

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Occupational stress is an important health issue closely related to mental health.12 High occupational stress can influence emotional disorders such as depression and anxiety3 as well as cognitive functions such as attention and working memory.4 Firefighters often encounter highly stressful dangerous situations in their work environment. Previous studies identified a close relationship between job stress and mental health issues, such as depression, alcohol use, and sleep quality, in firefighters.56 Therefore, there is much interest in identifying and managing occupational stress of firefighters.
High stress levels are associated with structural changes in regions of the brain.78 Cumulative adversity and stress are associated with gray matter volume (GMV) in the medial prefrontal, anterior cingulate, and insular regions.9 Neuroanatomic differences in several brain regions, such as basal ganglia, cingulate cortex, and hippocampus are related to stress vulnerability and resilience.10 Taken together, these findings suggest that the close association between stress and mental health is mediated by properties of brain structures. Several previous studies analyzed the relationship between occupational stress and gray matter characteristics. A magnetic resonance imaging (MRI) study demonstrated that highly stressed subjects had reduced cortical thickness in the mesial frontal cortex, low GMV in the caudate, and high GMV in the amygdala.11 Another MRI study showed that highly stressed subjects had low GMV in the anterior cingulate cortex (ACC), the dorsolateral prefrontal cortex, the caudate, and the putamen.12
This study evaluated the occupational stress of firefighters and analyzed the relationship between their occupational stress and regional GMV properties. We assessed job stress, categorized firefighters into highly and lowly stressed groups, and compared GMVs between the two groups. Initially, we conducted whole-brain voxel-based morphometry (VBM) to investigate brain regions that have regional GMV differences between highly and lowly stressed groups. Then, we selected brain regions based on VBM results and calculated GMVs at manually delineated region of interest (ROI) to compare groups. We also evaluated correlations between clinical variables and GMV values.
Go to : 
METHODS
Participants
We recruited 1,022 participants from the Firefighter Research on Enhancement of Safety & Health (FRESH) cohort,13 including firefighters and rescue workers, assessed at three university hospitals between 2016 and 2017: Severance Hospital recruited firefighters from Seoul, Gyeonggi, Chungcheongnam-do, Daejeon, and Jeollabuk-do regions; Wonju Severance Christian Hospital recruited firefighters from Gangwon and Chungcheongbuk-do regions; and Gyeongsang National University Hospital recruited firefighters from Gyeongsangbuk-do, Gyeongsangnam-do, and Jeollanam-do regions. To assess psychological characteristics, we conducted several self-reporting questionnaire. All participants completed the Korean version of the posttraumatic diagnostic scale (PDS) for post-traumatic stress disorder (PTSD) symptoms.14 We administered the Center for Epidemiologic Studies Depression Scale (CES-D) to assess depressive symptoms,15 the Beck Anxiety Inventory (BAI) to assess anxiety symptoms,16 the Alcohol Use Disorders Identification Test (AUDIT) to assess alcohol-related symptoms,17 and the Pittsburgh Sleep Quality Index (PSQI) to assess sleep difficulty.18 Among these participants, 352 participants (aged > 40 years or new hires with less than 1 year of service) were included in neuroimaging sub-study who underwent 3-Tesla (3T) brain MRI to investigate structural changes in the brain.
Additionally, we assessed occupational stress using the short form of the Korean Occupational Stress Scale-26 (KOSS-26).19 The KOSS-26 was conducted through a web-based survey “Job Contents And Health Survey of Firefighters.” The scale comprises 26 items across 8 categories: physical environment, job demand, insufficient job control, interpersonal conflict, job insecurity, organizational system, lack of reward, and occupational climate. Briefly, each item is rated on a 4-point Likert scale, with higher scores indicating higher occupational stress. The score for each category is then converted to a value between 0 to 100 points. The total KOSS-26 score is calculated by averaging the scores of the categories. In our study, each of the 121 subjects (117 males and 4 females) completed both a brain MRI and KOSS-26 questionnaire. We excluded participants with severe depression and anxiety (cutoff: CES-D 23 points, BAI 25 points) from the study based on their answers to the psychological questionnaires. As a result, 115 subjects (112 males and 3 females) were included in the study. To obtain a possible number of samples per group with a model power of 0.8 or greater in group differences (t-test or analysis of variance) and relationship (correlation or regression) measures, we divided all subjects into two groups and compared them.2021 The median value of the KOSS-26 score of 115 firefighters and rescue workers was 44.8. The Cronbach's α value for KOSS-26 was 0.878. We classified participants into the highly stressed group (n = 58) or lowly stressed group (n = 57) based on whether they scored above or below the median value.
Brain MRI preprocessing
We conducted brain MRIs using a 32-channel 3T MRI scanner (Achieva; Philips Healthcare, Best, the Netherlands or Ingenia CX; Philips Healthcare). A 3D T1-turbo field echo sequence was obtained according to the following parameters: repetition time = 9.9 ms, echo time = 4.6 ms, fiel of view = 220 × 220 mm2, section gap = 0 mm, voxel size = 0.859 × 0.859 × 1.0 mm3, flip angle = 15°, total acquisition time = 5 minutes 29 seconds. All three institutions participating in this study acquired MRI data using the same protocol. We analyzed brain images using MATLAB 8.5 (MathWorks, Natick, MA, USA) and SPM12 (Wellcome Department of Imaging Neuroscience, London, UK). With the same protocol described in our previous VBM study for firefighters,22 standardized diffeomorphic anatomical registration with an exponentiated Lie algebra algorithm (DARTEL) preprocessing steps for VBM was performed.23
After VBM analysis, we performed an ROI-wise surface-based morphometry (SBM) analysis by setting the brain regions where the group difference was significant in the VBM as the ROIs. The FreeSurfer 6.0 (http://surfer.nmr.mgh.harvard.edu/) was utilized for SBM analysis. The preprocessing steps included skull stripping using a hybrid approach,24 correction of intensity non-uniformity,25 segmentation and surface reconstruction,26 topology-correction of cortical surfaces using non-separating loops,27 surface inflation and flattening,28 and automatically parcellating the human cerebral cortex.29 Afterwards, we extracted mean values of GMV within each ROI. ROIs were derived from the Desikan-Killiany cortical atlas.30
Statistical analysis
We performed statistical analyses for demographic and clinical characteristics using the Statistical Package for the Social Sciences (SPSS) version 24.0 (SPSS Inc., Chicago, IL, USA), and designated P value <0.05 to be statistically significant. To compare demographic data (clinical characteristics of highly and lowly stressed groups), we used independent t-tests and χ2 tests.
We explored for the region with GMV differences using VBM analysis of the whole brain. To find group differences in GMV, we used an analysis of covariance model at each voxel. Age, sex, and intracranial volume (ICV) of each subject were chosen as covariates because of their known impacts on gray matter properties.31 ICV was calculated for each subject by summing the gray matter, white matter and cerebrospinal fluid volumes. Statistical inferences were set at P < 0.005 uncorrected and an extent threshold of 10 contiguous voxels. Albeit a relatively liberal threshold, this threshold has often been applied in exploratory whole-brain VBM studies.3233 In the ROI-wise SBM analysis, group differences were assessed by using an analysis of covariance for the extracted GMV value of each ROI. Age, sex, and ICV of each subject were entered as covariates.
To assess brain-behavior relationships, we performed a partial correlation analysis for GMV, KOSS-26 scores, and the length of services. We extracted mean GMV of clusters with group differences using the MarsBaR toolbox (http://marsbar.sourceforge.net/) and considered age, sex, and ICV of each subject as covariates. In subsequent correlation analyses, we added parameters related to comorbid conditions (CES-D, BAI, AUDIT) as covariates.
Ethics statement
The current study's protocols were approved by the Institutional Review Boards of Severance Hospital, Yonsei University Health System in Seoul, Korea (4-2016-0187), Wonju Severance Christian Hospital in Wonju, Korea (CR316014 and CR318335), and Gyeongsang National University Hospital in Jinju, Korea (GNUH 2016-04-015-006). All participants provided informed consent.
Go to :
RESULTS
Demographic and clinical characteristics of study subjects
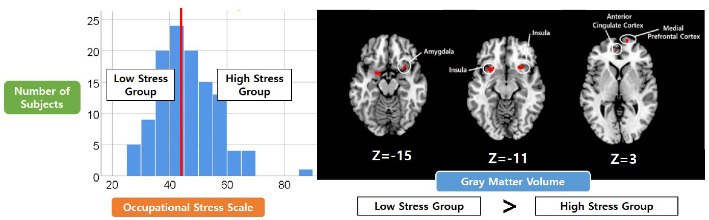
The mean ± standard deviation ages of the two groups classified by occupational stress scores were 49.9 ± 6.5 and 49.2 ± 6.7 years, respectively (Table 1). The highly stressed group scored significantly higher on KOSS-26, PDS, and PSQI measures (KOSS-26: P < 0.001; PDS: P = 0.005; PSQI: P = 0.003). However, highly and lowly stressed groups had no significant difference for CES-D, BAI, and AUDIT scores.
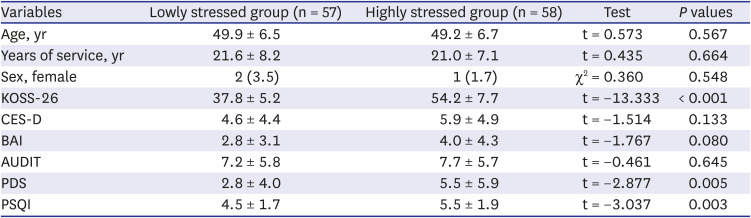
Table 1
Demographic and clinical variables of subjects
Data are shown as mean ± standard deviation or number (%).
KOSS-26 = Korean Occupational Stress Scale-26, CES-D = Center for Epidemiologic Studies Depression Scale, BAI = Beck Anxiety Inventory, AUDIT = alcohol use disorders identification test, PDS = Post-traumatic Diagnostic Scale, PSQI = Pittsburgh Sleep Quality Index.
![]()
Exploratory VBM results
The highly stressed group had lower GMVs than the lowly stressed group on both sides of the insula, the left amygdala, right medial prefrontal cortex (mPFC), and ACC (Table 2, Fig. 1). The highly stressed group had higher GMVs in the right temporal pole than the lowly stressed group.

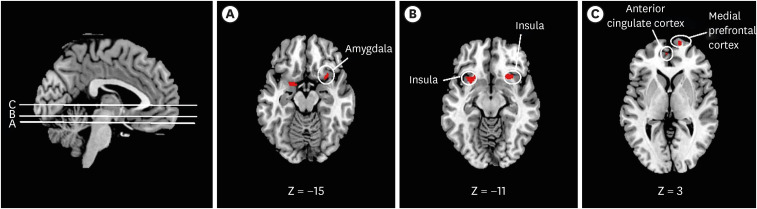 | Fig. 1Brain regions in which voxels had lower gray matter volume in the highly stressed group than the lowly stressed group. Statistical inference thresholds determined by uncorrected P values height threshold of 0.005, with an extent threshold of contiguous 10 voxels. Coordinates indicate locations of brain slices according to the Montreal Neurological Institute system. (A) Amygdala; (B) both sides of insula; (C) medial prefrontal cortex and anterior cingulate cortex.
|
Table 2
Exploratory whole-brain VBM analysis
Brain regions in which voxels had significant group gray matter volume differences between highly and lowly stressed groups (height threshold of uncorrected P values < 0.005, extent threshold of contiguous kE: 10 voxels).
VBM = voxel-based morphometry, kE = number of cluster voxels.
![]()
ROI-based SBM results
Based on results from the VBM analysis, we identified both sides of the insula, the temporal pole, and the amygdala as ROIs. Because clusters of the mPFC and ACC were on the rostral side, we also identified the rostral mPFC and ACC on both sides as ROIs. As a result, the highly stressed group had lower GMVs in both sides of the insula (left insula: P = 0.010; right insula: P = 0.018) and right rostral mPFC (P = 0.008). In other ROIs, we saw no significant difference in GMV between the two groups.
Correlation analysis results
We determined GMV values of the insula and the mPFC for correlation analysis. Within the highly stressed group, low GMV of the insula significantly correlated with length of service (left insula: r = −0.347, P = 0.009; right insula: r = −0.333, P = 0.012; Fig. 2). These correlations remained significant when controlling for other covariates (CES-D, BAI, and AUDIT) (left insula: r = −0.391, P = 0.004; right insula: r = −0.394, P = 0.003). Other correlation analyses were not significant. In particular, within the lowly stressed group, the correlation between GMV of the insula and length of service was not significant (P > 0.05).
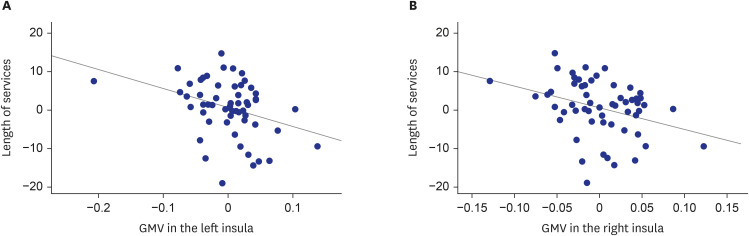 | Fig. 2Correlation analysis of mean GMV values for clusters in the bilateral insula and the length of service for firefighters under high stress (n = 58). To depict partial correlation, we used linear regression to regress variables onto covariates. To generate scatter plots, we used calculated non-standardized residuals. (A) Smaller GMV in the left insula significantly correlated with longer years of service (r = −0.347, P = 0.009). (B) Smaller GMV in the right insula significantly correlated with longer years of service (r = −0.333, P = 0.012).GMV = gray matter volume.
|
Go to :
DISCUSSION
This study identified gray matter abnormalities related to occupational stress in firefighters. In VBM analysis, firefighters with high occupational stress had lower GMVs than those with low occupational stress in both sides of the insula, the left amygdala, right mPFC, and ACC. These results were consistent with previous findings that these brain regions have GMV changes in response to cumulative adversity.9 We confirmed the low GMV of the bilateral insula and right mPFC in the highly stressed group in ROI-based SBM analysis. Within the highly stressed group, lower GMV of the insula significantly correlated with the length of service. By contrast, the highly stressed group had higher GMVs than the lowly stressed group in the right temporal pole. Firefighters in this study had no comorbid psychiatric problems such as depression or anxiety, no history of psychiatric medications, and normal working functions. Our results suggest that regional GMV abnormalities are related to occupational stress.
Both the insula and amygdala are closely associated with emotional regulation. The insula plays a crucial role in body/emotional awareness, and the GMV of the insula is related to emotional regulation.34 The left amygdala is closely related to automatic responses to emotional stimuli.3536 Chronic occupational stress is suggested to affect emotional processing, such as emotion recognition and regulation of emotional stimuli.37 Functional activity and connectivity of brain regions related to emotional processing may be affected by burnout.38 The temporal pole, which had a larger GMV in the highly stressed group, is related to retrieving affective autobiographic memories.39 Considering this information together, it is possible that GMV changes in brain regions, including the insula and the amygdala, mediate difficulties in emotional processing related to occupational stress. In particular, lower GMV of the insula correlated with longer length of service in the highly stressed group, suggesting that changes in the insular gray matter are related to firefighters' accumulated occupational stress.
We found that firefighters under high occupational stress had lower GMV in the ACC and the mPFC. The ACC is a crucial area for self-regulation, and alterations in its function and structure are frequently associated with occupational stress.1238 The rostral part of the ACC and mPFC are closely related to self-referential processing of negative emotional stimuli.40 Brain regions related to self-referential processing are part of the neuro-circuit responsible for resilience to stress.4142 Considering the small size of the brain cluster in this study and that participants did not perform behavioral tasks to evaluate self-referential thinking, additional studies are needed to a draw a more definitive conclusion.
The most interesting finding in this study is that the GMV of the amygdala was lower in the high occupational stress group. This is in contrast to a previous VBM study that reported an association between occupational stress and increased volume of the amygdala.11 Several possibilities can be considered for the reasons for these conflicting findings. First, neurobiological responses to stress on the left and right sides of the amygdala are different, and the relationship between stress and increases in amygdala volume has been suggested to be more prominent on the right side.43 Second, this study targeted firefighters, a group at high risk for PTSD, and research has indicated that reductions in GMV of the amygdala appear in PTSD.44 Brain regions identified in this study were similar to areas of interest in brain imaging studies of PTSD patients.45 While the subjects in our study had never been diagnosed with PTSD or taken psychiatric medications, firefighters are often exposed to stressful situations due to the nature of their occupation, and in this study, the highly stressed group had higher scores for PTSD-related symptoms than the lowly stressed group. Many studies have reported structural and functional brain alterations associated with trauma exposure without PTSD.46 It is important to consider whether our findings reflect the effects of accumulated traumatic exposures during firefighters' duties.
There were some limitations in this study. First, we did not include people suffering from major illnesses, which may have affected grouping criteria. KOSS-26 is a psychometric tool that comprehensively and reliably quantifies occupational stress and has been used in work-related studies of firefighters.4748 However, because KOSS-26 does not assign cut-off values, we classified groups based on the median value of firefighter scores. Second, we conducted this study with a cross-sectional design. Therefore, it is difficult to identify causal relationships between occupational stress and brain imaging results. Third, firefighter duties are varied, and individuals have different experiences. Further analysis that considers specific work-related factors in a larger participant sample would be helpful to understand the effects of stress and resilience on the brain.
In conclusion, we analyzed changes in regional GMV related to occupational stress in firefighters. Firefighters under high stress tended to have had lower GMV than those under low stress in brain regions associated with emotional processing. In particular, low GMV of the insula in firefighters under high stress significantly correlated with the length of service. These findings are important to consider because regional gray matter abnormalities and associated emotional dysregulation may be related to firefighter susceptibility to burnout.
Go to :
 XML Download
XML Download