

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The fundamental step in establishing and implementing national policies for individuals with autism spectrum disorder (ASD) is to identify the current prevalence and mortality of ASD.12345 The information on the prevalence and mortality of ASD among children enables policymakers to estimate the socioeconomic burden of the disease. In addition, this information is also useful for international comparisons.
The prevalence rate of ASD has been consistently increasing around the world. For example, in the United States, 1 in 54 children aged 8 years had a diagnosis of ASD in 2016, a statistic which is 2.03 times (1 in 110 children) higher than the estimates in 2006.67 In Korea, previous studies reported that the prevalence of ASD was estimated to be 2.64% (1 in 38 children) among school-aged children, that being 7- to 12-year-olds, 18.53 cases per 100,000 persons when looking at all age groups.8910 However, studies on the age-specific prevalence of ASD are limited in Korea; in particular, no study has investigated the time trends of ASD prevalence over the last 10 years.
Therefore, the aim of this study was to establish annual birth cohorts that include all infants born from 2002 to 2012 and calculate the prevalence and premature mortality statistics of ASD according to birth year using the National Health Insurance Service database.
Go to : 
METHODS
Data sources
We customized and used the National Health Insurance Database to test the study hypothesis. The National Health Insurance Database is managed by the National Health Insurance Service in Korea. Since universal health coverage was implemented in 1989, all citizens residing in the Republic of Korea, except for the vulnerable class, are obligated to subscribe to the national health insurance. As of April 2020, 97.2% of all citizens residing in the Republic of Korea are subscribed to the mandatory national health insurance; the remaining people are beneficiaries of the Medical Aid program funded by the government. Healthcare services provided through Medical Aid are also reimbursed by the National Health Insurance Service. Thus, theoretically, the National Health Insurance Service has the healthcare service data of all citizens of the Republic of Korea.11 We extracted information regarding sex, age, and subscription type (health insurance/Medical Aid) from the National Health Insurance Service qualification database and information regarding ASD from the detailed healthcare service database. Access to these databases was given through the Big Data Utilization Specialist Program of the National Health Insurance Service.
Study design and population
We conducted a population-based retrospective birth cohort study. ASD was defined as the inclusion of ICD-10 codes F84.0, F84.1, F84.5, F84.8, or F84.9 as the main diagnosis or additional diagnosis in the healthcare service databank of the National Health Insurance Database.51213 To estimate the 8-year prevalence of ASD, we established birth cohorts of children born from 2002 to 2012. The total and sex-specific (male/female) numbers of ASD development every year were calculated until children became 8 years of age (e.g., children born in 2002 were followed up until 2010 and children born in 2012 until 2020, etc.).
To analyze the risk for premature mortality among children diagnosed with ASD, we established three new birth cohorts: 1) a birth cohort comprising children born between 2002 and 2012 and followed until 8 years of age (2010–2020) (e.g., children born in 2002 were followed up until 2010 and children born in 2012 until 2020, etc.), 2) a birth cohort comprising children born between 2002 and 2003 and followed until 8 years of age (2010–2011), and 3) a birth cohort comprising children born between 2011 and 2012 and followed until 8 years of age (2019–2020).
We estimated 8-year ASD prevalence and mortality, considering the average age at ASD diagnosis previously reported.14 Data on death and date of death were obtained from the mortality data in the National Health Insurance Database qualification databank.
Statistical analysis
The 8-year ASD prevalence (per 1,000 births) was calculated as the number of ASD cases detected until 8 years of age in children born each year, divided by the number of total birth in the corresponding year (e.g., the 8-year ASD prevalence in 2010 was calculated as the number of children diagnosed to ASD until 2010 among those born in 2002, divided by the number of total birth in 2002). Therefore, the 8-year ASD prevalence can be summarized as follows:
Prevalencei = Number of ASD Cases Until Year i Among Children Born in Year (i−8)Number of total births in year (i−8) × 1,000
The risk of premature mortality among ASD patients was estimated using the above-mentioned birth cohorts through Cox proportional hazard models adjusted for sex, household income (high, middle, and low classes based on the health insurance premium quartile), area of residence (Seoul Capital area, which includes Seoul, Incheon, and Gyeonggi Province; other metropolitan areas; and other regions [cities and provinces]), and year of birth.15 The Cox proportional hazard models can be summarized as follows:
h(t) = h0(t)exp(b1Xsex + b2Xhousehold income + b3Xarea of residence + b4Xyear of birth + b5XASD diagnosis
All statistical analyses were performed using SAS Enterprise Guide 7.1. Statistical significance was defined as a two-tailed P value < 0.05.
Ethics statement
The Institutional Review Board (IRB) of Seoul National University Hospital approved the study protocol (approval No. 20180917/07-2018-27/103) and waived the requirement for informed consent because anonymized claims data were used.
Go to :
RESULTS
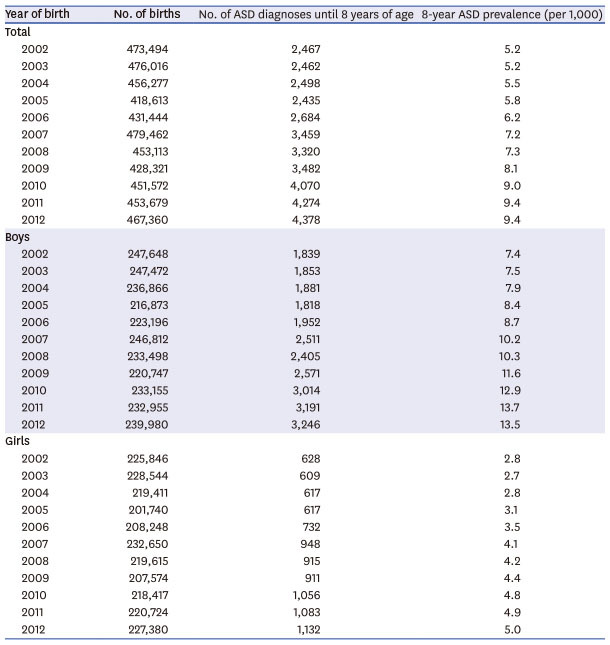
A total of 4,989,351 children born from 2002 to 2012 were enrolled in this study. Of these, 35,529 were diagnosed with ASD until 8 years of age. Among children born in 2002, 2,467 out of 473,494 children (5.2 per 1,000 births) were diagnosed with ASD, and 8-year ASD prevalence was 2.6 times higher among boys (1,839; 7.4 per 1,000 boy births) than among girls (628; 2.8 per 1,000 girl births). Among children born in 2012, 4,378 out of 467,360 children (9.4 per 1,000 births) were diagnosed with ASD, and 8-year ASD prevalence was 2.7 times higher among boys (3,246; 13.5 per 1,000 boy births) than among girls (1,132; 5.0 per 1,000 girl births) (Table 1).
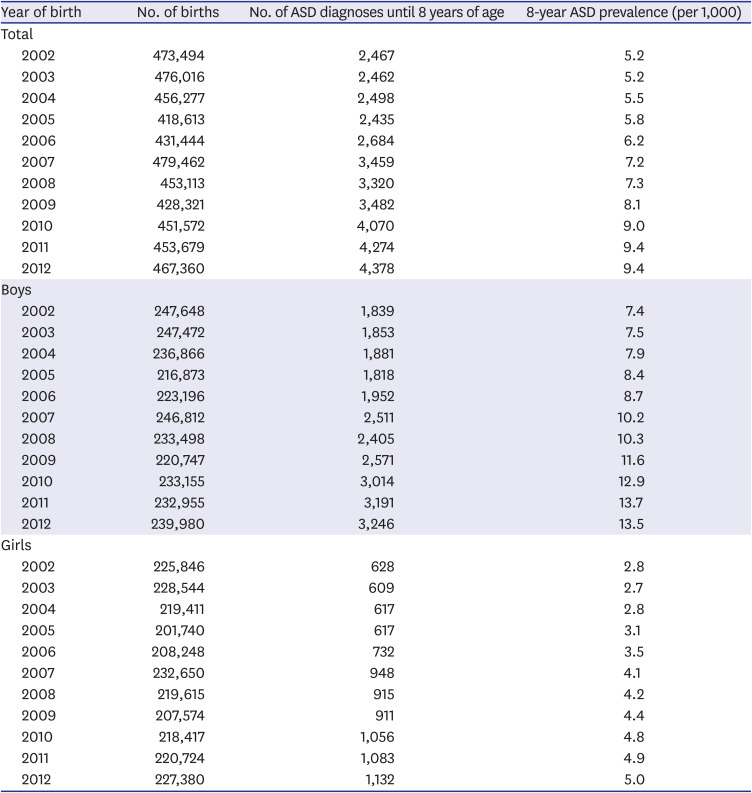
Table 1
8-year prevalence of ASD among children born from 2002 to 2012
![]()
Table 2 shows the ASD cases newly diagnosed in each birth year. For most groups of children born in each year, the number of newly diagnosed ASD cases spiked at age 3 or 4 and substantially decreased after age 8 or 9.
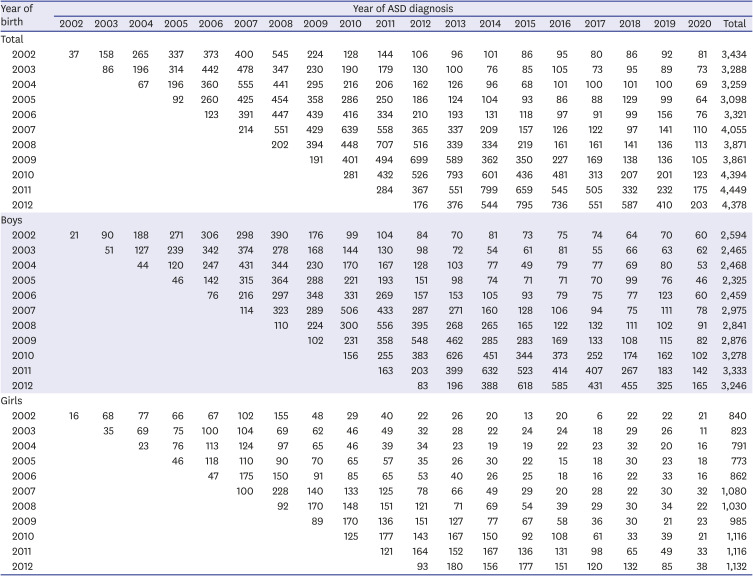
Table 2
Total number of ASD newly diagnosed from 2002 to 2012
![]()
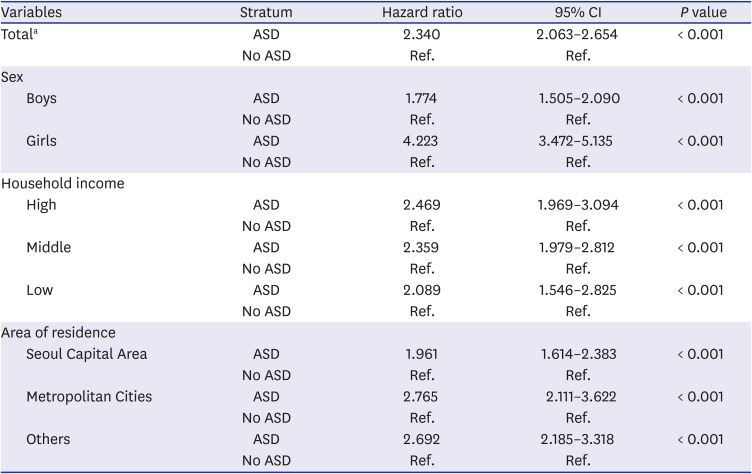
Regarding the risk of all-cause mortality among children with ASD (born between 2002 and 2012), the hazard ratio (HR) of death in children diagnosed with ASD was 2.340 (95% confidence interval (CI), 2.063–2.654; P < 0.001) compared to those who were not diagnosed with ASD. In the sex-stratified analyses, the HR for death according to ASD diagnosis was 4.223 (95% CI, 3.472–5.135; P < 0.001) for girls and 1.774 (95% CI, 1.505–2.090; P < 0.001) for boys, indicating that girls are at a higher risk of death from ASD (Table 3, Fig. 1). In analyses stratified by income status, the HR was not only increased in middle (2.359; 95% CI, 1.979–2.812; P < 0.001) and lower-income class (2.089; 95% CI, 1.546–2.825; P < 0.001) but also in the high-income class (2.469; 95% CI, 1.969–3.094; P < 0.001). Regarding the area of residence, the risk of premature death was higher among those residing outside the Seoul Capital area than those residing in the Seoul Capital area. In particular, the HR of death among people with ASD who were residing in areas in the Seoul Capital area was 1.961 (95% CI, 1.614–2.383; P < 0.001), that of those residing in other metropolitan areas was 2.765 (95% CI, 2.111–3.622; P < 0.001), and that of those residing in other cities and provinces was 2.692 (95% CI, 2.185–3.318; P < 0.001) (Table 3). Meanwhile, the HRs of all-cause premature mortality were 1.982 (95% CI, 1.414–2.781; P < 0.001) among children with ASD born between 2002 and 2003, and 2.391 (95% CI, 1.497–3.819; P < 0.001) among children with ASD born between 2011 and 2012.
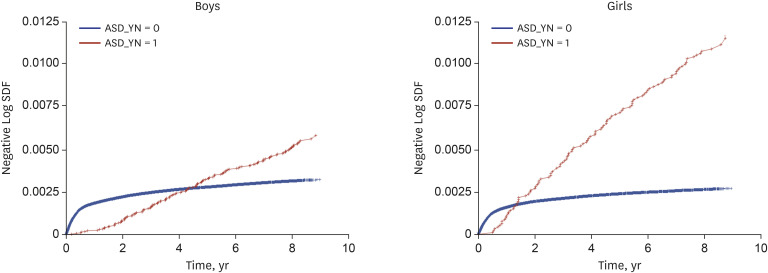 | Fig. 1Risk of all-cause mortality in children with autism spectrum disorder stratified by sex.Associations were assessed using Cox regression models adjusted for household income, area of residence, and birth year.
ASD = autism spectrum disorder.
|
Table 3
Risk of all-cause mortality in children with ASD compared with children without ASD, stratified by sex, household income, and area of residence
ASD = autism spectrum disorder, CI = confidence interval, Ref. = reference.
aCox proportional hazard models adjusted for sex, income, area of residence, and year of birth.
![]()
Go to :
DISCUSSION
Prior to devising policies pertaining to individuals with ASD, policymakers need to ascertain the number of people affected by the disorder and the number of people who would die due to the disorder.145 To date, corresponding information on ASD in the Republic of Korea has not been properly studied. Therefore, we followed up on all newborns and estimated the prevalence and mortality of ASD among children at 8 years of age.
In this study, we established birth cohorts of children born from 2002 to 2012 using nationwide population-based claims data in the Republic of Korea, analyzed newly diagnosed ASD cases according to birth year, and assessed the trend of diagnosis according to age for each cohort. The results showed that the number of newly diagnosed ASD cases spiked at age 3 or 4 and substantially decreased after age 8 or 9. This phenomenon was evident in both boys and girls. The present study also showed that the risk for premature death from ASD was higher among girls, the high-income class, and people residing in regions outside the Seoul capital area than among boys, the low-income class, and people residing in other regions, respectively.
Although the prevalence of ASD varies by country, it is on the rise overall.61617 An increased prevalence means that there is an increased number of newly diagnosed cases if the mortality rate is consistent. The United States established the Autism and Developmental Disabilities Monitoring Network in 2000. The network analyzes the trends of ASD prevalence among 8-year-olds every 2 years.6 According to their data, the prevalence of ASD among 8-year-olds rose from 14.5 cases per 1,000 children (1 in 69 children) in 2012 to 18.5 cases per 1,000 children (1 in 54 children) in 2016.618 According to Canada’s National Autism Surveillance System, the prevalence of ASD among children aged 8 years old in Canada was 15.9 cases per 1,000 children in 2015; 28% of the children were diagnosed with ASD at or after the age of 8.19 In Sweden, the cumulative incidence of ASD is estimated to be 12 cases per 1,000 children among children aged 8 years old.20
In contrast, there is no nationwide data on the prevalence of ASD in the Republic of Korea, and the disorder is not continuously monitored.121 The prevalence of ASD among children in the Republic of Korea has been estimated based on regional epidemiology study results, as opposed to using nationwide data. The epidemiology study calculated the prevalence of ASD among elementary school children (7–12 years) to be 2.64% using an epidemiological tool. One noteworthy factor is that two-thirds of the patients with ASD, as identified using the epidemiological tool, had not been diagnosed by a physician prior to the survey.8 Even if nationwide population-based claims data, such as those used in the present study, were used in that study, the prevalence was calculated for all patients with ASD in a particular year; thus, it was difficult to identify the number of ASD diagnoses according to age.9 Thus, the present study is significant in that it is the first study to identify the annual nationwide prevalence of ASD according to age.
In a US surveillance monitoring study, the median age at ASD diagnosis among children aged 8 years old was reported to be 4.25 years.6 Among children aged 4 years old, the median age at diagnosis was 33 months, which is similar to our findings.22 As the rate of ASD diagnosis before age 4 increased from 58% in 2014 to 71% in 2018, there has been a growing emphasis on the importance and awareness of early ASD diagnosis.2223 In a nationwide study conducted in Canada, the ASD diagnosis rate was 33% among children up to age 3 and 72% among children up to age 7, indicating a lower early diagnosis rate than the US.19
The prevalence of ASD among children aged 8 years and older, the stage at which the rate of increase in diagnosis diminishes, was 5.2–9.4 cases per 1,000 population, which is lower than that reported in foreign studies and that estimated in the Republic of Korea using an epidemiological tool.681920 Previous epidemiological studies reported that two-thirds of children diagnosed with ASD using an epidemiological tool had not been diagnosed by a physician, shedding light on the reality of under-diagnosis of ASD and the consequent lack of treatment in the Republic of Korea.821 Although a previous large-scale study reported a 4–5 times higher prevalence of ASD in males than in females, the male-to-female prevalence ratio among children aged 8 years in the present study was relatively low at 2.45–2.82.61419
Our analysis showed that the risk of mortality was substantially higher among preschool-aged children with ASD than among their counterparts without ASD. In particular, the risk of premature mortality was markedly higher among girls than among boys, a finding which aligns with the findings of previous studies.1224252627 ASD is not a direct and sole cause of death. One of the hypotheses concerning the higher mortality rate associated with ASD is related to the comorbid conditions of ASD or intentional or unintentional injury.15242728 Since we analyzed all-cause mortality in this study, additional studies that include the analysis of the major comorbidities of ASD and the cause of death are needed.
When we stratified the risk of mortality from ASD according to income level, the risk of mortality was increased not only in the middle/low-income class but also in the high-income class. Previous studies reported that the rate of early ASD diagnosis and prevalence were higher in families with higher socioeconomic status, whereas delayed diagnosis and inadequate treatment in low-income families affected prognosis.293031 Thus, further studies, especially those with information regarding the cause of death, should be conducted to analyze the association between the risk of premature mortality and family income and the reason for the gap between income levels using nationwide data.
Our analysis of the association between the risk of all-cause mortality and ASD diagnosis according to the area of the residence revealed that there are regional gaps in the risk of premature mortality from ASD. In particular, the risk of premature mortality was highest among those residing in other metropolitan cities, followed by other cities and provinces and the Seoul capital area. A previous study that analyzed the utilization of healthcare by individuals with ASD in the Republic of Korea reported that these individuals utilized 36% of the healthcare facilities in Seoul and 22% of the healthcare facilities in Gyeonggi Province as of 2017.5 Although more than half of the healthcare facilities utilized are located in the Seoul capital area, the findings of the present study indicate that the risk of premature mortality from ASD is substantially higher among people residing in regions outside the Seoul capital area. This may be attributable to differences in the supply of and access to healthcare services needed for ASD across regions or a low rate of diagnosis of ASD in regions outside the Seoul capital area. Therefore, further research is needed to estimate the prevalence of ASD according to region.
In the Republic of Korea, three types of databases, namely the disability registry, the current state of individuals with disabilities, and National Health Insurance Scheme data, are used to estimate the number of individuals with developmental disabilities, including ASD. The government relies on the disability registry database to develop policies. Thus, individuals must register their disability to reap the benefits of these policies. However, there is a risk that the number of people with ASD is underestimated in the disability registry due to issues such as stigma.1432 The National Health Insurance claims data provide information on everyone in the Republic of Korea who received care for ASD. However, it is possible that the actual social burden due to ASD may be overestimated. An analysis of the 2017 health insurance claims data showed that healthcare utilization was remarkably diminished among people in their 30s and older and was virtually absent among people in their 40s and older.15 Therefore, cohorts need to be established and analyzed by linking the disability registry data and health insurance claims data to comprehensively determine the actual epidemiological features and social burden from ASD.145
Prior to this study, there has been virtually no attempt to estimate the nationwide prevalence of ASD—the most fundamental factors that need to be considered when developing and implementing relevant national policies—in the Republic of Korea. The present study confirmed that the increase in the prevalence of ASD in the Republic of Korea levels out from age 8. The current prevalence of ASD among children aged 8 years old was about 9.4 cases per 1,000 births and that the prevalence was about 2.7 times higher in boys than in girls. In addition, the risk of premature mortality was higher among children diagnosed with ASD and among girls with ASD than among boys with ASD. The significance of this study is that it generated foundational nationwide data that can be used in ASD research, policies, and decision-making. More specific studies, including analyses of causes of death, are needed to establish detailed targets and tailored policies and plans.
Go to :
 XML Download
XML Download