

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has been the major concern in most of the world since December 2019, which is being overcome by widespread inoculation with various COVID-19 vaccines. However, concerns about the safety of the COVID-19 vaccines are still a major hurdle to widespread vaccination due to insufficient safety data. Here, we report the first case of adult-onset Still’s disease (AOSD) in a patient after receiving the BNT162b2 mRNA COVID-19 vaccine (Pfizer, New York, NY, USA).
Go to : 
CASE DESCRIPTION
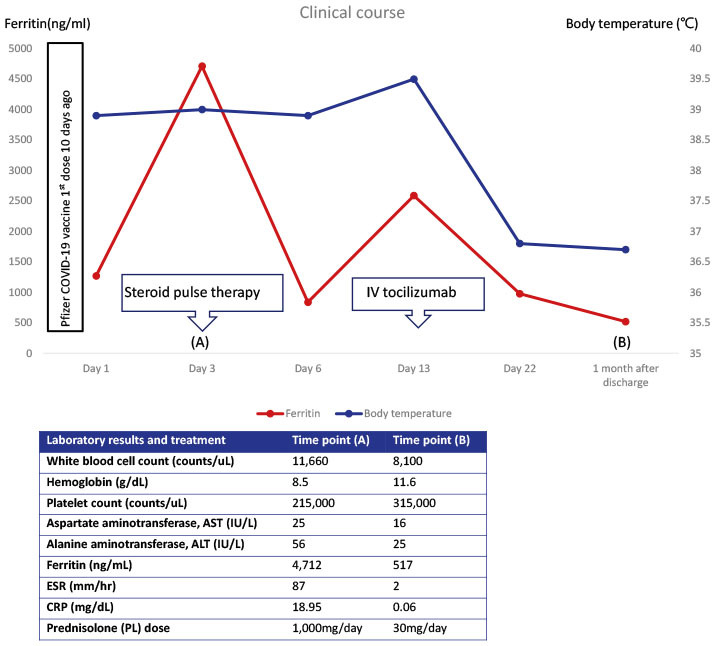
A 36-year-old, previously healthy woman developed high spiking fever, chilling sense and sore throat 10 days after the first dose of the BNT162b2 mRNA COVID-19 vaccine (Pfizer). She visited a primary clinic and took oral antibiotics for 3–4 days, but the symptoms persisted, and she was admitted to our hospital for evaluation of high fever. At baseline, she was febrile with a body temperature of 38.9°C, blood pressure 100/70 mmHg, pulse rate 100/minute and respiration rate 20/min. She had sore throat and multiple joint pain including hands and ankles. On physical examination, mild pharyngeal injection was noted with diffuse edema on both hands and feet. Computed tomography (CT) of the neck, chest, abdomen and pelvis revealed splenomegaly (12.3 cm) and several mildly enlarged lymph nodes in the paraaortic and aortocaval spaces. Laboratory test showed white blood cell count 12,220/mm3, erythrocyte sedimentation rate 56 mm/hr, C-reactive protein 16.28 mg/dL, and ferritin 1,268 ng/mL. Rheumatoid factor (RF) and antinuclear antibody (ANA) were negative. Thorough investigations for infections including blood and urine cultures, malaria antigen test, leptospira antibody test, Hantaan virus antibody test, Orientia tsutsugamushi antibody test, and COVID-19 polymerase chain reaction test revealed no significant results. The daily high spiking fever reaching 39°C continued until hospital day 3, when she developed salmon pink colored, maculopapular rash on the trunk (Fig. 1A) as well as dyspnea that required oxygen supplementation. Follow-up chest radiograph and CT scan revealed newly developed bilateral pleural effusion and pericardial effusion (Fig. 1B and C) and the ferritin level rose from 1,268 ng/mL to 4,712 ng/mL. Based on the classification criteria for AOSD,1 she was diagnosed with AOSD (fever, arthralgia, leukocytosis, sore throat, lymphadenopathy, splenomegaly, negative RF and ANA). Steroid pulse therapy (methylprednisolone 1,000 mg for 3 days) was tried initially, but only led to a brief resolution of fever. Then, we tried intravenous tocilizumab (8 mg/kg), which dramatically improved all the symptoms and laboratory abnormalities. She was discharged and is currently in good condition and the bilateral pleural effusion and cardiomegaly disappeared (Fig. 1D) 1 month after discharge.
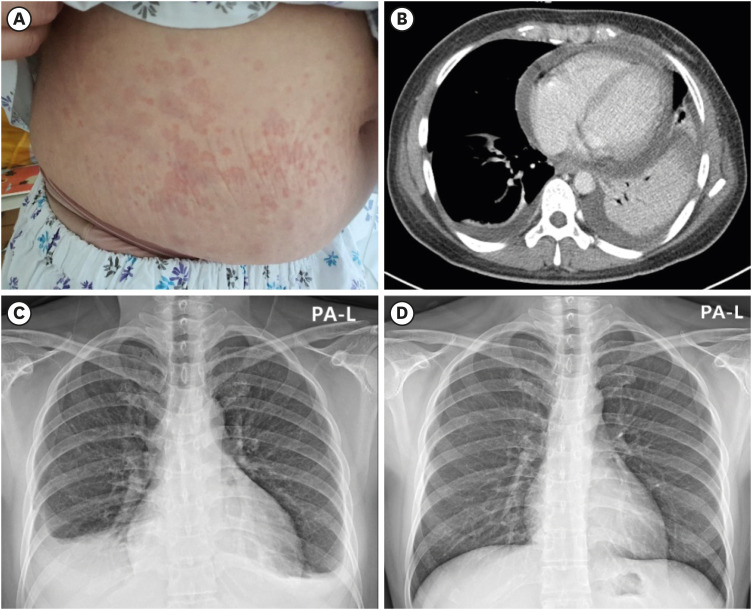 | Fig. 1Photograph (A), CT scan of the chest (B), and serial chest radographs (C, D) of this case.(A) Salmon colored, maculopapular rash is noted on the trunk. (B) Chest CT scan taken on hospital day 3 reveals bilateral pleural effusion and pericardial effusion. (C) Chest radiograph taken on hospital day 3 shows bilateral pleural effusion and cardiomegaly, (D) Chest radiograph taken 1 month after discharge reveals improvement of bilateral pleural effusion and cardiomegaly.
CT = computed tomography.
|
Ethics statement
The authors obtained approval from the Institutional Review Board (IRB) of Dongguk University Ilsan Hospital (IRB number 2021-11-012). Informed consent for data collection and publication of the study was obtained from the patient.
Go to :
DISCUSSION
To the best of our knowledge, this is the first reported case of AOSD occurring after receiving BNT162b2 mRNA COVID-19 vaccine. A case of flare-up of underlying AOSD after receiving the same vaccine was reported,2 but it dealt with a patient with an established disease of AOSD. There have also been reports of AOSD occurring after COVID-193 as well as COVID 19 vaccination,45 but the vaccines documented in the two reported cases of AOSD after COVID-19 vaccination were mRNA-1273 and ChAdOx1 nCov-19 vaccine.
AOSD is a rare autoinflammatory disorder characterized by high spiking fever, rash, arthralgia or arthritis and multiple organ involvement. Although the exact pathogenic mechanism of AOSD is not fully understood, innate immune system activation, rather than adaptive immunity, is implicated in the pathogenesis of AOSD.6 Danger signals such as pathogen-associated molecular patterns or damage associated molecular patterns are transmitted to macrophages and neutrophils via Toll-like receptors (TLR) leading to overproduction of interleukin (IL)-1β, which ultimately results in intense innate immune cell activation and overproduction of several proinflammatory cytokines, called ‘cytokine storm’.
Similar to AOSD, most of the morbidity and mortality due to COVID-19 results from the ‘cytokine storm’ characterized by overproduction of proinflammatory cytokines due to intense activation of the innate immune system. Once severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) enters the host immune cell, the genomic ssRNAs and replicative dsRNA intermediates are recognized by cytosolic receptors including TLR 3,7,8 and ultimately activate the downstream inflammatory pathways via transcriptional factors such as nuclear factor kappa B and interferon regulatory factors 3/7, which leads to overproduction of proinflammatory cytokines and hyperinflammation.7 Accordingly, AOSD was reported to occur after COVID-19.3
The occurrence of AOSD after BNT162b2 mRNA COVID-19 vaccination in this report could be a rare coincidence. However, there also are possible explanations and evidence for the relation between the two events. First, there is a close temporal relationship in this case. A substantial increase in humoral response against SARS-CoV-2 spike protein was noted 14 days after the first vaccine dose.8 There have also been many reports of AOSD occurring after receiving various vaccines including influenza, pneumococcal, hepatitis A and hepatitis B vaccine.91011 Secondly, there is a possibility that the SARS-CoV-2 spike proteins induced by the vaccine might trigger the innate immune hyperactivation. SARS-CoV-2 spike proteins are also known to activate the immune system in COVID-19.7 Lastly, anti-IL-6 treatment was effective in this patient. IL-6 has been reported to have a pathogenic role both in AOSD and COVID-19 infection.67 Moreover, anti-IL-6 treatment has been shown to be effective in lowering the mortality of severe COVID-19 infection12 like in the case of AOSD,13 though the former needs to be clarified with high quality data in the future.
Go to :
 XML Download
XML Download