI = immunoglobulin heavy chain rearrangement bone marrow involvement, OS = overall survival, PET BMI = positron emission tomography-computed tomography bone marrow involvement.
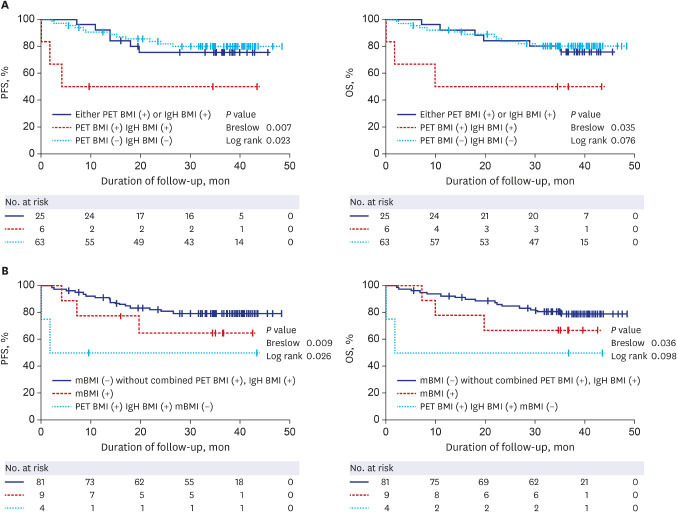
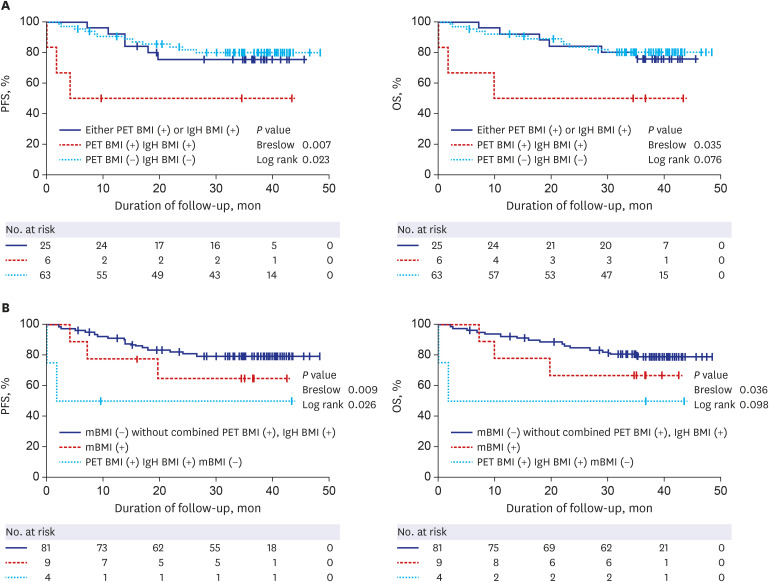
The survival outcome of patients (n = 6) with double positive PET BMI and IgH BMI were significantly worse than those (n = 25) with either positive PET BMI or IgH BMI, and even less than those (n = 63) with neither PET BMI nor IgH BMI (3-year PFS: 50.0% vs. 75.4% vs. 97.9%, P = 0.007, 3-year OS: 50.0% vs. 75.6% vs. 80.1%, P = 0.035; Fig. 3A). Within patients with negative conventional mBMI, moreover, the combined positive PET BMI and IgH BMI were significantly associated with short survival outcome (3-year PFS: 50.0% vs. 64.8% vs. 79.3%, P = 0.009, 3-year OS: 50.0% vs. 66.7% vs. 79.1%, P = 0.036; Fig. 3B).
Fig. 3
Kaplan-Meier survival curves of patients with diffuse large B-cell lymphoma according to the bone marrow involvement status assessed by (A) combined PET/CT and PCR-based clonality; (B) combined assessment with PET/CT, PCR-based clonality and morphology. Survival panels present the 3-year PFS curves (left) and 3-year OS curves (right). Statistical differences were calculated using the Breslow test and log rank test.
PFS = progression-free survival, PET BMI = positron emission tomography-computed tomography bone marrow involvement, IgH BMI = immunoglobulin heavy chain rearrangement bone marrow involvement, OS = overall survival, mBMI = morphologic bone marrow involvement, PET/CT = positron emission tomography-computed tomography, PCR = polymerase chain reaction.
Prognostic factors for survival outcomes
PFS was significantly associated with age (> 60, P = 0.032), B symptom (P = 0.023), Eastern Cooperative Oncology Group (ECOG) performance score (≥ 2, P = 0.009), IPI (P = 0.046), NCCN-IPI (P = 0.004, Supplementary Fig. 1) and combined assessment of PET BMI and IgH BMI (P = 0.007) on univariate analysis. On multivariate Cox-regression analysis, combined assessment of PET BMI and IgH BMI (P = 0.030; hazard ratio [HR], 4.83; 95% confidence interval [CI], 1.17–19.97), Age (> 60, P = 0.027; HR, 4.04; 95% CI, 1.17–14.01) were independent prognostic factors of PFS. OS was significantly associated with age (> 60, P = 0.031), B symptom (P = 0.026), ECOG performance score (P = 0.026), NCCN-IPI (P = 0.003, Supplementary Fig. 1) and combined assessment of PET BMI and IgH BMI (P = 0.035) on univariate analysis. On multivariate analysis, NCCN-IPI (P = 0.036; HR, 1.91; 95% CI, 0.73–5.03) was only found to be an independent prognostic factor (Table 6).
Table 6
Univariate and multivariate Cox-proportional hazard regression analyses predicting PFS and OS in DLBCL patients
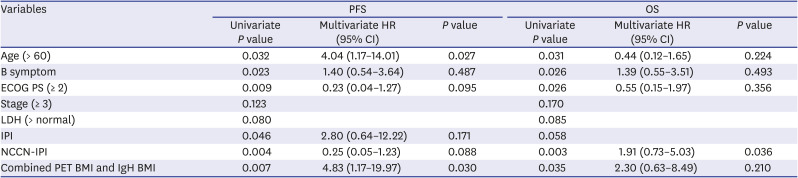
Univariate analysis and multivariate Cox-proportional hazard regression analysis was conducted using the Breslow method. Multivariate analysis was performed using the covariates, which showed a P value of less than 0.05 in the univariate analysis.
PFS = progression-free survival, OS = overall survival, DLBCL = diffuse large B-cell lymphoma, CI = confidence interval, HR = hazard ratio, ECOG PS = Eastern Cooperative Oncology Group performance score, LDH = lactate dehydrogenase, IPI = International Prognostic Index, NCCN-IPI = National Comprehensive Cancer Network-IPI, PET BMI = positron emission tomography-computed tomography bone marrow involvement, IgH BMI = immunoglobulin heavy chain rearrangement bone marrow involvement.
DISCUSSION
BM infiltration of lymphoma cells is one of the important prognostic factors of DLBCL.1 Unilateral BM trephination biopsy has been conducted to confirm BMI.3 If the additional less invasive tools for determining BMI can use for detecting focal or diffuse BM involvement, it will be helpful to determine diagnosis or prognosis in patients with DLBCL. Many approaches have been used for determining BMI, such as PCR amplification of immunoglobulin gene rearrangement or FDG/PET-CT.112426313233 To our knowledge, this was the first trial to evaluate the prognostic value of a combination of FDG PET/CT and PCR-based clonality for the treatment of DLBCL. This prospective cohort study from a single institution aimed to evaluate the diagnostic and prognostic significance of BM assessment in DLBCL according to the IgH gene rearrangement as well as FDG PET/CT compared with conventional BM biopsy. Nine patients showed positive mBMI in 94 enrolled patients, which was relatively lower than generally known.23435 Of the 85 patients with negative mBMI, 65 patients showed no definitive lymphoid clusters, whereas 20 showed relatively few lymphoid aggregates in conventional BM biopsy. These were predominantly composed of weak positive CD20, BCL2 cells. 22 patients (22 out of 85 patients) with negative mBMI were detected with positive PET BMI or IgH BMI. The characteristics of positive mBMI were not concordant with those of focal PET BMI without iliac crest lesion. The discordance of three detecting methods mainly occurred due to anatomic sites. Focal FDG uptake of BM without diffuse iliac crest may not be detected as morphologic BM biopsy, resulting in inconsistency between positive PET CT and morphologic BMI. This finding may suggest that focal PET BMI without iliac crest could indicate BMI without mBMI. The assessment of diffuse FDG uptake remained controversial in several studies.3136 However, some patients with diffuse BM uptake showed positive mBMI.32 Our study showed that three patients with diffuse PET BMI were matched with positive conventional mBMI. Berthet et al.33 reported that PET BMI was an independent predictor of PFS, but not of OS in the multivariate analysis. In the study, the multivariate analysis showed that age and NCCN-IPI were important negative prognostic factors. In addition, a combination assessment of PET BMI and IgH BMI were important independent factors of PFS.
Several approaches have been used for the detection of IgH gene rearrangement in patients with BMI.181923 Diagnosis based on the morphological features and cytomorphological features can be subjective and may differ depending on the different subsets of marrow invasion. Compared with previous studies, the study similarly found that the clinical characteristics of concordant mBMI were associated with poor ECOG performance status, high-intermediate standard, and NCCN-IPI risks, compared with the discordant morphologic marrow involvements.373839 Complete response (CR) was achieved in all three patients with discordant mBMI, however, half of patients with concordant mBMI failed to achieve a CR after R-CHOP chemotherapy. All three patients with discordant atypical morphology or focal marrow invasion had IgH rearrangement. Compared with previous studies, the study similarly found the positive clonal IgH in 15 of 85 (17%) patients with negative mBMI.24264041 Patients with negative mBMI and positive IgH BMI were significantly associated with high serum lactate dehydrogenase (LDH) level, advanced stage, and high standard and NCCN-IPI risks than patients with mBMI (−) and IgH BMI (−). A combination of PCR technique and PET/CT assessment could increase the accuracy of identifying BMI, and high NPV of IgH rearrangement may help to evaluate prognosis of negative mBMI.
The study had several limitations. First, molecular PCR analysis was performed at BM samples. Molecular PCR assessment in peripheral blood should be investigated further including the method of circulating tumor-DNA detection. If a correlation between peripheral blood and BM aspiration samples to detect clonal Ig gene rearrangement exists, these can be used to detect a BMI or minimal residual disease in the clinical setting. Second, an increase in FDG BM uptake (diffuse or focal) was interpreted as an indication of BMI without the definitive cut-off of standard uptake value. Because low FDG BM uptake was not reliably visualized with PET BMI, 4 patients with positive mBMI were classified with negative PET BMI. Regardless of these limitations, the data suggested that the patients with double positive PET BMI and IgH BMI were significantly associated with poor survival outcome. Mitterbauer et al.24 reported that negative mBMI and positive IgH BMI were significantly worse than negative mBMI and negative IgH BMI. In our study, patients with combined positive IgH BMI and PET BMI without detecting mBMI showed poor survival outcome than those with negative conventional mBMI. It could give additional information to patients with negative morphologic BMI.
In conclusion, the study suggests that the combined assessment with IgH gene rearrangement PCR and PET/CT could give additional information for detecting the BMI in patients with DLBCL. The assessment of BMI based on PET/CT and IgH gene rearrangement PCR is an indicator to predict the survival outcomes of DLBCL, particularly in patients with negative conventional mBMI.
 XML Download
XML Download