

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rheumatic diseases (RDs) such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and ankylosing spondylitis (AS) occur often in women of childbearing age.123 In SLE, the male-to-female ratio of disease incidence is 1:9, and this ratio increases up to 1:15 in individuals of reproductive age.4 Furthermore, the incidence and prevalence rates peak in women during their childbearing years.3 RA is also approximately 2 times more prevalent among women than among men,5 and the female-to-male ratio is 3.7:1 before 30 years of age but decreases to 1:1 after the 6th decade of life.6 AS occurs more frequently in men, but the proportion of women with a new diagnosis of AS has been increasing, especially in women of childbearing age.7
Pregnancy is a common issue among women with RDs since women are often diagnosed with these diseases before encountering pregnancy. Although pregnancies in women with RDs are usually successful due to improved care,8910 women with RDs are at increased risk of adverse pregnancy and offspring outcomes. Population-based cohorts have demonstrated that women with SLE have more pregnancy complications such as preeclampsia/eclampsia (PE/E), preterm birth (PB), and intrauterine growth retardation (IGR) than the general population.11 Although pregnancy complications were less frequently found in patients with RA than in those with SLE, slightly less favorable outcomes were demonstrated in RA pregnancies than in the pregnancies of unaffected women with an increased risk of IGR and PE.9 Women with AS have been shown to have an increased risk of cesarean section (C-section) compared with healthy women,1213 and an increased risk of prematurity was reported in 2 case control studies.1314 Pregnancy complications are closely linked to adverse offspring outcomes. Offsprings of women with SLE, RA, and AS have been shown to have increased risk of being small for their gestational age.81516 In addition, a decreased chance of a liveborn child has been demonstrated in women with RA and SLE.1718 Since the manifestations of RDs and practice patterns are highly variable among populations with different ethnic and socioeconomic backgrounds,1920 determining the risk of pregnancy complications and adverse offspring outcomes in different populations can provide holistic view of the disease burden on women with RDs. Therefore, this study aimed to determine the risk of pregnancy complications and adverse offspring outcomes in Korean women with RDs of childbearing age using a nationwide population database.
METHODS
Data source
In this retrospective cohort study, we used data from the National Health Insurance Service-National Health Information Database (NHIS-NHID), which is a longitudinal database containing the healthcare records and claims data of approximately 50 million national insurance subscribers and their dependents in South Korea. The NHIS database includes all inpatient and outpatient claims data and information on health utilization including medical history, diagnosis, and prescription information.21 Demographic variables include information regarding gender, age, region of residence, subscriber classification, and income quartile. For this study, pregnancies ending in delivery in women of childbearing age (defined as women between the ages of 20 and 44 years) were selected from data collected during the period from January 1, 2009, to December 31, 2016. A pregnancy ending in delivery was defined as a case when the according International Classification of Diseases (ICD) 10th revision codes, O80-84 was included as a principal diagnosis or first additional diagnosis. Women could have multiple pregnancies ending in delivery captured during the study period, and each pregnancy ending in delivery was considered an independent event. Offsprings were identified by matching the maternal and offspring health insurance numbers in the NHIS-NHID during the study period.
Study population
The study population included a cohort of cases and controls. We investigated women with seropositive RA (SPRA), SLE, and AS between the ages of 20 and 44 years identified by the ICD-10 diagnostic codes of M05, M32, and M45, respectively, in the NHIS-NHID during the study period. SPRA, SLE, and AS were selected as they are representative RDs that occur frequently in women of reproductive age. Among them, only women diagnosed with SPRA, SLE, or AS before the date of delivery were selected as the patient group. In 2009, the government of the Republic of Korea subsidized medical expenses for patients with rare and intractable diseases through a copayment assistance policy called the Individual Copayment Beneficiaries Program (ICBP), and SPRA, SLE, and AS were designated as rare diseases covered by this program. Under the ICBP system, the NHIS established a registration program that includes codes for the targeted diseases classified according to the Korean Standard Classification of Diseases (KCD)-7 (based on the ICD-10), date of definitive diagnosis, and tests performed to confirm the diagnosis. In the ICBP, an RD is defined as a case that satisfies existing criteria (SLE: 1997 American College of Rheumatology [ACR] criteria22 or 2012 Systemic Lupus International Collaborating Clinics criteria23; SPRA: 2010 ACR/European Alliance of Associations for Rheumatology [EULAR] classification criteria24 or 1987 ACR classification criteria; AS: 1984 modified New York criteria25) at the physician’s judgment. We used data from January 1, 2009, with the assumption that all patients with SPRA, SLE and AS were accurately coded since ICBP registration required fulfillment of classification criteria for definitive diagnosis.
For control selection, women who were age-matched and did not have ICD-10 codes for SPRA, SLE, and AS were randomly sampled in a 1:5 ratio to women with SPRA, SLE, and AS. Among these women, those with chronic diseases (hypertension [I10-12,15], hyperlipidemia [E78], diabetes mellitus [E10-14], and cancer [C]) were excluded, and the follow-up period of the patient group was matched. Finally, those who gave birth during the study period were selected as a control group.
Outcome measures
Delivery methods and pregnancy complications were defined as cases in which the relevant ICD-10 codes were included in the principal diagnosis or first additional diagnosis. The pregnancy period was defined using the delivery date as a reference point including a period between 266 days before the delivery date to the delivery date. Only complications occurring within the pregnancy period were included. Delivery methods included C-section [O82] and normal spontaneous vaginal delivery [O80,81,83,84]. Pregnancy complications included threatened abortion (TA) [O200,262,312], PB [O601], PE/E [O141,149], IGR [O358,365], and urinary tract infection (UTI) [O230,231,234,235,239]. The prevalence of low birth weight (LBW) offsprings and offspring death within 1 year of birth were measured to determine offspring outcomes. LBW was defined as a case in which a principal diagnosis or first additional diagnosis included the ICD-10 codes P0700-2, P0709-14. A date of death registered in the offspring's health insurance eligibility information was used to determine the number of deaths occurring within 1 year. The offspring mortality rate within 1 year was calculated by dividing the number of offspring deaths occurring within 1 year of birth by the number of person-years in the same observation period.
Statistical analysis
Discrete variables are described as frequencies and percentages, and continuous variables are described as the mean and standard deviation (SD). The rates of C-section between the RD and control groups were compared using the χ2 test. For infant data, the χ2 test was used to compare the proportions of LBW infants between the RD and control groups. Odds ratios (ORs) with 95% confidence intervals (CIs), adjusted for age, income level, and residential district, were used to compare the RD and control groups. Odds ratio was determined using multiple logistic regression. Statistical significance was set at P < 0.05. All analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA).
RESULTS
Characteristics of the study population
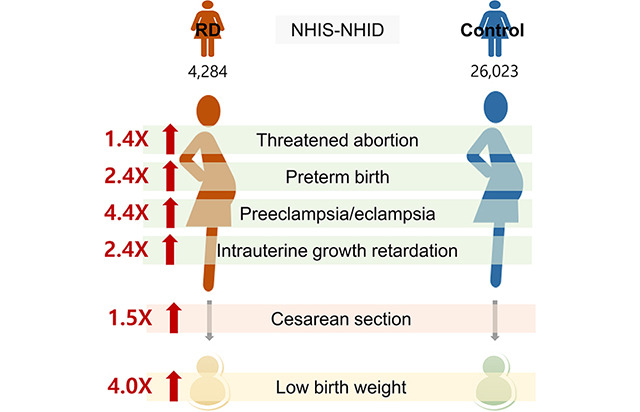
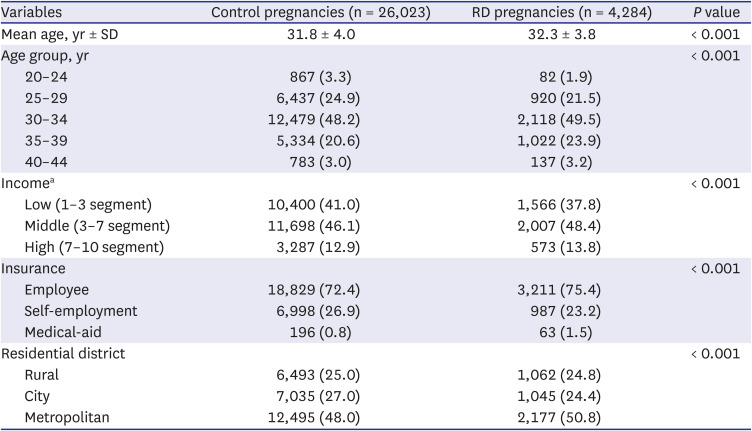
A total of 41,547 women with RD and 208,941 controls both of childbearing age were identified. The RD group included 3,527 women who had 4,284 cases of pregnancies ending in delivery during the study period. In the control group, 20,592 women had 26,023 cases of pregnancies ending in delivery. The demographic characteristics of subjects in the RD and control groups at the time of delivery are summarized in Table 1. The mean maternal age at the time of delivery among RD pregnancies was 32.3 ± 3.8 years, which was slightly higher than that of 31.8 ± 4.0 years in the control group (P < 0.001). More women in the RD group than in the control group had a low-income level, were dependent on medical-aid, and resided in a metropolitan area at the time of delivery.
Table 1
Baseline characteristics of the study population
Delivery method
C-section was performed more often in the RD pregnancies than in control pregnancies (46.69% vs. 36.3%, P < 0.001). The C-section rate was the highest among women with SLE (50.5%), followed by those with AS (48.4%) and SPRA (41.8%); these rates were all significantly higher than those in the control group (P < 0.001). RD pregnancies were more likely to result in C-section delivery than control pregnancies with an OR of 1.5 (95% CI, 1.4–1.6). Among RD pregnancies, the ORs for C-section were 1.8 (95% CI, 1.6–1.9) in SLE pregnancies, 1.7 (95% CI, 1.5–2.0) in AS pregnancies, and 1.2 (95% CI, 1.1–1.3) in SPRA pregnancies (Table 2).
Table 2
Cesarean section rates in RD pregnancies

Pregnancy complications
Most of the measured pregnancy complications occurred significantly more often in RD pregnancies than in the control group (P < 0.001), with the exception of UTI. Likewise, in RD pregnancies, there was a 1.4–4.4-fold increased odds of developing pregnancy complications including TA, PB, PE/E, and IGR. The ORs for pregnancy complications were 1.4 (95% CI, 1.2–1.5) for TA, 2.4 (95% CI, 1.9–3.2) for PB, 4.4 (95% CI, 3.3–5.9) for PE/E, and 2.4 (95% CI, 2.0–3.1) for IGR. SLE pregnancies were associated with the highest risk of developing pregnancy complications, followed by SPRA pregnancies. However, the risk of pregnancy complications was not increased in AS pregnancies. SLE pregnancies were associated with increased risk of TA (OR, 1.6; 95% CI, 1.4–1.9), PB (OR, 3.8; 95% CI, 2.7–5.3), PE/E (OR, 8.9; 95% CI, 6.5–12.2) and IGR (OR, 3.3; 95% CI, 2.5–4.4). SPRA pregnancies had increased risks for TA (OR, 1.3; 95% CI, 1.1–1.5) and IGR (OR, 2.0; 95% CI, 1.4–2.8) (Table 3).
Table 3
Risk of pregnancy complications during RD pregnancies

Values are presented as number (%) or odds ratioa (95% confidence interval).
RD include SLE, SPRA, and AS.
RD = rheumatic disease, SLE = systemic lupus erythematosus, SPRA = seropositive rheumatoid arthritis, AS = ankylosing spondylitis, IUG = intrauterine growth retardation.
aAdjusted for age, income, and residential district.
*P < 0.001 compared with controls.
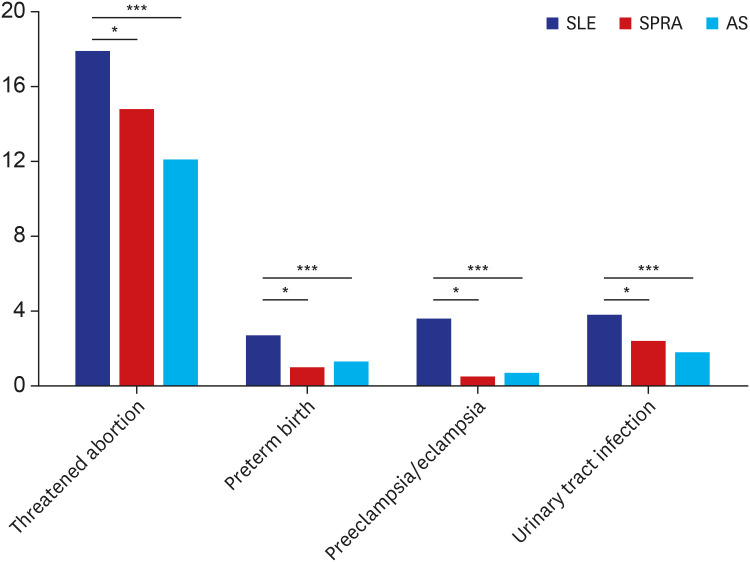
When the prevalence of pregnancy complications was compared among different RD pregnancies, SLE pregnancies had a significantly higher prevalence of all measured pregnancy complications than SPRA and AS pregnancies, with the exception of IGR, which was similar among SLE, SPRA, and AS pregnancies (Fig. 1).
Offspring outcomes
To evaluate the offspring outcomes, the prevalence of LBW offsprings and the offspring death within 1 year of birth were assessed (Table 4). The prevalence of LBW was higher in the offsprings of women with RDs than among controls (3.6% vs. 0.9%, P < 0.001). The prevalence of LBW was 5.9%, 2.4%, and 1.5% in offsprings of women with SLE, SPRA, and AS, respectively; these values were all significantly higher than those of controls (P < 0.001 for SLE and SPRA, P < 0.05 for AS). Offsprings of women with RDs were 4 times more likely to be born with a LBW than those of controls (OR, 4.0; 95% CI, 3.2–4.9). The ORs for LBW were 6.6 (95% CI, 5.2–8.4) and 2.6 (95% CI, 1.8–3.6) in offsprings of women with SLE and SPRA, respectively, and there was no significant increase in the OR for offsprings of women with AS after adjusting for variables. The offspring morality rate within 1 year of birth was higher among women with RDs (6.2/10,000 persons) than among offsprings of controls (4.9/10,000 persons). No cases of death within in 1 year of birth occurred among offsprings of women with SPRA and AS, but two cases of death within 1 year of birth occurred among offsprings of women with SLE. The offspring mortality rate within 1 year of birth among offsprings of women with SLE was 15.1/10,000 persons.
Table 4
Prevalence of low birth weight and the offspring mortality rate within 1 year of birth of women with RDs and controls

RD includes SLE, SPRA, and AS.
Death ≤ 1 year is offspring death within 1 year of birth.
RD = rheumatic disease, LBW = low birth weight, OR = odds ratio, CI = confidence interval, SLE = systemic lupus erythematosus, SPRA = seropositive rheumatoid arthritis, AS = ankylosing spondylitis.
aAdjusted for maternal age, income, and residential district.
*P < 0.001 compared with controls; **P < 0.05 compared with controls.
DISCUSSION
This study demonstrated that women with RDs have an increased risk of developing pregnancy complications, and the risk of LBW offsprings and offspring mortality rate within 1 year of birth is increased among women with RDs. Our study suggests that women with RDs are burdened by their diseases during their childbearing years.
Women with RDs had a 1.5-fold increased risks of C- section delivery and 1.4–4.4-fold increased risk of pregnancy complications including TA, PB, PE/E, and IGR. C-section is generally performed to reduce maternal and perinatal mortalities, and severe maternal and fetal morbidities have been demonstrated to be associated with a threefold increase in risk of C-section delivery.26 It is well documented that pregnancies in women with RDs are high-risk pregnancies. Mothers with SLE must confront PE/E, disease flares, fetal loss, PB, IGR, and neonatal lupus.272829 Pregnancy outcomes in patients with RA have also been shown to be slightly less favorable and have an increased risk of miscarriages and PB.1530 In women with AS, there are controversies regarding the risk of pregnancy complications. Some studies have shown increased risk of PB and small for gestational age,12 but others have reported comparable maternal and fetal outcomes to the general population. We found an increased risk of TA, PB, PE/E, and IGR in SLE pregnancies and increased risk of TA, and IGR in SPRA pregnancies; these findings were comparable to those of previous reports, with some results showing much higher risk (OR of PE/E in SLE pregnancies). The reason for this relatively high OR may be that we excluded chronic disease when selecting patients for the control group, since our criteria was strict to ensure our controls were relatively normal women without risk for pregnancy complications. In AS, we found a comparable risk of pregnancy complications to the control population. In accordance with these increased pregnancy complications, we found an increased rate of C-section in RD pregnancies compared with matched controls (46.7% vs. 36.3%). This rate is also higher than the reported national C-section rate in Korea of 36.9%.31 We found that the risk of C-section delivery was increased in all 3 RDs assessed, and this finding is comparable to those of previous studies.133032 An increased risk of C-section delivery appears to be associated with an increased risk of pregnancy complications in SLE and RA. However, the increased rate of C-section delivery in AS pregnancies found in this study and others appears to be related to factors other than pregnancy morbidities such as dysfunctional labor related to ankylosis of the sacroiliac joints.10 Korean women with RDs have been shown to have a greater burden of comorbidities and medication use during their childbearing years than women without RDs of the same age.33 Maternal comorbidities and concomitant medication may have contributed to increased risks of pregnancy complications.
The most common pregnancy complication was TA; the rate of TA was significantly higher in SPRA and SLE pregnancies than in control pregnancies. Similar to the findings of a previous study from Norway utilizing the Medical Birth Registry,34 this finding indicates that miscarriages are more common in patients with RA and SLE. When pregnancy complications were compared among different RDs, the prevalence of complications was overwhelmingly high during SLE pregnancies. TA, PE, PE/E, and UTI were more frequent in SLE pregnancies than SPRA and AS pregnancies. However, the prevalence of IGR was found to be similar among SLE, SPRA, and AS pregnancies. The increased prevalence of pregnancy complications in SLE compared with RA and AS could be associated with increased use of corticosteroids and immunosuppressive drugs and increased flares during SLE pregnancies.293536
In addition to the increased risk of pregnancy complications in women with RDs, we also found an increased risk of adverse neonatal outcomes in the offsprings of women with RDs. The offsprings of women with RDs were 4 times more likely to be born with LBW than the offsprings of controls. The odds ratio of LBW offsprings was increased in SLE and SPRA pregnancies, but not in AS Pregnancies. The increased risk of LBW offsprings found in this study is in accordance with the findings of previous studies.151630 In a meta-analysis, the relative ratio of LBW < 2,500 g was 4.4 in the SLE group.32 In a study by Bowden et al.37, babies born to women with RA or other inflammatory polyarthritis had a significantly lower mean birth weight than controls. Although the pathogenesis of LBW in offsprings of women with RDs is unclear, high disease activity, drugs used to treat the disease, and abnormal immune responses during RD pregnancies such as placental insufficiency and PE/E have been reported to be associated with LBW in newborns of patients with RDs.38394041424344 The risk of LBW was highest in offsprings of patients with SLE with an OR of 5.9, followed by patients with SPRA (OR, 2.4). In women with AS, the risk of LBW offsprings was not increased compared with controls. This finding was in accordance with those of previous studies.3245 A noteworthy finding of this study is that the offspring mortality rate within 1 year of birth was higher among women with RDs than among controls. Very few population-based studies have followed up the offsprings for more than few months after birth in women with RD. The offspring mortality rate within 1 year of birth of women with RD was 6.2/10,000 persons, whereas 4.9/10,000 persons in controls. Two cases of death occurred in offsprings of women with SLE within 1 year of birth, but no cases of death occurred in offsprings of women with SPRA and AS during the same period. The offspring mortality rate within 1 year of birth of women with SLE was 15.1/10,000 persons. In both cases of which offspring death occurred, mothers were diagnosed with SLE 6–8 months before becoming pregnant, and did not take HCQ before or during pregnancy. HCQ is recommended preconception and throughout pregnancy for patients with SLE since many studies have supported a beneficial role of HCQ in controlling disease activity, preventing flares, and reducing the frequency of PE and prevents fetal growth restriction and prematurity in the fetus.46474849 Our findings suggest a need for educational efforts to improve drug adherence during pregnancy.
This is the largest population-based study evaluating pregnancy complications and offspring outcomes in Korean women with RD. The advantage of this study is that data of almost all RD from the entire country is included, thus, selection bias is small. In addition, although we identified RD cases based on ICD-10 codes, discrepancy between the coding and the classification criteria is minimal since, accurate coding based on fulfillment of classification criteria is required to receive copayment benefits through ICBP in Korea. However, this study has some limitations. First, due to the limitations of information included in NHIS-NHID, it was not possible to ascertain the condition of offspring at birth or maternal disease activity. Second, except for income, insurance, and residential district, other social factors that can affect outcomes—such as the level of education—were not included in the NHIS-NHID, so they were not adjusted for in this study. Third, offspring death occurring within 1 month of birth may have been underestimated. Fourth, since we did not adjust for confounding variables such as multiparity, comorbidities, and co-medications, this may have influenced the obstetric outcomes. To assign a health insurance number for a newborn, a birth must be registered within 1 month of birth. Parents may not have registered the birth, if the offspring passed away shortly after birth. Fifth, ~25% of cases were lost in the process of matching mother with the offspring. If offsprings had medical insurance separate from the mother, these cases could not be matched.
In conclusion, women with RD have a higher risk of pregnancy complications and adverse offspring outcomes. These adversities can significantly influence childbearing and family life of women with RD. Therefore, meticulous monitoring and social support should be made available through various systems.
 XML Download
XML Download