

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel coronavirus responsible for coronavirus disease 2019 (COVID-19), which was first detected in Wuhan, China, in December 2019.1 This disease rapidly spread worldwide, and the World Health Organization declared it to be a global pandemic in January 2020.2 The severity of the disease ranges from asymptomatic to life-threatening.34 SARS-CoV-2 has infected nearly 130 million people and caused 2.8 million deaths worldwide as of April 6, 2021.5 All epidemiological evidence to date shows that the severity of COVID-19 decreases with a decrease in age.67 While there is abundant information about risk factors for disease severity and mortality in adults (for example, advanced age, cardiovascular disease, diabetes, cancer, immunosuppression, obesity, and tobacco use), limited information is available about risk factors in children.8
Initially, asthma was thought to be a risk factor because COVID-19 affects the respiratory system. Theoretically, excessive mucus secretion in the bronchi, epithelial damage, airway obstruction, and local immunosuppression caused by inhaled corticosteroids create an excellent environment for SARS-CoV-2 infection in patients with asthma.9 Moreover, patients with asthma have a greater risk of more severe outcomes when infected with common cold viruses, such as coronaviruses.10 When infected with respiratory viruses, patients with asthma have a delayed and insufficient innate antiviral immune response at the tissue level.11 However, accumulated evidence revealed that this concern was unwarranted. Unlike the few studies that demonstrated asthma to be a risk factor, many studies revealed that asthma in children is not a risk factor for COVID-19.8121314 Various theories have been put forward to explain this. Some mechanisms proposed to explain the milder course of COVID-19 in children with asthma are as follows: 1) Th2-mediated inflammation results in a decrease in the expression levels of angiotensin-converting enzyme 2 (ACE2) and transmembrane protease serine 2 (TMPRSS2) genes, which mediate the entry of SARS-CoV-2 into cells, 2) eosinophilic inflammation reduces the viral load in respiratory cells, and 3) the use of inhaled corticosteroids in children with asthma downregulates the expression levels of ACE2 and TMPRSS2 genes.8111516
There is limited information about the effect of the COVID-19 pandemic on children and adolescents with asthma. In the present study, we aimed to assess the attitudes of adolescents with asthma toward the COVID-19 pandemic and determine the effects of the pandemic on their quality of life (QoL).
METHODS
Patients and controls
In total, 155 patients who had asthma and were aged 12–18 years and 124 healthy controls who did not have asthma or other chronic diseases and belonged to a similar age group were invited to participate in the present study. Of these, 125 patients with asthma and 98 healthy controls who accepted the invitation to participate were enrolled in the study. The controls were randomly selected from those who were admitted to the general outpatient clinic with temporary complaints between March 2020 and March 2021. The patient and control groups were similar in terms of the female/male ratio (55/70 and 48/50, respectively) and mean participant age (14.6 ± 2 and 15.1 ± 1.65 years, respectively) (P = 0.459 and P = 0.062, respectively). The diagnosis of COVID-19 is based on the presence of clinical findings and PCR positivity.
A partial lockdown was imposed on every person under the age of 18 on most days, from the date of the first case of COVID-19 in Turkey to the study period. Therefore, patients and controls were subject to the same restrictions in the same period.
Definitions
Asthma is the most common chronic inflammatory disease of the respiratory system, which is characterized by reversible airway obstruction and bronchial hypersensitivity.17 In our study, the diagnosis of asthma was made by a pediatric allergist based on the Global Asthma Initiative (GINA) guidelines.18
Rhinitis is an inflammatory disease of the nasal mucosa, characterized by nasal symptoms such as runny nose, sneezing, nasal congestion, and nasal itching. These symptoms occur for more than an hour over two or more consecutive days.19 Atopic dermatitis is a chronic inflammatory skin disease characterized by intense itching, dry skin, and recurrent eczema lesions.20 In our patients, the diagnosis of allergic rhinitis and atopic dermatitis were made according to the history and physical examination.
Allergic sensitization was defined as skin prick test positivity or specific immunoglobulin E (IgE) positivity against any allergen causing clinical symptoms.
Questionnaires
The questionnaire form administered to the participants consisted of three parts. In the first part, all the participants were asked whether they complied with the protective measures against COVID-19 (i.e., compliance with general recommendations and physical distancing, mask use, and handwashing).
In the second part, the participants’ level of concern about COVID-19 was measured. For this purpose, they were asked seven questions using a visual analog scale (VAS) created by us (with scores ranging from 0 to 10 according to the level of concern).
The third part of the questionnaire consisted of EUROHIS-QOL 8, a part of the World Health Organization Quality of Life (WHOQOL) questionnaire. EUROHIS-QOL 8 consists of eight questions (related to the overall QoL, general health, energy, daily life activities, self-esteem, social relationships, finances, and home) selected from WHOQOL.2122 The first question in the scale is related to the general perception of QoL, while the second question is related to the general perception of health. The remaining six questions are related to energy for everyday life, satisfaction with daily activities, self-satisfaction, satisfaction with personal relationships, income levels to fulfil needs, and home conditions.21 The short (8-item) scale EUROHIS-QOL 8 is recommended for public health research as it demonstrates good cross-cultural fieldwork performance and satisfactory convergent and discriminant validity.23 The validated Turkish version of EUROHIS-QOL 8 was used in the present study.24 The questions in the questionnaire and in the asthma control test were asked via a phone call.
This study was conducted between 1 March to March 31, 2021, one year after the first COVID-19 case was reported in Turkey.
Statistical analysis
Experimental (post-hoc) power analysis was performed considering the present findings of the research. The small effect size value was obtained by comparing the mean scores of the EUROHIS-QOL8 scale between patients (n = 125; 31.2 ± 6.7) and controls (n = 98; 33.7 ± 4.4), and it was calculated as d = 0.44. Using the calculated effect size, the power value obtained from our study, which was a Type I error at the level of 5% and which was n: 223 units in total, was determined as 90%. The analysis was performed with G*Power (Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175-191.) program.
Statistical analyzes were performed using the statistical package SPSS 23 (IBM Corp., Armonk, NY, USA). Categorical data were expressed as frequencies and percentages, and continuous data as mean ± standard deviation (SD) or median (minimum and maximum). Kolmogorov-Smirnov test and histogram were used to test the normality of the distribution of data. Categorical variables were compared using the Pearson's χ2 test and Fisher exact test. Group comparisons were made using either the independent sample T-test or the Mann-Whitney U test, depending on whether the variables have a normal distribution. The Wilcoxon signed-rank test was used to compare two related samples. A P value of less than 0.05 was considered statistically significant.
RESULTS
The percentage of allergic sensitization to at least one allergen was 80.2% (n = 101) in patients with asthma. The second most common allergic disease accompanying asthma was allergic rhinitis (n = 61, 48.8%). Inhaled corticosteroids were the most commonly used medicine by asthmatic patients in our study group (n = 63, 50.4%). General characteristics of the patients are given in Table 1.
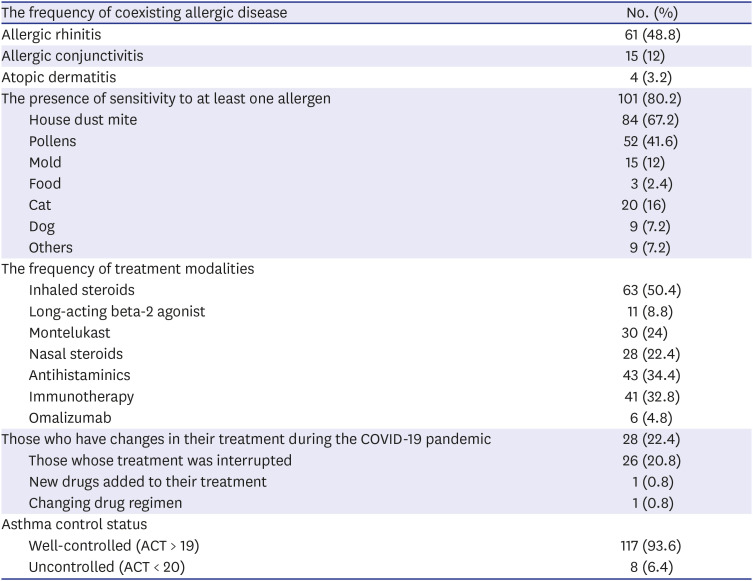
Table 1
General characteristics of adolescents with asthma (n = 128)
![]()
Twenty-two patients (17.6%) stated that they gave up applying to the hospital despite their existing complaints.
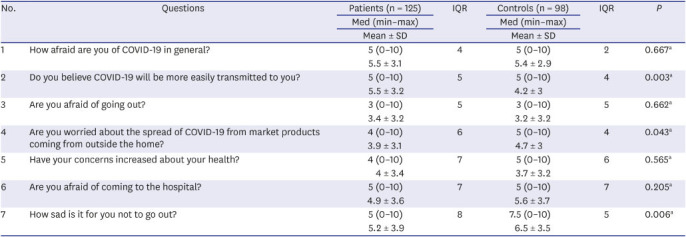
In our study, patients with asthma believed COVID-19 could be transmitted more easily to them (Table 2). In addition to the total EUROHIS QOL score, patients with asthma had lower scores with respect to the general perception of QoL (Q1), satisfaction with health status (Q2), economic status (Q7), and home conditions (Q8), compared to controls (Table 3).
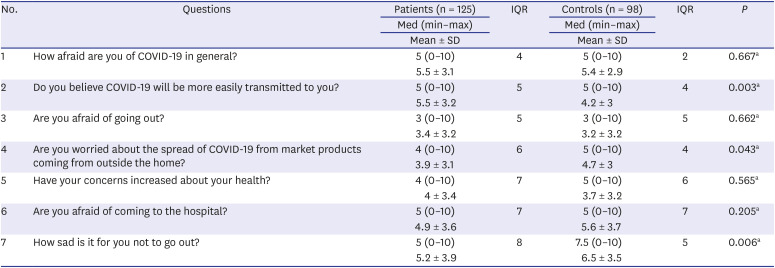
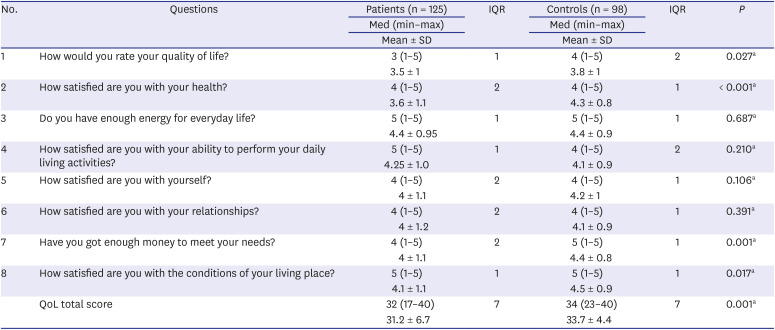
Table 2
Patient concerns regarding the COVID-19 pandemic graded using VAS (0: not at all, 10: very much)
COVID-19 = coronavirus disease 2019, VAS = visual analog scale, SD = standard deviation, Med = median, Min = minimum, Max = maximum, IQR = interquartile range.
aMann Whitney U test.
![]()
Table 3
The EUROHIS-QOL 8-Item scores of patients and controls in COVID-19 pandemic (very bad:1, very good:5)
COVID-19 = coronavirus disease 2019, SD = standard deviation, Med = median, Min = minimum = Max = maximum, IQR = interquartile range, QoL = quality of life.
aIndependent sample t-test.
![]()
Almost all asthmatic patients and controls stated that they generally followed the rules for protection from COVID-19. The rates of wearing face masks outside and compliance with physical distancing were high in both groups. The median daily handwashing frequency was similar between the two groups, both before (median: 5, minimum: 0, maximum: 40, IQR: 7; median: 5, minimum: 0, maximum: 20, IQR: 4) and after (median: 10, minimum: 2, maximum: 50 IQR: 10; median: 8, minimum: 3, maximum: 30, IQR: 5) and during the pandemic (P = 0.100 and P = 0.244). Compliance with protection rules and some aspects of daily life changes during the COVID-19 pandemic among patients and controls are given in Table 4.
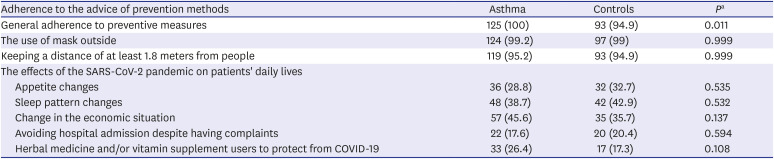
Table 4
Adherence to COVID-19 prevention recommendations and daily life changes during the pandemic
Values are presented as number (%).
COVID-19 = coronavirus disease 2019, SARS-CoV-2 = severe acute respiratory syndrome-coronavirus-2.
aPearson's chi-squared test.
![]()
The frequency of COVID-19 in asthmatic patients (n = 2, 1.6%) was lower than in the control group (n = 6, 6.1%), but was not statistically significant (P = 0.142). The number of patients who had casual contact with COVID-19 positive cases was lower in asthmatics (n = 52, 41.6%) than in controls (n = 71, 72.4%) (P < 0.001).
Less than half of both groups (n = 57.45, 6%; n = 40, 40.8%) believed that COVID-19 would completely disappear from the world (P = 0.475).
Asthmatic patients were found to differ on some points between genders. Fear of COVID-19 infection was higher in females (median: 6 minimum: 0, maximum: 10, IQR: 5) than in males (median: 5, minimum: 0, maximum: 10, IQR: 4) (P = 0.009). Female patients believed COVID-19 would be more easily transmitted to them (median: 7, minimum: 0, maximum: 10, IQR: 5) than to males (median: 5, minimum: 0, maximum: 10, IQR: 4) (P < 0.001). Additionally, female patients were more afraid of going out (median: 5, minimum: 0, maximum: 10, IQR: 5) than males (median: 2, minimum: 0, maximum: 10, IQR: 5) (P = 0.015). The sadness of being restricted from going out was higher in female patients (median: 7, minimum: 0, maximum: 10, IQR: 5) than in males (median: 5, minimum: 0, maximum: 10, IQR: 7) (P = 0.001). The median frequency of handwashing in female patients (median: 10, minimum: 5, maximum: 50, IQR: 8) was higher than in males (median: 6, minimum: 2, maximum: 50, IQR: 5) during the COVID-19 pandemic (P = 0.001).
The score of fear of COVID-19 infection in patients with changes in sleep patterns (median: 6.5, minimum: 0, maximum: 10, IQR: 4) was significantly higher than in those with no changes in sleep patterns (median: 5, minimum: 0, maximum: 10, IQR: 4) (P = 0.025).
The rate of disruption in treatment (n = 11, 50%) and change in appetite (n = 11, 50%) was significantly higher in those who gave up applying to the hospital despite their current complaints, compared to those who did not (n = 28, 27.2%; and n = 25, 24.3%) (P = 0.036 and P = 0.016). The level of concern about the health status of the patients who gave up applying to the hospital (median: 5.5, minimum: 0, maximum: 10, IQR: 8), and the level of concern about being affected in their treatment (median: 6.5 minimum: 0, maximum: 10, IQR: 9), was significantly higher than those who did not (median:3, minimum: 0, maximum: 10, IQR: 6; and median:2, minimum: 0, maximum: 10, IQR: 6) (P = 0.049, P = 0.028). There was no difference in the QoL between the two groups.
The median frequency of handwashing in patients and controls (median: 10, minimum: 2, maximum: 50, IQR: 10; median: 8, minimum: 3, maximum: 30, IQR: 5) was significantly higher than before the pandemic (median: 5, minimum: 0, maximum: 40, IQR: 7; and median: 5, minimum: 0, maximum: 20, IQR: 4) (P < 0.001 and P < 0.001).
In order to determine the effect of asthma only, asthmatic adolescents and controls were compared, excluding patients with allergic rhinitis and atopic dermatitis. Asthmatic adolescents without other allergic diseases believed COVID-19 would be more easily transmitted to them (the median VAS score at Q2 was 7 [minimum: 0, maximum: 10] in patients) and their total QoL scores (31.4 ± 6.7) was lower than controls (median VAS score at Q2 was 4 (minimum: 0, maximum: 10) and 33.7 ± 4.4, respectively) (P < 0.001 and P = 0.009, respectively) (Supplementary Tables 1 and 2).
The frequency of discontinuing or not taking the treatment due to the pandemic was higher in patients who received allergen IT (n = 20, 48.8%, and n = 18, 43.9%) than in those who received other treatments (n = 6, 7.1%, and n = 21, 25%) (P < 0.001, and P = 0.032).
Patients with uncontrolled asthma had lower scores than well-controlled patients for each of the EUROHIS questions. In addition, patients with uncontrolled asthma had significantly lower Q3 scores (3.75 ± 1.4), Q4 (3.5 ± 1.4), compared to well-controlled patients (4.5 ± 0.9; 4.3 ± 0.9; 7) (P = 0.040, P = 0.026) (Supplementary Tables 3 and 4).
DISCUSSION
Many studies have shown that COVID-19 is rarer and milder in children than the general population.1622242526272829 Unlike children, both asthma and severe asthma have been shown as risk factors for COVID-19 mortality in a large cohort of 17 million adults in the UK.30 It has been suggested that the main causes of the low rate of COVID-19 in children compared to adults are associated with lower expression of ACE2 receptors in the respiratory epithelium and more frequent exposure to a wide variety of pathogens, resulting in immunity to common coronaviruses.11 The role of T2 (type-2) inflammation in the outcome of children with asthma infected with SARS-CoV-2 is not elucidated completely. Analysis of induced sputum samples in adults with severe asthma who received ICS, especially in high doses, found reduced ACE2 and TMPRSS2 gene.31 Additionally, Jackson et al.32 showed decreased ACE2 gene expression in airway cells of patients with asthma and respiratory allergies with high IgE. Lower age and presence of asthma can reduce the level of ACE2 expression.33 Sajuthi et al.34 reported that while T2 inflammation had a strong negative effect on ACE2 expression in the airway, it upregulated airway epithelial TMPRSS2 expression. Moreover, the lower prevalence of asthma among COVID-19 cases may be due to underdiagnosis and underreporting or related to patients with chronic lung disease being more careful when applying physical distance and other measures to prevent infection.8 Consistent with previous data, the frequency of COVID-19 was lower in asthmatic patients than in controls in our study.
In COVID-19 pandemic, children and adolescents have been greatly affected by the sudden withdrawal from school, social life, and outdoor activities. Several studies have shown that prolonged school closure and home confinement negatively affect children's psychological and mental states, cause behavioral problems, and increase stress in children.353637 Deolmi et al.38 have shown that high rates of anxiety and depressive symptoms occur in children and adolescents due to the pandemic itself, social isolation, and parental stress. Some children may also have experienced increased domestic violence during this period.39 It is thought that with adequate and timely intervention, the damage caused by this pandemic to mental health can be reduced.39 We think that the fact that the anxiety scores of the controls at some points related to the pandemic were similar or higher than the patients' were due to these effects of the pandemic on all adolescents. Although the levels of concern at Q4 and Q7 were higher in the controls, it was observed that this did not ensure that the total QoL was lower than that of asthmatics.
Lung involvement is the most common serious manifestation of SARS-CoV-2 infection.40 Being aware of this situation may have led to increased anxiety and protective behavior about COVID-19 in asthmatic patients. In addition, the disruption of routine controls and treatment of patients during the pandemic period (especially in patients receiving subcutaneous immunotherapy) may have adversely affected the QoL of the patients. For these reasons, it may be expected that COVID-19 would impair the QoL in asthmatic adolescents more than in the healthy population. The fact that EUROHIS-QOL scores of patients was lower in adolescents with asthma during the pandemic period in our study supports this idea.
In a few studies conducted in our country, it has been shown that asthma negatively affects the QoL of adolescents.4142 A study conducted during the COVID-19 pandemic showed that asthmatic patients had high anxiety and depression scores, and their families had deep concerns about the transmission of COVID-19.43 Although the QoL of adolescents with asthma before and after the pandemic could not be compared, our results suggest that the QoL of asthmatic patients is adversely affected by COVID-19 pandemic.
Other allergic diseases accompanying asthma, such as allergic rhinitis and atopic, also affect QoL. To determine the effect of asthma alone, adolescents with asthma and controls were compared, excluding patients with allergic rhinitis and atopic dermatitis. Based on the subgroup analysis, it was found that the QoL of only asthmatic adolescents was lower than the controls, similar to the general patient group.
In our study, female patients were more concerned at many points related to the COVID-19 pandemic. This suggests that the gender factor should also be taken into account in psychosocial approaches to asthmatic patients.
Irregular sleep pattern is one of the important factors affecting mental health.3944 A study conducted in Italy showed that children have a significant delay in sleep timing and worsening sleep quality during the lockdown due to COVID-19.45 Hawke et al.46 showed that the COVID-19 pandemic affects mental health more in young people with asthma/allergies than those without asthma/allergies. It was determined that asthmatic patients with changes in their sleep patterns had a higher fear of COVID-19 infection in our study.
A study conducted in Turkey showed that asthma and allergic diseases do not appear to be risk factors for hospitalization for COVID-19 in children.12 They reported that asthma prevalence was 6.5% within the 107 pediatric patients, as the general prevalence of asthma in Turkish children (6.9%).1247 We determined the frequency of COVID-19 as 1.6% in our patients with asthma.
For children with asthma to attend school safely, attention should be paid to asthma control, risk stratification, and compliance with medication.48 However, during the pandemic period, the treatment of chronic diseases may be interrupted for various reasons. Parental anxiety is one of them, especially for immunotherapy.49 In our study, one of every five patients with asthma reported that their treatment was disrupted during the pandemic period, and some of them gave up admitting to the hospital due to the risk of COVID-19 despite having complaints.
In conclusion, our results support that the prevalence of COVID-19 in children with asthma is lower than in the healthy population. Asthmatic adolescents are concerned about their health conditions and their QoL is lower than the healthy population. Among adolescents with asthma, those receiving subcutaneous immunotherapy are the ones whose treatments are most affected. Policies should be developed to protect adolescents with asthma from the negative effects of the COVID-19 Pandemic and to improve their QoL.
This study contains some limitations. The first of them is that the level of QoL before the pandemic is not known, and therefore the true impact of the pandemic cannot be fully predicted. The patients were asked whether their sleep patterns changed during the pandemic period, but what these changes were and their intensities were not questioned. It will be enlightening to conduct studies focusing on sleep disorders in children with asthma during the pandemic period and to question them more deeply.
 XML Download
XML Download