

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Women remain underrepresented in surgery despite the growing female presence in the medical field in the last decades, both in Korea and worldwide. The numbers and percentages of female medical students, physicians, surgical trainees, surgeons, and academics have been consistently increasing.123456 In Korea, women accounted for 38.7% of all graduates of the medical schools and the graduate schools of medicine in 2020,7 and 22.8% of all physicians were female in 2018; however, only 8.9% of surgical physicians were women.8 In the U.S., the Association of American Medical Colleges reported that 51% of all medical students in the U.S. were female in 2018,9 and 35.2% of all active physicians were women in 2017, although they only accounted for 20.6% of surgeons.10 In the U.K., 35% of all licensed doctors are females while the only 12% of surgeons are women.5
Surgical specialties may not be an attractive career option for female medical students.111213 Studies have argued that a male-dominant culture or “old boys' club” mentality, gender biases, and gender discrimination are the main reasons for this.11415161718 Female students report greater exposure to gender discrimination and sexual harassment during medical school than male students, and the exposure gap is largest in general surgery among all medical specialties.1920 After becoming a surgeon, women are likely to experience more perceived gender discrimination than male surgeons2122 and more gender-based disadvantages in terms of promotions, salaries, editorial board membership, and so on.11423242526
Although prior studies have provided rich evidence of gender discrimination against female surgeons, the definition and measures of this discrimination have not fully reflected recent trends or more subtle and less visible types of discrimination. As explicit discrimination becomes less acceptable in society and in many organizations, discrimination continues implicitly, in covert forms.18 For instance, some recent studies have found gender differences in the feedback given during surgery training,27 autonomy in the operating room,28 and networking opportunities in the surgery society.29 These findings necessitate further research that reflects and attempts to measure the various broader phenomena of gender discrimination in surgery throughout the entire career path. Moreover, while prior studies on gender discrimination or gender gaps in surgery have focused on academic surgery, surgical trainees, or single surgical subspecialties,2130 the present study addresses more broadly defined categories of gender discrimination in the entire field of surgery including academic/clinic and surgical subspecialties.
In Korea, significant gender discrimination and inequality still exist in the surgical community; however, to date, there has been no study on gender discrimination among the members of the Korean Surgical Society. Consequently, this study aims to determine the current prevalence and degree of gender discrimination in the Korean Surgical Society and to compare the experiences and perceptions of gender discrimination between male and female Korean surgeons.
Go to : 
METHODS
Survey design
The items used to measure experiences and perceptions of gender discrimination were developed in a multistep process. First, we reviewed the literature focusing on items measuring gender discrimination in the fields of surgery, medicine, and human resource management. We also conducted in-depth interviews with eight female surgeons and consulted two professionals, one in the medical ethics field and one from the field of gender equality, regarding the developed questionnaire. The final questionnaire comprised of 16 items on experiences of gender discrimination and 17 items on perceptions of gender discrimination. We obtained the content validity of the survey items by having experts in medicine and gender equality review the questions. The reliability (Cronbach's alpha) of the 16 items on experiences of gender discrimination was 0.906, and the reliability of the 17 items on perceptions of gender discrimination was 0.951.
The survey questionnaire consisted of four sections: experiences of gender discrimination, perceptions of gender discrimination, the reasons for and methods of gender discrimination in the surgical field, and participants' demographic characteristics and affiliations. Participants responded to the questions regarding their experiences of gender discrimination with either “yes” or “no” answers, and to the questions regarding their perceptions of gender discrimination with a 4-point Likert scale with 1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree. Responses of agree or strongly agree were reported as positive, while those of disagree or strongly disagree were considered negative.
Ten experts including female surgeons and expert panels in the fields of industrial welfare and labor relations participated in the pilot test of the survey questionnaire. We revised the survey items guided by the pilot test results so that the items have greater clarity and there is as little room for misunderstanding or ambiguity as possible. The survey questionnaire was distributed via the web-based survey tool SurveyMonkey® (https://ko.surveymonkey.com).
Participants
All registered members of the Korean Surgical Society were invited to participate via email. The general terms of the study, information on the survey, and a request for consent were included with the invitation, which was linked to individualized accounts. Participation was voluntary and anonymous, and no compensation was provided. The survey was conducted from November 11, 2019, to January 11, 2020, and three reminder emails were sent out at three-week intervals. Of the 4,525 surgeon members invited to participate, 432 responded (9.5% response rate). Incomplete responses were excluded from data analysis; we analyzed 400 responses after excluding any cases with a significant amount of missing information.
Statistical analysis
We estimated unadjusted comparisons of experienced gender discrimination and perceptions of gender discrimination by gender using χ2 tests. We also used binary logistic regression to estimate the effects of gender on experienced gender discrimination and perceptions of gender discrimination while adjusting for age, subspecialty, etc. Two-tailed significance was assessed. All analyses were performed using SPSS Statistics (IBM Corp., Armonk, NY, USA).
Ethics statement
The Institutional Review Board of Chung-Ang University Hospital approved the study (CAUH 1971-004-378). All of the participants submitted informed consent when they replied.
Go to :
RESULTS
Respondents' characteristics
The final sample was 70.7% male and 29.3% female. Table 1 describes the participants' demographic characteristics and practice settings, stratified by gender. When compared with the male surgeons, the female surgeons were younger (mean age: 39.5 vs. 46.8, P < 0.001) and less experienced in practice (mean years of practice: 14.2 vs. 21.8, P < 0.001). There was a difference in the distribution of subspecialty by gender (P < 0.001) in which the male respondents were mostly concentrated in the hepatobiliary–pancreas and colorectal fields (25.4% and 24.0% of all male surgeons, respectively). Female respondents, meanwhile, were mostly concentrated in breast-thyroid-endocrine surgery (41.0% of all female surgeons). More female surgeons than men were either fellows or non-tenured academic faculty, and disproportionately more male surgeons than women were working in private practices (P < 0.001).
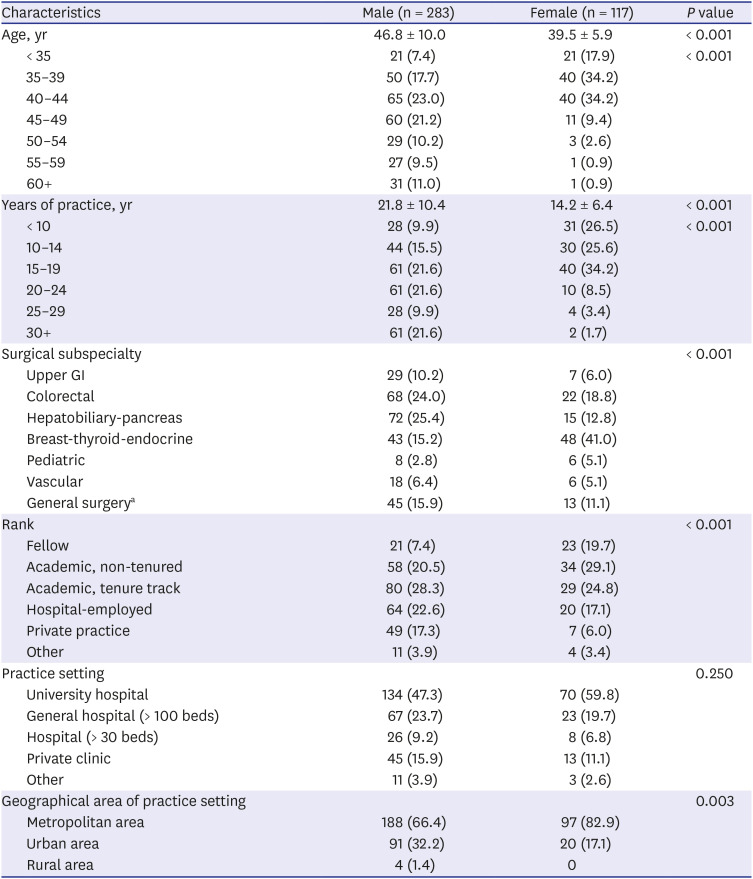
Table 1
Respondents' characteristics by gender
Values are presented as mean ± standard deviation or number of patients (%).
GI = gastrointestinal.
aWhich means not having subspecialty.
![]()
Experiences of gender discrimination
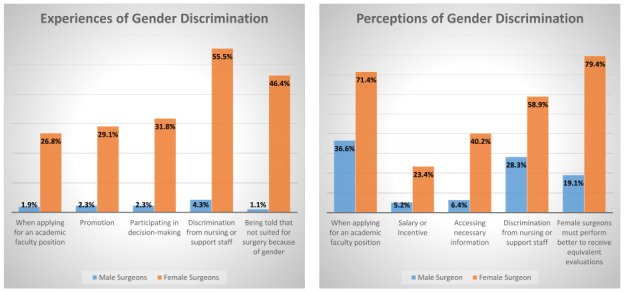
Table 2 illustrates the differences in respondents' experiences of gender discrimination according to gender. Female surgeons were more likely to report experiences of gender discrimination than male surgeons (all P < 0.001): The female surgeons reported they had experienced disrespect from a patient or caregiver (80.0%), had to perform better to receive equivalent performance evaluations to their male colleagues (63.6%), had experienced discrimination or disadvantage from nurses or other support staff (55.5%), and had experienced discrimination in informal networking and relationships within an organization (50.0%).
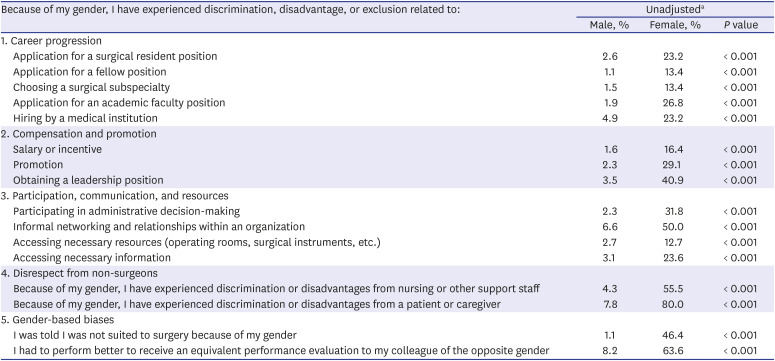
Table 2
Experiences of gender discrimination by gender
aFrequency was defined as having experienced the item via a “yes” response. Each row is from a separate χ2 test. P values are based on the χ2 tests.
![]()
Even after adjusting for years of practice, surgical subspecialty, rank, and geographical area of practice setting, female surgeons were more likely to experience gender discrimination than male surgeons across all discrimination types (odd ratio [OR] = 3.447–230.242, P < 0.001; Table 3). We examined the group of surgeons with less than 20 years of practice experience, who were on average younger and higher in terms of the proportion of female surgeons, separately from the entire sample to test if there was generational difference in the experience of gender discrimination. In this group, female surgeons were still more likely to experience gender discrimination than male surgeons across the twelve items, although the gender gap was smaller than for the entire sample (OR = 4.135–80.761, P < 0.050; Table 3). In the entire sample and in the group with less than 20 years of practice experience, female surgeons were more likely to experience discrimination than male surgeons in terms of their career progression toward academic faculty positions and responses from patients or caregivers and were more likely to be told they were not suited to surgery because of their gender.
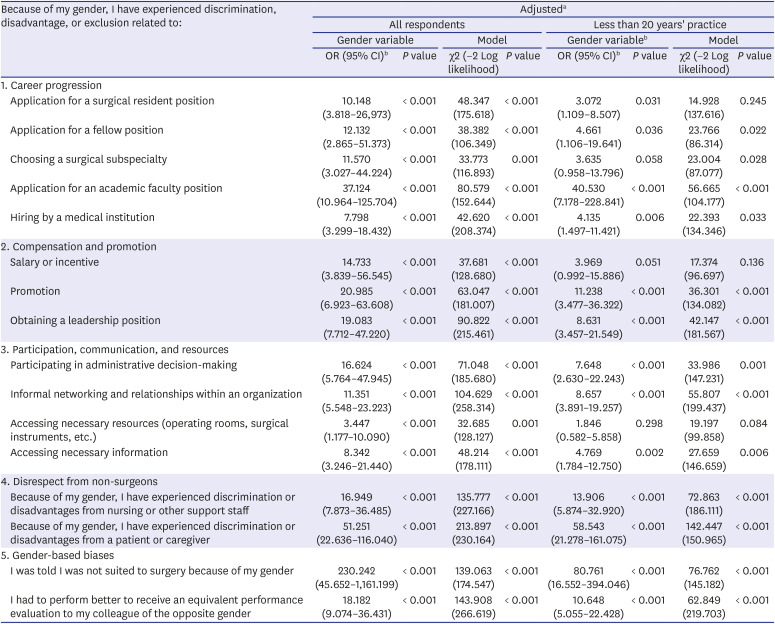
Table 3
Association between gender and experiences of gender discrimination
OR = odds ratio, CI = confidence interval.
aEach row is from a separate binary logistic regression model with gender as an independent variable. Covariates include years of practice, surgical subspecialty, rank, and geographical area of practice setting; bFemale vs. male.
![]()
Perceptions of gender discrimination
The unadjusted statistics indicated that gender differences were significant in the perception of the disadvantages faced by female surgeons. Female surgeons were significantly more likely to agree to the 16 items regarding discrimination against female surgeons (P < 0.001; Table 4), except for one item, “application for a surgical resident position.” The female surgeons perceived discrimination in the following items the most; obtaining a leadership position (female vs. male: 87.9% vs. 55.0%), discrimination by patients or caregivers against female surgeons (female vs. male: 86.9% vs. 61.8%), general biases against female surgeons in surgery (female vs. male: 84.1% vs. 48.2%), gaining promotions (female vs. male: 79.4% vs. 27.9%), and having to perform better to receive equivalent performance evaluations to male surgeons (female vs. male: 79.4% vs. 19.1%).
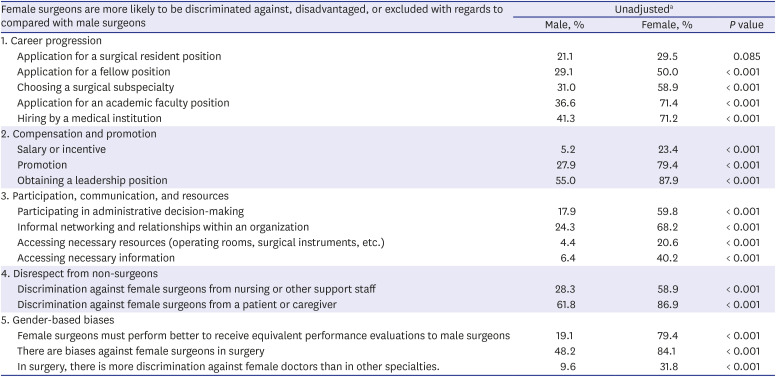
Table 4
Perceptions of gender discrimination by gender
aFrequency was defined as having perceived the item via “agree” or “strongly agree” response. Each row is from a separate χ2 test. P values are based on the χ2 tests.
![]()
After adjustment for years of practice, surgical subspecialty, rank, and geographical area of practice setting, the female surgeons were still more likely to agree about the presence of gender discrimination than the male surgeons across all discrimination items (OR = 2.438–16.842, P < 0.010; Table 5). Gender differences in the perceptions of gender discrimination were particularly significant regarding salary, promotions, accessing necessary information, and the pressure to perform better to receive equivalent performance evaluations to that of the opposite sex. In terms of perceived gender discrimination in the group of surgeons with less than 20 years of practice experiences, female surgeons perceived more gender discrimination than male surgeons across the 15 items (OR = 2.531–20.000, P < 0.010; Table 5). However, the gender differences of the perception of this group was not significantly different from the entire sample, indicating that the perception gap persists among the younger generation surgeons.
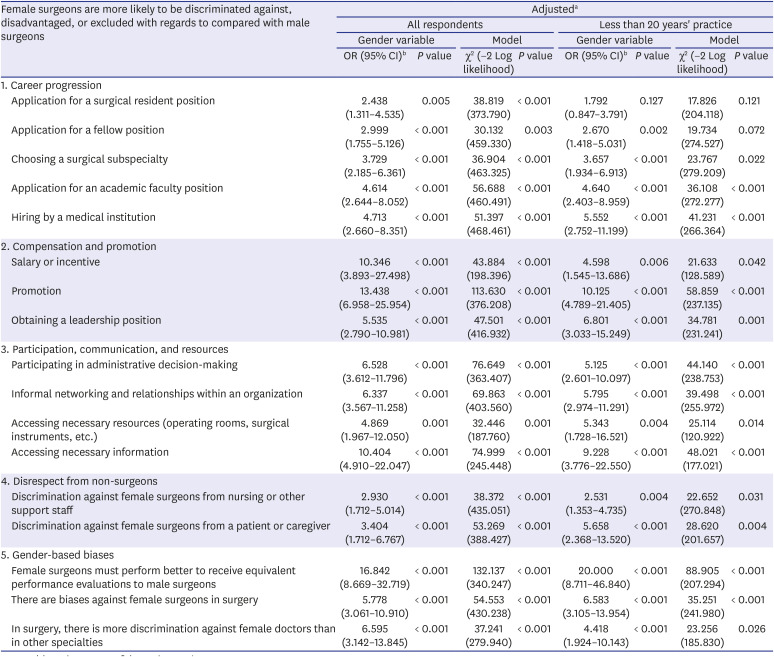
Table 5
Association between gender and perceptions of gender discrimination
OR = odds ratio, CI = confidence interval.
aEach row is from a separate binary logistic regression model with gender as an independent variable. Covariates included years of practice, surgical subspecialty, rank, and geographical area of practice setting; bFemale vs. male.
![]()
Reasons for gender discrimination and suggestions to decrease it
We asked respondents to choose the three most important reasons for gender discrimination in surgery from among 10 possible items. The two most frequently chosen responses by male surgeons were “differences in physical capacity and activity between women and men” (57.3%) and “performance hindrance due to pregnancy and childbirth” (51.8%). The two most frequent responses chosen by female surgeons were “performance hindrance due to pregnancy and childbirth” (68.7%) and “general favoritism towards male surgeons” (65.7%). We also asked respondents to choose the three most necessary policies or efforts that could reduce gender discrimination from among 11 items. The two most frequent answers given by male surgeons were “bringing in a substitute when a female surgeon takes maternity leave” (62.8%) and “awareness of the need for a work–family life balance for surgeons” (51.4%). On the other hand, the two most frequently chosen responses by female surgeons were “improving the male-dominated culture in medicine” (55.6%) and “awareness of the need for a work-family life balance for surgeons” (49.5%).
Go to :
DISCUSSION
This study explored the gender discrimination that is prevalent in surgical field of Korea and examined and discovered significant gender differences in the experiences of gender discrimination and the perception of such discrimination against female surgeons. The inclusive conceptualization of gender discrimination in this study is consistent with contemporary approaches to the broadened spectrum of gender discrimination, such as the increased interest in microaggression.3132
This study is the first attempt in Korea to examine the experience and perception of gender discrimination in surgery. There have been only very few academic studies on gender discrimination in medicine. The most recent study by Shin and Lee,33 which analyzed the survey conducted by the Korean Medical Women's Association and the Korean Intern Resident Association in 2019, is also consistent with our findings. They discovered that women showed significantly higher perception of gender discrimination than men in all surveyed areas of gender inequality, including residency, professorship, employment, promotion, pay and compensation, participation in decision making. 12.6–47.3% of women in medicine experienced discrimination across the various areas of inequality.33 A similar study by the Korean Women's Medical Association in 2011 also found that 41.0–74.2% of women in medicine agreed that discrimination existed in hiring, position, promotion, performance evaluation, etc.34 Our current study is consistent with these prior findings such that women showed higher perception of gender discrimination, ranging from 20.6% to 87.9% than men. This study provides additional specified insights on the prevalence of gender discrimination in surgery.
The results were consistent with the findings of previous studies that have identified the challenges that female surgeons and physicians experience, such as the gender pay gap, lack of role models and mentors, gender biases, and the lower likelihood of working in academic surgery and in leadership positions.1141617253033 In addition, implicit forms of discrimination, for example, the imbalanced allocation of resources or reduced access to informal networking opportunities, were no less prevalent than the obvious and visible forms in surgery. The results suggest that the traditional conceptualization of gender discrimination may fall short of capturing its full range. However, only a few studies have actually surveyed surgeons about their experiences of gender discrimination, and, although they have critically contributed to our understanding of gender discrimination in medicine and surgery, they have applied too simplistic or very limited sets of questions about gender discrimination.213536 As observed by Stephens et al.,37 implicit bias works at the subconscious level and is not only hard to recognize but can even contradict conscious beliefs. Consequently, this bias is very difficult to assess or challenge. The present study contributes important insights that illustrate the full range of gender discrimination that female surgeons face, including both explicit and implicit biases and discrimination.
The results of this study identified the gender gap in the perceived discrimination against women, consistent with previous studies.223839 In addition to actual experiences of gender discrimination and biases, the fact that mainstream male surgeons have significantly lower awareness of the existence of such prevalent gender biases and discrimination can further aggravate the discrimination female surgeons experience. Although perceptions are largely influenced by experience, without actual experience, people can form a skewed perception of the inequality and discrimination in society. Raising awareness of gender biases and discrimination among male surgeons will be a crucial step toward addressing gender discrimination in surgery.
An additional adjusted analysis of surgeons with less than 20 years of practice experience showed that in this generally younger group, the experience of gender discrimination decreased, although the difference between the male and female respondents' perceptions of gender discrimination in this group was not significantly different from that of the entire sample. The group with less than 20 years' experience was younger, lower in rank (fellow, instructor, and associate or assistant professor), and included more women than the older group. However, despite the decreased experience of discrimination, younger female surgeons were still more likely to experience gender discrimination than their male counterparts. Moreover, there was no change in the perceptions of discrimination against female surgeons in the younger generation, and the young female surgeons perceived more discrimination than males.
These results imply that despite the increased number of female surgeons and residents, gender discrimination persists, and there is a significant perception gap between male and female surgeons of this discrimination. Although the increase in the number of women in leadership positions suggests the possibility of improving the situation,40 the results of our study imply that simply having more women in the field may not be a fundamental solution. In addition, as Dossa and Baxter41 noted, this strategy will force female surgeons to tolerate various forms of discrimination for the coming decades, and will, eventually, be ineffectual since women will be more likely to leave the surgical field due to the persistent discrimination and disadvantages they will face.
When asked to choose a reason why discrimination persists, both men and women chose performance hindrance due to pregnancy and childbirth as a major reason. However, only female surgeons were acutely aware of general favoritism towards male surgeons as another major causes of persisting gender discrimination, which is consistent with the previous research.15172942 Gender difference was also found in terms of the necessary effort to reduce gender discrimination, where female surgeons were significantly more likely to point out changing the male-dominated culture. A 2019 survey by Shin and Lee33 also found a similar result in which women gave much higher priority to “correcting men-oriented medical practices pattern” as necessary than men did. Such gender differences in the perception of the causes of discrimination and necessary measures to reduce discrimination is evidence that raising male surgeons' awareness of discrimination against women and creating consensus is the beginning of a positive change.
Improving systems, rules, and procedures is important; however, this kind of approach cannot fully address implicit discrimination or “second-generation gender bias,” which refers to practices that may appear neutral but, when applied, discriminate against one gender by reflecting the values of another gender that created or developed the setting. Such second-generation gender bias can become an organizational barrier limiting women from assuming leadership roles.40 Instead, what must be at the center of the efforts to reduce discrimination in surgery is the creation of a culture and climate that are gender-neutral and not easily influenced by any specific groups within the medical community.
This study has some limitations. First, the survey response rate (9.5%) may raise concern about response biases. Although we admit this concern, similar surveys administered to medical professionals such as dentists, physicians, oncologists, etc.434445 through professional associations showed response rates ranging from 10% to 18%. A similar survey of gender equality by Shin and Lee33 recorded a 9.2% response rate. Unlike these examples, the current study sent the survey to all members of the Korean Surgical Society regardless of their practice status, in order to guarantee anonymity and voluntary participation. For this reason, the response rate of the current study may appear relatively lower, but we believe that it is comparable to other similar studies of medical professionals. Second, female surgeons were overrepresented in the sample (29.3%), compared to the national population of women registered with the Korean Surgical Society (8.9%). As highlighted by Rogers et al.,39 a selection bias may have been present in that more women may have responded due to the nature of the study: it is possible that female surgeons are more strongly motivated to express the gender discrimination they have experienced or perceived, whereas male surgeons may be less likely to respond to such surveys. In fact, a significant number of male surgeons expressed the opinion that they felt uncomfortable about the survey topic, and some contested that male surgeons experience reverse discrimination. Finally, the survey queried experiences of gender discrimination throughout the medical and surgery career path; thus, like other self-reported surveys, responses may have been subject to recall bias.
Despite these limitations, this study's major strength is that it covered a wide variety of gender discrimination manifestations, ranging from explicit to implicit forms, and found differences between the genders in both actual experiences and perceptions. The study offers an inclusive description of various forms of gender discrimination in the surgical field and contributes to raising awareness of gender discrimination. It is also the first academic attempt to investigate the current status of gender discrimination across the entire community of surgeons in Korea. The results were generally consistent with prior studies conducted in other countries and can contribute to the generalized understanding of gender biases and discrimination in surgery. While gender discrimination and biases are in and of themselves morally wrong, they are also detrimental to the surgeons who are subject to such discrimination in terms of their personal outcomes. Based on the understanding of the perceptions and experiences of gender discrimination found in this research, future studies can explore how gender discrimination expectations might affect surgeons' professional career choices and attitudes, including job satisfaction, burnout, psychological well-being, and professional confidence. This study only reported the results of aggregated experiences and perceptions of discrimination, whereas the odds ratios of experiences of each discrimination type ranged from 3.4 to 230. Therefore, it is necessary to more closely examine each discrimination type to better understand the wide range of odds ratios despite the very high probability of female surgeons experiencing and perceiving gender discrimination.
Go to :
 XML Download
XML Download