

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute ischemic stroke is a highly time-sensitive disease that requires treatment as quickly as possible. Thrombolysis, which includes intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT), is a crucial treatment for acute ischemic stroke.1 Thrombolysis within the early therapeutic window results in better neurological outcomes and reduced mortality.23 Before thrombolysis can be applied; however, the brain must be imaged to rule out intracerebral hemorrhage. Recent guidelines have recommended brain computed tomography (CT) within 20 minutes of hospital arrival.14
Major efforts have been made to treat acute ischemic stroke more rapidly, and improvements in emergency medical services (EMS) at the prehospital stage play a significant role. Recent treatment guidelines from the American Heart Association/American Stroke Association (AHA/ASA) recommend that EMS conduct prehospital notifications before the arrival of patients with acute ischemic stroke to the appropriate hospitals.5 EMS prehospital notifications can reduce door-to-imaging times and door-to-IVT times for patients with acute ischemic stroke and increase the number of patients eligible for thrombolysis, thereby leading to positive outcomes.6 Telephones have been widely used for prenotification, and EMS have also confirmed whether patients with acute ischemic stroke can be accepted and treated in the contacted hospitals.7
Recently, the use of smartphones has surpassed that of cellular phones. An appropriate mobile app could therefore be a useful means for communicating acute ischemic stroke information between out-of-hospital and in-hospital medical teams. The mobile app can simultaneously deliver necessary information to multiple medical staff and hospitals. In acute stroke treatment that requires multidisciplinary management in a limited time, prenotification through mobile app will play an epochal role in reducing treatment time. We developed FASTroke, a mobile app, which has major roles in identifying suspected stroke patients by EMS personnel, prenotification of suspected stroke patients in nearby treating hospitals, and preregistration of patient's data to facilitate the intra-hospital delivery system. The app was implemented in Daegu, a city in Korea with a population of approximately 2.5 million people. We hypothesized that the prehospital notification system in this app could reduce door-to-CT, door-to-IVT, and door-to-EVT times for patients with acute ischemic stroke.
Go to : 
METHODS
Study design and participants
This study was a retrospective, observational study conducted in Daegu, the fourth largest metropolitan city in South Korea, from February 2020 to January 2021. While 2 regional and 4 local emergency centers operate in Daegu, 5 major hospitals (Kyungpook National University Hospital, Yeungnam University Medical Center, Keimyung University Dongsan Hospital, Daegu Catholic University Medical Center, and Daegu Fatima Hospital) participated in FASTroke project, except for 1 local emergency center that could not perform EVT interventions 24 hours a day, 365 days a year. All 48 fire safety centers including 119 ambulances in Daegu participated in the study. We included adult patients with acute ischemic stroke (aged ≥ 18 years) who experienced the first abnormal symptoms (as perceived by the patient or witness) within 6 hours of being treated by EMS and were transported to the emergency department by ambulance. The study excluded patients who were candidates for reperfusion therapy but were not treated due to their refusal. Patients in the prehospital stage who could not take a stroke screening test due to mental change to predict acute ischemic stroke were also excluded. To compare the management time delay and clinical outcomes, the patients were categorized into FASTtroke prenotification and no FASTtroke prenotification based on the FASTroke app use. FASTroke activation patients were subgrouped according to whether they were preregistered prior to arriving at the hospital.
Mobile application
In December 2019, the Daegu Emergency Medicine Collaboration Committee (DEMCC) developed the FASTroke app as an identification, prenotification, and preregistration system for suspected stroke patients, which can efficiently utilize the regional stroke care system and subsequently improve the quality of acute stroke management. The app was introduced to all major regional emergency departments and fire departments throughout Daegu City. For the FASTroke project as a regional acute stroke care system, DEMCC organized a FASTroke team consisting of specialist physicians in emergency medicine, neurology, and neurosurgery related to treating patients with acute ischemic stroke.
The FASTroke app can be used on iOS and Android systems and is free to download and apply for membership; however, DEMCC administrator approval is required for full membership. The smartphones used by the EMS, hospital stroke team, and emergency department staff were identified and registered individually by the DEMCC. EMS could activate FASTroke at any time in the event of a patient with suspected acute ischemic stroke who is then transferred to the nearest acceptable hospital, in the cases of first abnormal times (FAT, defined as the time elapsed since the first neurological abnormalities were detected) within 6 hours and blood glucose levels of at least 60 mg/dL. If these criteria are met, FASTroke can be activated if one of the symptoms (facial droop, unilateral limb weakness, and dysarthria) is present.8 Next, the patient's name and birth date is entered for hospital preregistration, and the hospital to which the patient is to be transferred is entered. After the EMS sends the information, the hospital's medical staff (stroke team and emergency department) receive notifications through their smartphones to prepare for the patients with acute ischemic stroke and to preregister the patients at the hospital. EMS can also enter the symptom onset time, blood pressure, previous diseases, and medication history, information shared with the hospital's medical staff. If a hospital cannot accommodate patients with acute ischemic stroke due to impossible reperfusion therapy, the hospital's stroke team administrator can register their hospital's nonavailability through the app at any time, preventing the EMS from activating that hospital via FASTroke.
Outcome measurement
After the patient's arrival at the hospital, the following times were measured for the examination and treatment: door-to-CT, door-to-IVT, and door-to-EVT. The door time was defined as the time at reception at the emergency department's entrance, the CT scan time was when the first CT image was taken, the IVT time was when tissue plasminogen activator was injected, and the EVT time was when the catheter puncture procedure was started. For the neurological evaluation, the National Institutes of Health Stroke Scale (NIHSS) was measured at admission and discharge, and the severity of stroke was divided into minor (1–4 points), moderate (5–15 points), moderate to severe (16–20 points), and severe (21–42 points) according to NIHSS score.9 To evaluate the patient's neurological improvement, the difference in NIHSS scores between admission and discharge were calculated.
Data collection
Data of patients with the International Classification of Diseases, 10th Revision, Clinical Modification diagnostic codes I60–I64 were collected from the electronic medical records (EMR) of five hospitals. The diagnostic code input was made through a final diagnosis from an on-duty neurologic specialist. The diagnosis was based on physical examinations and medical imaging results. In total, 119 ambulances reached the hospital and only patients who entered the hospital within the FAT of 6 hours were selected. Information on the selected study group of patients was collected from the EMR of the five hospitals and the 119 run sheets of Daegu.
We retrieved the patients' age, sex, past disease, smoking status, hospital admission time, mental status score, neurological examination, and treatment from their EMR. Arrival at the hospital (also known as door time) is the line that divides the prehospital stage from the hospital stage. The last normal time (LNT) is when the patient was last identified as being normal. The time taken to arrive to the hospital door was recorded based on a combination of FAT and LNT. The transport time, defined as the period between the arrival of the ambulance at the scene and its arrival at the hospital door, was determined from the EMS run sheet.
Statistical analysis
The continuous variables are reported as median and interquartile ranges and were compared using the Mann-Whitney U test and Student's t-test according to its normal/non-normal distribution. Categorical variables are reported as numbers and percentages and were compared using the χ2 test or Fisher's exact test. The associations between baseline characteristics and the use of the FASTroke app with the time spent on management including brain CT, IVT, and EVT were first analyzed using a univariate logistic regression analysis. As recommended by the AHA/ASA guidelines, the door-to-CT time was divided into 20 minutes, the door-to-IVT time was split into 2 parts based on 60 minutes, and the door-to-EVT time was divided into 90 minutes close to the median value in this study.1 To confirm the factors affecting the performance of CT scans and reperfusion treatment within the target time, the following variables were adjusted and analyzed using a multivariable logistic regression analysis: age, sex, previous disease, admission time, NIHSS at admission, and FASTroke use. The results were reported as odds ratios (ORs) and 95% confidence intervals (CIs). The FASTtroke prenotification was categorized by whether prenotification was employed, and the no FASTtroke prenotification was analyzed as a reference value. All statistical analyses were performed using SPSS version 25.0 for Windows (SPSS Inc., Armonk, NY, USA).
Ethics statement
The research protocol was approved by the Institutional Review Board of Kyungpook National University Hospital (2021-06-025) and exempted from prior consent requirements due to the study's retrospective nature.
Go to :
RESULTS
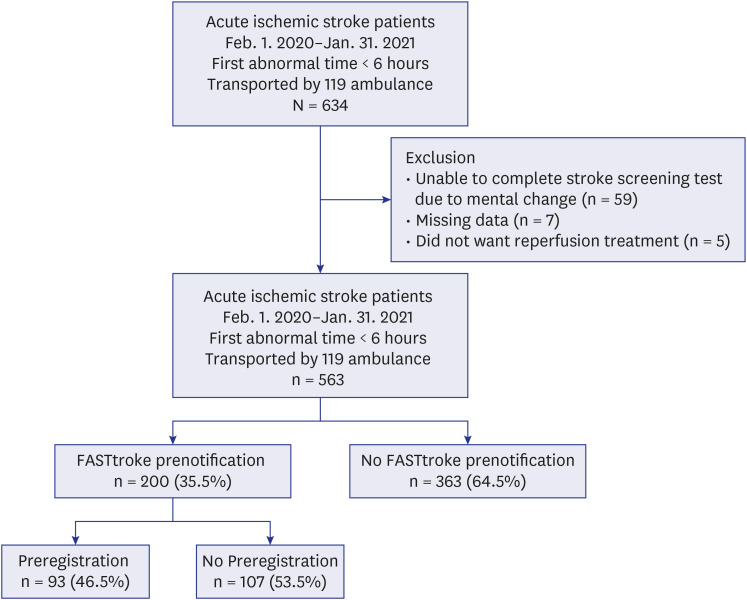
During the study period, 563 patients with acute ischemic stroke within 6 hours of FAT were transported by 119 ambulances to 5 participating hospitals. Of these, the hospitals were prenotified by FASTroke of 200 (35.5%) patients, with 93 (46.5%) preregistered on the way to the hospital (Fig. 1).
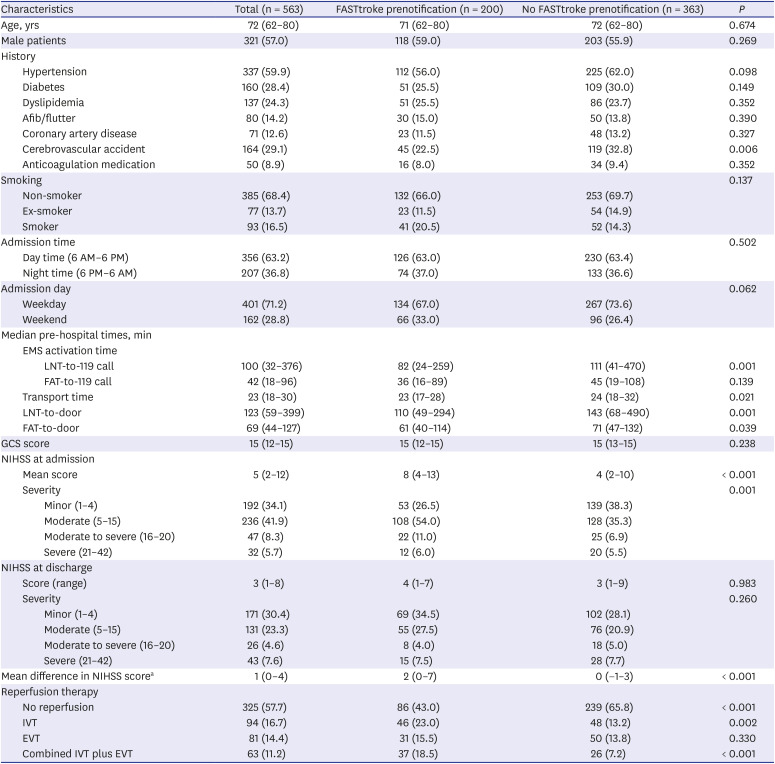
The mean age of the study patients was 72 years, and 321 (57.0%) were male. There was no significant difference in terms of previous illnesses in the use of FASTroke; however, the FASTtroke prenotification had fewer patients with a history of stroke than the no FASTtroke prenotification (22.5% vs. 32.8%, P = 0.006). There was no difference in FASTroke activation between the patients admitted to the hospital at night and those admitted during the day (P = 0.502), and there was no difference between weekday and holiday admissions (P = 0.062). The symptom-onset-to-door time was shorter for the FASTtroke prenotification for LNT and FAT, (LNT-to-door time of 110 minutes vs. 143 minutes, P = 0.001; FAT-to-door time of 61 minutes vs. 71 minutes, P = 0.039), and the transport time from scene to door was also shorter (23 minutes vs. 24 minutes, P = 0.021). The time from LNT to 119 call was short in the FASTroke prenotification group (82 minutes vs. 111 minutes, P = 0.001), but no significant difference was observed with FAT. The FASTtroke prenotification had a higher mean NIHSS score at admission (8 vs. 4, P < 0.001), as well as a higher difference value (the difference in scores between admission and discharge) than the no FASTtroke prenotification (2 vs. 0, P < 0.001). In terms of reperfusion therapy, the rates of IVT treatment alone and IVT combined EVT treatment were higher in the FASTtroke prenotification (IVT 23.0% vs. 13.2%, P = 0.002; combined IVT plus EVT 18.5% vs. 7.2%, P < 0.001). However, the rate of EVT alone did not significantly differ (15.5% vs. 13.8%, P = 0.330) (Table 1, Fig. 2).
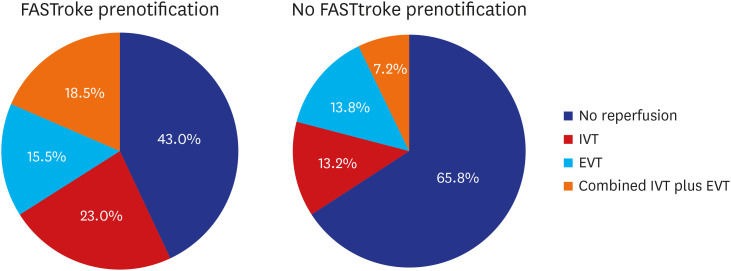 | Fig. 2Differences in perfusion therapy according to the use of FASTroke prenotification.IVT = intravenous thrombolysis, EVT = endovascular thrombectomy.
|
Table 1
Demographic and clinical characteristics
Values are presented as number (%) or number (range).
Afib = atrial fibrillation, EMS = emergency medical services, LNT = last normal time, FAT = first abnormal times, GCS = Glasgow Coma Scale, NIHSS = National Institute of Health Stroke Scale, IVT = intravenous thrombolysis, EVT = endovascular thrombectomy.
aDifference in NIHSS score between admission and discharge.
![]()
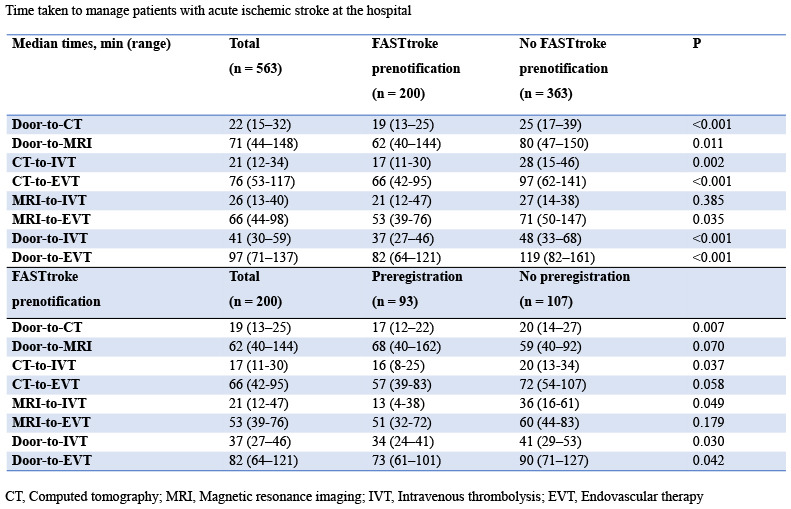
In the hospital, FASTtroke prenotification had shorter door-to-CT (19 minutes vs. 25 minutes, P < 0.001) and door-to-magnetic resonance imaging (62 minutes vs. 80 minutes, P = 0.011) scan times, and shorter CT-to-IVT (17 minutes vs. 28 minutes, P = 0.002) and CT-to-EVT (66 minutes vs. 97 minutes, P < 0.001) times. Thus, door-to-IVT (37 minutes vs. 48 minutes, P < 0.001) and door-to-EVT (82 minutes vs. 119 minutes, P < 0.001) times were faster in FASTroke prenotification. In FASTtroke prenotification, the preregistered patients had shorter performance times, door-to-CT times (17 minutes vs. 20 minutes, P = 0.007), and door-to-reperfusion times (IVT 34 minutes vs. 41 minutes, P = 0.030; EVT 73 minutes vs. 90 minutes, P = 0.042) than the nonregistered patients (Table 2).
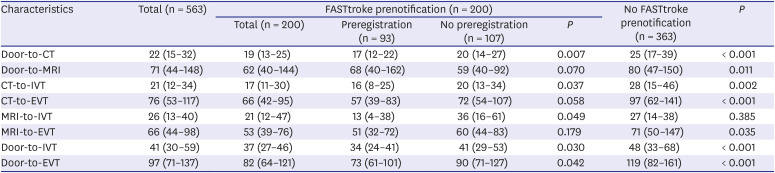
Table 2
Time taken to manage patients with acute ischemic stroke at the hospital
Values are presented as median times (range; unit: minutes).
CT = computed tomography, MRI = magnetic resonance imaging, IVT = intravenous thrombolysis, EVT = endovascular thrombectomy.
![]()
Table 3 shows the results of the multivariable logistic regression analysis after dividing the patients with acute ischemic stroke into groups by target time spent on CT, IVT, and EVT (CT 20 minutes; IVT 60 minutes; EVT 90 minutes). The results of the analysis were as follows. FASTroke and no preregistration (adjusted OR, 1.88; 95% CI, 1.19–2.96; P = 0.006), FASTroke and preregistration (adjusted OR, 3.35; 95% CI, 2.04–5.53; P < 0.001), previous history of stroke (adjusted OR, 0.58; 95% CI, 0.39–0.86; P = 0.007), and NIHSS at admission (adjusted OR, 1.03; 95% CI 1.00–1.06; P = 0.016) were independent factors affecting the time to brain CT scan. The factors affecting the door-to-IVT time were FASTroke with preregistration (adjusted OR, 5.56; 95% CI, 1.29–23.93; P = 0.021), previous history of stroke (adjusted OR, 0.23; 95% CI, 0.08–0.73; P = 0.012), and anticoagulation medication (adjusted OR, 0.07; 95% CI, 0.01–0.55; P = 0.012). The factors affecting the door-to-EVT time were FASTroke with preregistration (adjusted OR, 6.73; 95% CI, 2.53–17.87; P < 0.001) and NIHSS score at admission (adjusted OR, 1.12; 95% CI, 1.05–1.19; P < 0.001).
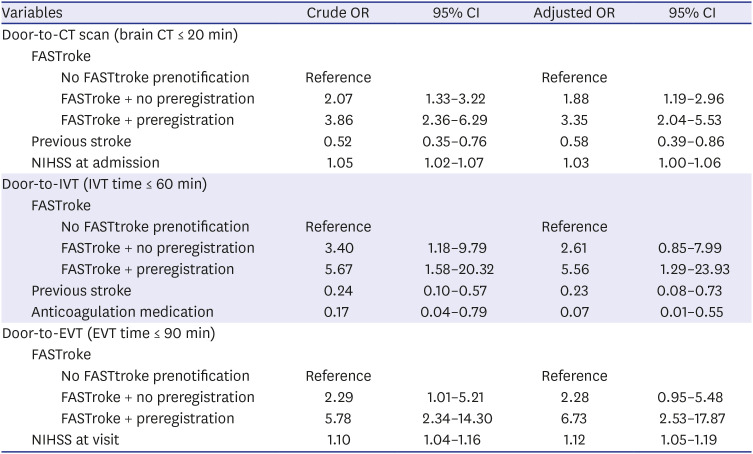
Table 3
Multivariate regression analysis of factors affecting the time to management of acute ischemic stroke
Adjusted variable: age, sex, hypertension, diabetes, dyslipidemia, atrial fibrillation/flutter, coronary artery disease, cerebrovascular event, anti-coagulation medication, visit time, visit day, NIHSS at visit, FASTroke use.
OR = odds ratio, CI = confidence interval, CT = computed tomography, NIHSS = National Institute of Health Stroke Scale, IVT = intravenous thrombolysis, EVT = endovascular thrombectomy.
![]()
Go to :
DISCUSSION
In this study, EMS prenotification of patients with acute ischemic stroke using the FASTroke app showed major time savings in patient management. Door-to-CT-scan times decreased by 6 minutes, door-to-IVT times by 11 minutes, and door-to-EVT times by 37 minutes. There were additional time savings for in-hospital management of patients with acute ischemic stroke when the hospitals performed preregistration.
Acute ischemic stroke is highly time-sensitive, with neurons dying at a rate of 1.9 million/min; prompt management is crucial.10 Numerous attempts have been made to reduce the delay in treating acute ischemic stroke, including the Helsinki model, which led to improved patient outcomes.1112 The time to CT scan, the time to treatment decision, and the time to injection of a thrombolytic drug improved in patients with acute ischemic stroke prenotified by EMS.1314 Our study reported a 5-minute reduction in the door-to-CT time and a 2-minute reduction in the door-to-IVT time as a result of prenotification.6 Our study showed a breakthrough time reduction of 8 minutes in the door-to-CT time, 14 minutes in the door-to-IVT time, and 46 minutes in the door-to-EVT time for the FASTroke preregistered group compared with no FASTtroke prenotification.
Studies have recently been conducted to remotely check the clinical aspects, data, and scans of patients through smartphones to provide better treatment for patients with acute ischemic stroke.151617 Despite the limitations of small-scale research conducted in a single hospital, a recent study showed a reduction in door-to-needle times of 40 minutes using a mobile app in the prehospital setting.18 Consistent with prior studies, these results were confirmed in our study in a metropolitan setting; when the FASTroke app was activated, the percentage of patients who received reperfusion treatment was 9.8% higher for IVT alone and 11.3% higher for IVT plus EVT treatment. The median door-to-IVT time was 11 minutes shorter compared to those who did not activate the app. Further time savings were also achieved through hospital preregistration.
There are a number of limitations to using non-smart cell phones for prenotification in the prehospital stage. First, it is difficult to check the nearby hospital's capacity for accommodating patients with acute ischemic stroke in real-time with older phones. With cell phones, communication is only possible one-on-one, and EMS might encounter difficulties determining in advance whether a hospital's medical staff are busy or unable to answer the phone. With one-on-one calls, the hospital's medical staff needs to contact all stroke teams individually after receiving the EMS prenotification. By using the FASTroke prenotification app, EMS can immediately identify the hospitals that can accommodate patients with acute ischemic stroke. Once the code has been activated by the FASTroke app, all stroke team staff at the receiving hospital will be simultaneously informed by smartphone notifications. Hospitals that receive FASTroke prenotification can respond with a variety of procedures to manage patients more quickly. Special beds for patients with acute ischemic stroke can be prepared before the initial examination. Nurses can be ready to access blood vessels at the entrance, and tissue plasminogen activator can be prepared for administration the moment the patient arrives. Radiologists can prepare CT rooms for the rapid imaging of patients with acute ischemic stroke, and neurologists can accompany patients to all tests until the diagnosis. For reducing treatment time, EMS prenotification is essential, as is the standing by of various hospital medical staff, such as radiologists, neurologists, and emergency physicians, for the patients' arrival.19
Preregistration shortens the reception time after hospital arrival. Hospital registration numbers can be prepared in advance by the EMS entering the patients' names and resident registration numbers into the FASTroke app. The stroke team doctor who receives the FASTroke preregistration notification can order the necessary examinations before the patients are admitted to the hospital. The time required to register for tests is thereby shortened, preregistered patients are indicated with unique markings on the electronic medical patient list and are recognized by all medical staff in the emergency room, enabling faster management.
Several measures have been taken to facilitate FASTroke. We consider that it is not easy for the EMS to predict acute ischemic stroke based on the patient's symptoms alone at the prehospital stage. To judge these symptoms, patients with altered consciousness who could not clearly express their symptoms were excluded from the activation indications of the FASTroke. Although some patients with acute ischemic stroke may get excluded through this exclusion criterion, activating the FASTroke system in patients with numerous changes in consciousness or vague neurological symptoms may produce high false positives and exhaust the medical staff. An additional sign, hypoglycemia, a condition that could be ruled out immediately at the rescue scene to reduce false positives, was a prerequisite for FASTroke activation (blood glucose level > 60 mg/dL). A total of 512 patients were FASTroke activated during the study; of these, 312 were not enrolled. However, among the 312 not-enrolled patients, 58 were excluded with an ischemic stroke with a FAT over 6 hours, 126 with a hemorrhage stroke, and 12 with a transient ischemic attack. In other words, 116 patients (22.7%) had FASTroke alarms due to non-stroke diseases. These prediction results appear to be no different from a previously used prehospital stroke scale.20
Acute ischemic stroke can occur anywhere, and patients must be treated quickly and safely. However, communication between EMS and hospitals is limited, and it is not easy to know in real-time treatable operating conditions. Therefore, from the perspective of a regionalized emergency medical system, communication and cooperation between the prehospital EMS and hospital medical staff is essential.21 The FASTroke app allowed confirmation of acceptance in 24-hour hospital acute care and allowed conversations about the patient state between EMS and hospital medical staff. As a result, an effective regional collaboration system was constructed through the FASTroke app. To the best of our knowledge, there has been no study of the regional-sized pre hospital stage prenotify and communication through an app, and the results of this study are considered to be very meaningful.
A variety of factors affect the treatment of patients with acute ischemic stroke, including age, sex, underlying diseases, initial NIHSS scores, area of residence, transportation method, and time of onset.3422 In this study, higher NIHSS scores at admission resulted in a greater likelihood of the CT scan being performed within 20 minutes, and patients with a history of stroke had shorter door-to-scan times. The higher the NIHSS score at admission, the shorter the door-to-EVT times. An IVT performed within 60 minutes was less frequent for those with underlying diseases such as a previous stroke and anticoagulant medication. NIHSS is a critical factor in the prognosis of patients with acute ischemic stroke,2324 with higher scores indicating more prominent neurological symptoms, thereby enabling medical staff to recognize patients with acute ischemic stroke, activating FASTroke for faster treatment. In contrast, patients with previous underlying disease, especially those who have had a stroke, are difficult to distinguish from those with existing neurological symptoms, and predicting acute ischemic stroke is not easy. We assumed that these patients had infrequent FASTroke activation and relatively slow management.
This study had several limitations; the first was its retrospective nature, with the factors inherent in retrospective data collection, analysis, and interpretation. Second, the use of the FASTroke app and preregistration was not applied consistently. Although there were indications for FASTroke activation, FASTroke was used according to the prediction of acute ischemic stroke and the preference report form of the dispatched EMS. In addition, preregistration was applied differently depending on the circumstances of the hospital and medical staff. Third, given that the research period included the coronavirus disease 2019 pandemic period, EMS hospital treatment might have been restricted; however, the effect of the pandemic on this study could not be jointly analyzed. We confirmed in a previous study that the examination and treatment of patients with acute ischemic stroke at the hospital stage were not affected much during the pandemic.25 Fourth, due to its short follow-up period, this study could not determine the patients' long-term outcomes. Fifth, reperfusion therapy is performed according to current guidelines. However, neurologists may be biased in determining reperfusion due to multiple factors such as age and previous illness history and performance. The above limitations will be fully considered and improved in future research.
In conclusion, the FASTroke app is a useful tool in building a stroke care system for prenotification in a metropolitan area. In FASTroke prenotification, the transport time of acute ischemic stroke patients was shortened, and the proportion of reperfusion treatment was increased. The FASTroke app for patients with acute ischemic stroke helped reduce management times, such as door-to-brain-CT, door-to-IVT, and door-to-EVT. In particular, the app was most effective when the hospital conducted joint preregistration.
Go to :
 XML Download
XML Download