

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diphtheria, tetanus, and pertussis are community-acquired infectious diseases that can be life-threatening.12 Despite the substantial decline in incidence of diphtheria and tetanus and their near elimination due to immunization in developed countries, these diseases remain endemic in some developing countries with low vaccination coverage. Outbreaks of diphtheria are reported continuously in regions that are predominantly rural or in a state of economic crisis or civil war.3 Tetanus still occurs in African and Asian countries.4 Pertussis outbreaks, on the other hand, occur cyclically worldwide, including in developed countries with high vaccination coverage.256
Vaccination is the most effective strategy to prevent diphtheria, tetanus, and pertussis. Thus, most countries recommend universal childhood vaccination with combination diphtheria-tetanus-pertussis (DTP) vaccines, a primary series of three doses to be completed by 6 months of age and two boosters in the second year of life and at the time of school entry.78 Regarding booster dosage during adolescence, recommendations vary by country. Many high- and middle-income countries, including the United States and Korea, recommend a single dose of the adult formulation of tetanus and reduced-dose diphtheria and acellular pertussis combination vaccine (Tdap) instead of an adult formulation of tetanus-diphtheria toxoids (Td) vaccine to provide protection against not only diphtheria and tetanus, but also pertussis.9 However, vaccination with Td still is recommended in many countries in Asia, South America, and Africa, such as Peru, South Africa, and India.10 The cost of Td is considerably lower than that of Tdap.11
Despite a large number of studies on the immunogenicity and safety of Tdap and efforts to develop a new Tdap,121314 the development of Td has been limited. A new Td, BR-TD-1001, has been developed by a Korean pharmaceutical manufacturer with two purposes: for its supply to countries where Td is used widely and for its use in the initial step of novel Tdap development with the plan of adding acellular pertussis antigens. In this study we aimed to evaluate the immunogenicity and safety of BR-TD-1001 with respect to those of the licensed control Td.
METHODS
Study design and participants
A phase 3, randomized, double-blind, active-controlled trial was conducted in 10 sites in Korea from June 2016 to October 2017.
Healthy children aged 10 to 12 years who had received five doses of diphtheria-tetanus-acellular pertussis (DTaP) vaccine up to the age of 6 years were eligible for inclusion. The eligible ages of participants were determined according to the immunization schedule of Korea. Children were excluded if they met any of the following criteria: a history of a serious adverse event (SAE) after injection of a vaccine against diphtheria, tetanus, or pertussis; had received a diphtheria, tetanus, or pertussis vaccine within 5 years of enrollment consideration; had clinically-diagnosed or laboratory-confirmed diphtheria or tetanus; had a history of allergy to any vaccine component; had a chronic illness or medical condition that could interfere with participation in the trial; had received immune-modifying drugs within the past 3 months; had received blood products within the past 3 months or was planning to receive blood products during the trial period; had received any vaccine within the past 30 days; or had any other clinically significant medical or psychological condition that the investigator considered reason for ineligibility for the study.
The participants were assigned randomly in a 1:1 ratio to receive either one dose of the BR-TD-1001 or the control Td (Td-pur, GlaxoSmithKline, London, UK). PROC PLAN (SAS version 9.2) (SAS Institute, Cary, NC, USA) was used to generate the randomization list.
Investigational and control vaccine
The investigational vaccine, BR-TD-1001, manufactured by Boryung Biopharma (Seoul, Korea) contained 2 IU (2.5 Lf) of diphtheria toxoid (Corynebacterium diphtheriae Park Williams #8 strain) and 20 IU (5 Lf) of tetanus toxoid (Clostridium tetani Harvard strain) per 0.5 mL dose as well as 4.25 mg of sodium chloride and 0.5 mg of aluminum hydroxide as adsorbents. The control vaccine, Td-pur contained 2 IU (2.5 Lf) of diphtheria toxoid (C. diphtheriae Park Williams #8 strain), 20 IU (5 Lf) of tetanus toxoid (C. tetani, Massachusetts F1 strain), 4.25 mg of sodium chloride, and 1.5 mg of aluminum hydroxide per 0.5 mL dose. The Park Williams #8 strain of C. diphtheriae is used worldwide as the source of diphtheria toxoids.15 The Harvard C. tetani strain is one of several strains used widely to manufacture tetanus toxoids.16
Both vaccines were provided in prefilled syringes, which were stored at 2–8°C and intramuscularly injected into the deltoid muscle of each participant.
Immunogenicity assessment
Serum samples were collected from participants before vaccination and at 28 to 35 days after vaccination. The samples were stored at −70°C until they were tested. Seroprotection was determined by measuring anti-diphtheria toxin immunoglobulin G (IgG) and anti-tetanus toxin IgG using enzyme-linked immunosorbent assay kits (IBL International GmbH, Hamburg, Germany) for diphtheria (Cat. No. RE56191) and tetanus (Cat. No. RE56901), respectively, according to the manufacturer's instructions as described in previous study.17 The cut-off values were specified as follows: diphtheria and tetanus antibody concentrations < 0.1 IU/mL were considered non-seroprotective, and levels ≥ 0.1 IU/mL were considered seroprotective.1819
The non-inferiority of BR-TD-1001 with respect to immunogenicity was evaluated using the following statistical parameters. The primary immunogenicity objective was to compare the post-vaccination antibody response between the BR-TD-1001 group and the control group. The secondary immunogenicity objective was to determine the difference in seroprotection rate at 28 days after vaccination. The criterion for non-inferiority was that the upper limit of the one-sided 97.5% credible interval of the difference in the seroprotection rate (that of the control group minus that of the BR-TD-1001 group) for diphtheria and tetanus should be < 10%. The third immunogenicity objective was to compare the proportion of participants who demonstrated a boost response. Such a response was noted when a < 0.1 IU/mL pre-vaccination antibody titer increased to ≥ 0.4 IU/mL after vaccination or a ≥ 0.1 IU/mL pre-vaccination antibody titer increased at least fourfold after vaccination.
Safety assessment
Participants were observed for 30 mintues at the investigational site after vaccination, and study staff recorded any adverse events (AEs). AEs that occurred > 30 minutes after vaccination were recorded by parents or guardians on a diary card.
The solicited local AEs were pain, tenderness, erythema, and swelling at the injection site. The solicited systemic AEs included fever, anorexia/vomiting, diarrhea, headache, fatigue, and myalgia. Unsolicited AEs were represented by System Organ Class and Preferred Terms according to the Medical Dictionary for Regulatory Activities.20 An SAE was defined as any untoward medical occurrence resulting in hospitalization, significant disability, life-threatening signs, or death. The intensity of solicited local and systemic AEs and unsolicited AEs was evaluated on a three-grade scale of severity including mild, moderate, severe according to the protocol issued by the Ministry of Food and Drug Safety (MFDS) of Korea.21 Solicited local and systemic AEs were reported within 7 days (Days 0–6), and unsolicited AEs and SAEs were reported within 29 days (Days 0–28).
The safety objective was a comparison of the safety profiles of the BR-TD-1001 and the control Td.
Statistical analysis
The sample size calculation was based on expected precision of the results. Assuming 95% seroprotection rates for each diphtheria and tetanus toxoid and a drop-out rate of 10%, a sample size of 218 participants (109 participants per group) was calculated to meet all endpoints, with an overall power of 90% for non-inferiority and a one-sided overall type 1 error (alpha) level of 0.025 for each comparison, resulting in an alpha < 0.05. For immunogenicity analysis, geometric mean titer (GMT) was computed as the anti-log of the mean concentration transformation. The seroprotection rate of each vaccine group was calculated with its 95% confidence interval (CI) using the Clopper-Pearson method. The upper limit of the one-sided 97.5% credible interval of the difference in seroprotection rate between the two groups was calculated based on the Wilson score method without continuity correction. For safety analysis, the 95% CI of the AE rate was calculated using the exact binomial distribution of proportions. The differences in categorical variables between the BR-TD-1001 and control groups were tested using the χ2 test or Fisher's exact test. P values < 0.05 were considered statistically significant. All statistical analyses were performed using SAS software, Version 9.2 or higher.
Ethics statement
This study was conducted in accordance with the International Conference on Harmonization Guidelines for Good Clinical Practice and the Declaration of Helsinki. The study protocol and informed consent form were approved by the MFDS of Korea (investigational new drug number: 11860) and the Institutional Review Board of each study site (St. Vincent's Hospital: VC16BDMT0114). This study was registered retrospectively with Clinicaltrials.gov (NCT 04618939). Written informed consent was obtained from the parents or legal representatives of each participant, and written child assent was obtained from each participant prior to enrollment.
RESULTS
Participants
Among the 218 participants enrolled in the study, 108 and 110 were randomized into the BR-TD-1001 and control groups, respectively. The demographic characteristics of the participants are shown in Table 1. There were no significant differences between groups in demographic characteristics, including sex, age, body weight, and height. The per-protocol populations of the BR-TD-1001 and control groups were 102 and 105 participants, respectively. The flow of participants through the study is shown in Fig. 1. For safety assessment, all 108 BR-TD-1001 recipients and all 110 control vaccine recipients were included.
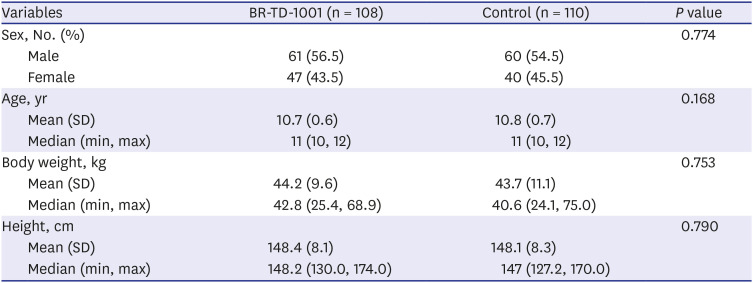
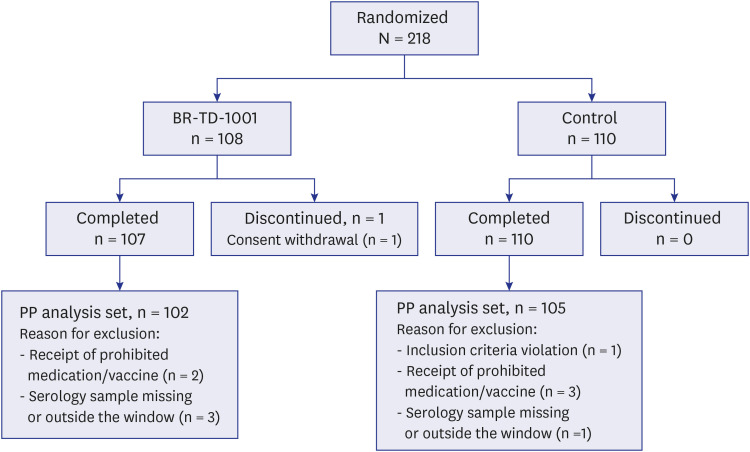
Table 1
Demographic characteristics of participants
![]()
Immunogenicity
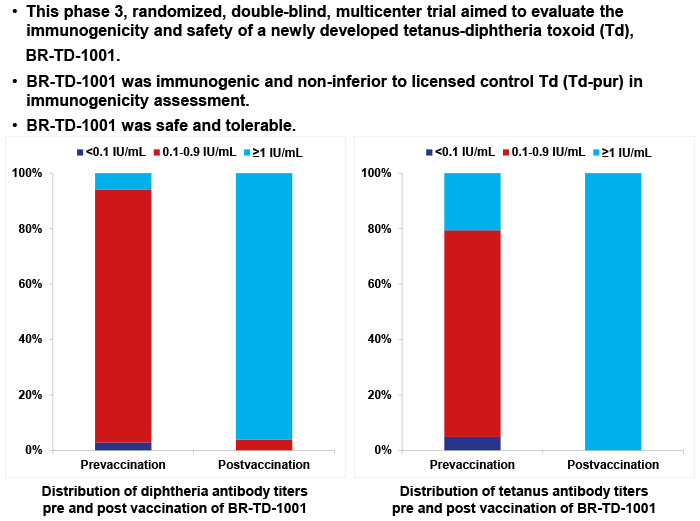
The results related to the first immunogenicity endpoint assessment, antibody response after vaccination, are shown in Table 2. For diphtheria, the GMT of anti-diphtheria toxin IgG increased significantly in both the BR-TD-1001 and control groups. There was no significant difference between groups in comparison of proportions of participants who achieved an antibody titer of ≥ 1 IU/mL (P = 0.256) and an antibody titer of 0.1–0.9 IU/mL (P = 0.256). For tetanus, the GMT of anti-tetanus toxin IgG increased significantly in both the BR-TD-1001 group and control groups. Again, there was no significant difference between groups in comparison of proportions of participants who achieved an antibody titer of ≥ 1 IU/mL (P = 1.000) and an antibody titer of 0.1–0.9 IU/mL (P = 1.000).
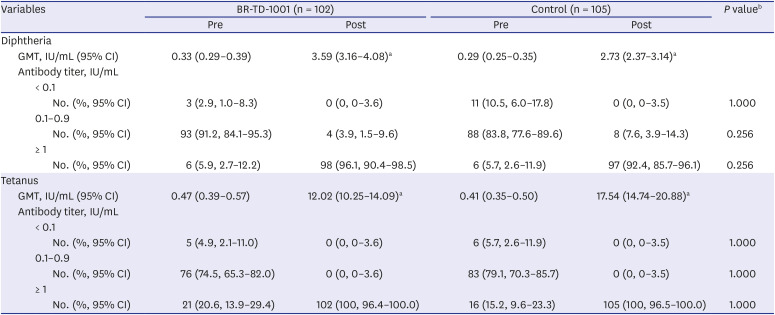
Table 2
Antibody responses after vaccination
CI = confidence interval, GMT = geometric mean titer, Pre = prevaccination, Post = postvaccination.
aThe P value for comparison of pre- and post-vaccination GMTs was < 0.05.
b These P values are for comparison of the proportions of participants with categorical antibody titers between the BR-TD-1001 and control groups after vaccination.
![]()
The results related to the secondary immunogenicity endpoint are shown in Table 3. Both groups demonstrated seroprotection rates of 100% against diphtheria after vaccination (BR-TD-1001 group 95% CI, 96.4–100%; control group 95% CI, 96.5–100%). The upper limit of the one-sided 97.5% credible interval of the difference in seroprotection rate (2%) was less than 10%; thus, BR-TD-1001 fulfilled the non-inferiority parameter for seroprotection against diphtheria. Both groups demonstrated seroprotection rates of 100% against tetanus after vaccination (BR-TD-1001 group 95% CI, 96.4–100%; control group 95% CI, 96.5–100%). The upper limit of the one-sided 97.5% credible interval of the difference in seroprotection rate (2%) was less than 10%; thus, the BR-TD-1001 group fulfilled the non-inferiority parameter for seroprotection against tetanus.

Table 3
Immunogenicity evaluation of seroprotection rate and boosting response
![]()
The results related to the third immunogenicity endpoint, boost response, are shown in Table 3. For diphtheria, 90.2% (95% CI, 82.7–95.2%) of the participants in the BR-TD-1001 group and 82.9% (95% CI, 74.3–89.5%) of participants in the control group demonstrated a boost response, and the difference between the two groups was not significant (P = 0.122). For tetanus, 96.1% (95% CI, 90.3–98.9) of participants in the BR-TD-1001 group and 99.0% (95% CI, 94.8–100%) of participants in the control group demonstrated a boost response, and the difference was not significant (P = 0.208).
Safety
The two vaccines had similar safety profiles. The incidence of AEs is shown in Table 4. The proportions of reported solicited local AEs were 58.3% and 70.0% in the BR-TD-1001 and control groups, respectively, and there was no significant difference (P = 0.072). There also was no significant difference between the BR-TD-1001 and control groups in the proportions of participants with solicited systemic AEs (P = 0.963) or unsolicited AEs (P = 0.610). Of the solicited local AEs, tenderness was most common in both the BR-TD-1001 group (56.5%) and the control group (68.2%). Of the solicited systemic AEs, myalgia was most common in both the BR-TD-1001 group (25.0%) and the control group (24.5%). Of the unsolicited AEs, infection and infestations were most common in both the BR-TD-1001 group (9.3%) and the control group (10.9%). Most participants demonstrated solicited local AEs, solicited systemic AEs and unsolicited AEs of mild or moderate (Fig. 2). None of the AEs led to hospitalization or discontinuation during the study period.
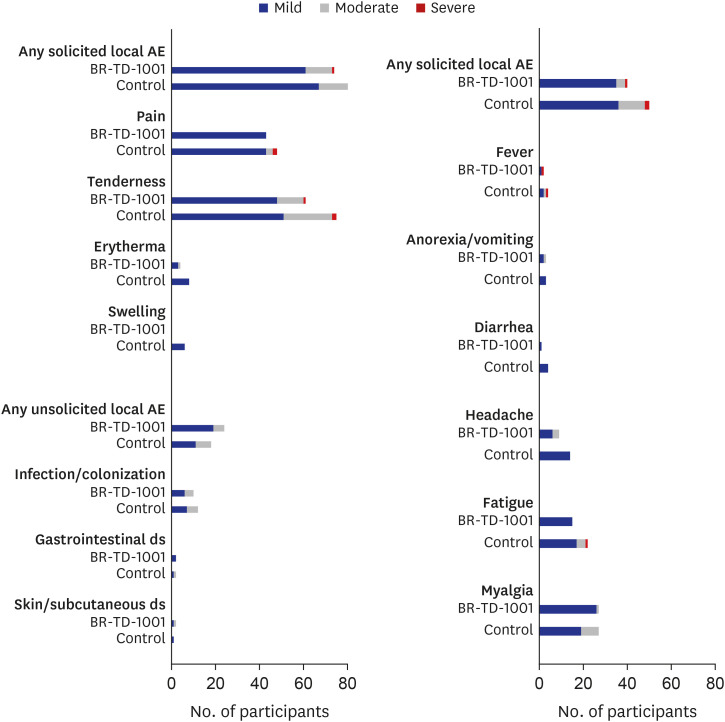
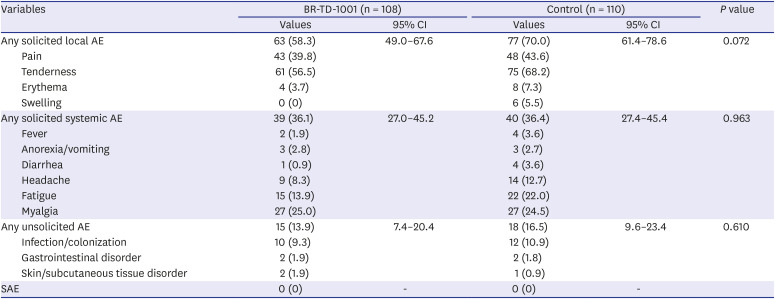
Fig. 2
Number of participants in BR-TD-1001 group and control group with AEs according to toxicity grade (mild, moderate, severe).
AE = adverse event, ds = disorder.
![]()
Table 4
Postvaccination safety assessment
Values are presented as number (%).
AE = adverse event, CI = confidence interval, SAE = serious adverse event.
![]()
DISCUSSION
The immunogenicity profile of the BR-TD-1001 group found in this study is comparable to those of other Tds reported previously.1516 The BR-TD-1001 group demonstrated non-inferior immunogenicity to the control group in terms of antibody levels, seroprotection rate, and boost response among study participants. Most participants in the BR-TD-1001 group demonstrated diphtheria and tetanus antibody titer ≥ 1 IU/mL, exceeding the cut-off values, and this finding was similar to that of the control group. In addition, the BR-TD–1001 vaccine met the international standard in terms of strains of toxoids used.
Pain was the most common local AE in both groups, consistent with the Td vaccine AE report of the Vaccine Adverse Event Reporting System maintained by the U.S. Centers for Disease Control and Prevention.22 Consistent with previous studies, both BR-TD-1001 and control groups experienced a low incidence of fever. Fever after DTP combination vaccine is associated with the pertussis component,23 and administration of diphtheria and tetanus toxoids alone is not associated with incidence of fever. Myalgia, which was presumed to be associated with the injection, was the most common systemic AE in both groups. Infection and infestations were the most common unsolicited AEs in both groups. These were not related causally to either vaccine but seemed to be incidental pediatric conditions. None of the participants in either group experienced any SAEs, including an arthus-type hypersensitivity reaction, which is associated with the Td vaccine.
The AEs after Td vaccination are related with dose of antigen, number of previous boost doses, and time since the previous dose.16 As a high dose of diphtheria toxoid can induce a greater number of AEs or SAEs, Td or Tdap that contain a reduced dose of diphtheria toxoid is recommended in children aged ≥ 7 years instead of the DTP combination vaccine.7 Neither of the toxoid constituents of the BR-TD-1001 vaccine exceeded World Health Organization (WHO) standards.
Seroprotection against diphtheria and tetanus elicited by vaccination wanes more rapidly than seroprotection against viral antigens such as measles24 and generally wanes by adolescence.17 Thus, the WHO recommends that three primary doses and three booster doses of diphtheria- and tetanus-containing vaccine be administered during childhood and adolescence. In adulthood, a booster dose every 10 years for life is recommended.79 Despite high vaccination coverage against diphtheria and tetanus in most parts of the world, vaccination coverage of the primary series is as low as 70%, and coverage of the booster series is even lower in some parts of world.25 Diphtheria and tetanus remain important public health problems in these regions.
There are ongoing outbreaks of diphtheria, with 5,000–17,000 cases reported worldwide annually, of which 30–60% occur in children under 15 years of age. In 2017, a major outbreak of diphtheria was reported in a Rohingya refugee center in Bangladesh,326 and outbreaks of diphtheria have also occurred in Haiti, Venezuela, and Yemen in the past 5 years due to poor access to vaccination as a result of economic crises or civil war.27 Maintaining herd immunity by vaccination is essential to control of diphtheria.
Despite a decreasing trend in the incidence of tetanus, approximately 80,000 cases were reported in 2017, of which 38,000 were fatal. Approximately half the cases were in children younger than 5 years.3 Tetanus occurs mostly in African and Asian countries, and a considerable portion of cases is associated with illegal medical procedures and maternal and neonatal tetanus contracted through wounds during the neonatal period.4 Maternal and neonatal tetanus can occur if the mother is not immunized against tetanus and cannot provide antibodies to her newborn child. Tetanus is not transmitted from person to person, but C. tetani cannot be removed from the environment. Spores cause tetanus to grow in a soil-rich environment, contaminated soil, animal waste, and debris and to enter the body through puncture wounds.16
Td vaccination, which can be administered from the age of seven years, is an effective strategy for protecting children from diphtheria and tetanus in endemic regions. The cost of Td is one-half to two-thirds that of Tdap,11 and use of Td instead of Tdap could facilitate mass supply by governments and international organizations. With the view of export, a new Td was developed by a Korean manufacturer even though diphtheria was eliminated in Korea in 1988 and tetanus had decreased greatly in Korea since 1990, less than 50 cases per year, and most of them occur in patients older than 40.28 The results of this study will be useful in promoting Td vaccination in regions with a high incidence of diphtheria or tetanus.
Pertussis is a highly contagious respiratory infection; although universal vaccination substantially reduced the numbers of cases and deaths, epidemic cycles occur every two to five years, even in countries with high vaccination coverage.25 Studies have demonstrated that the protection induced by immunization wanes rapidly, being effective for only 2–3 years.29 Many countries recommend Tdap administration in those aged 11–12 years and a decennial booster dose of Td or Tdap.789 Although use of Tdap is expected to increase continuously worldwide, a limited number is available. Thus, development of novel Tdaps is necessary. Vaccine manufacturers plan to add acellular pertussis antigens (pertussis toxin, pertactin, and filamentous hemagglutinin) to vaccine products currently under investigation.
In conclusion, the present study indicates that the BR-TD-1001 Td is non-inferior to the licensed control Td, Td-pur, in terms of immunogenicity and it was safe and well tolerated. This finding is essential for clinicians and healthcare authorities.
 XML Download
XML Download