

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
E-cigarettes (EC) are devices that either vaporize a nicotine solution with liquid flavors or heat-not-burn the ends of cigarettes. Since their introduction in 2004, EC have been considered a smoking cessation aid or alternative to conventional cigarettes (CC) to reduce smoking. However, e-cigarette or vaping use-associated lung injuries (EVALIs) have developed in the United States, and as of February 2020, a total of 2,807 hospitalized EVALI cases and 68 deaths have been reported.1 In response, the US Food and Drug Administration (FDA) announced a ban on selling EC and has begun to prepare guidelines to control marketing of EC.
In Korea, the market for cigarette-type EC is estimated to be US $1.67 billion (approximately 1.97 trillion won). In Korea, the heat-not-burn type of EC is more popular; Korea was the world’s second largest market for IQOS in 2017.2 It was reported that about 7% of all adult smokers use EC, and younger generations are more attracted to EC. About 10% of smokers under the age of 18 years had experience with EC, 15% of males and 3% of females, which is higher than the rates among adults.3 The health outcomes of EC use has been debated. Generally, EC use was associated with poorer health outcomes, but quality of life is different depending on accompanied CC use.4 As the number of reported EVALI cases increased rapidly in the US, the Ministry of Health and Welfare of Korea strongly recommended against the use of liquid-type EC from October 2019.5 In Korea, one case of suspected EVALI was reported after the recommendation to refrain from using liquid type EC and the operation of the monitoring system for suspected cases had been introduced since then.6
Formal diagnostic criteria for EVALI have not been agreed upon, EVALI is based on lung opacities on chest image with use of ECs or related product in the previous 90 days and require particular attention to the exclusion of lung infection and other causes of respiratory failure such as heart failure and rheumatologic disease.7 Considering the heterogeneous presentations suggesting EVALI and unawareness of this illness among doctors other than pulmonologists, uncounted cases of EVALI might exist in Korea. The National Health Insurance Service (NHIS) is the sole provider of financial coverage for medical care for the entire population in Korea. We tried to identify uncounted cases of EVALI using data linkage between the Korean National Health and Nutrition Examination Survey (KNHANES) and the NHIS administrative claims database.
Go to : 
METHODS
Study population and data sources
This study analyzed data from the KNHANES, which is a nationwide survey that has been conducted periodically by the Korea Centers for Disease Control and Prevention (KCDC) to investigate the health status of the South Korea population using interviews about health and nutrition and a basic health assessment. Participants are chosen by proportional allocation-systematic sampling with multi-stage stratification using age, sex, residence type, education level, and other variables. The KNHANES comprises well-sampled data representing the entire Korean population. The NHIS is a sole provider of the health insurance system that covers the entire South Korean population. Nearly all Korean citizens are enrolled in NHIS, and they are categorized as insured employees, insured self-employed individuals, or medical aid beneficiaries. The NHIS dataset includes all inpatient and outpatient medical claims and the corresponding codes for diagnoses and treatment procedures.8
We used data collected by the VI (2013–2015), VII (2016–2018), and VIII-1 (2019.1–2019.9) KNHANES in conjunction with the NHIS administrative claims database. All data in the present study were anonymized fully prior to assessment. We intended to investigate the occurrence of severe pneumonia according to EC use by linking the KNHANES, which provides smoking history, with the NHIS claims database, which provides disease codes and inpatient medical claims. This information is available on the KCDC (http://knhanes.cdc.go.kr/knhanes/eng/index.do) and National Health Insurance Sharing Service websites (http://nhiss.nhis.or.kr).
Study outcomes and definitions
Endpoints
The primary endpoint of this study was diagnosis of severe pneumonia requiring hospital admission according to EC use during the study period. The secondary endpoints of this study were in-hospital mortality, intensive care unit (ICU) admission, ventilator care, and hospital stay in days.
Identification of acute severe pneumonia requiring hospital admission
An acute EC-related severe pneumonia case was defined as pneumonia development requiring hospital admission within 3 months of the survey on smoking. The definition of pneumonia based on the International Classification of Disease, Tenth Revision (ICD-10) includes the following codes: J12.x, J15.x, J16-J17, J18.x, J67.x, J68.x, J69.1, J70, J70.9, J80, J96.x, J96.9.x, and J98.x. Payment claims for ICU care were defined as the presence of one of these procedure codes for intensive care: AJ001–003, AJ100, AJ200, AJ300, and AJ500; ventilator care was defined as the presence of one of these procedure codes for ventilator care: M5830, M5850, M5867, M5858, M5860, and M5859, according to the Healthcare Common Procedure Coding system codes provided by the Health Insurance Review and Assessment service.
Smoking status
Those who had smoked fewer than 100 cigarettes (5 packs of cigarettes) in their lifetime were categorized as non-smokers.9 All participants were asked if they had used EC in their lifetime. Those who had used EC in the previous month were categorized as “current EC user.” Those who had experience with EC but had not vaped in the previous 30 days were categorized as “former EC user.” We aimed to investigate the influence of current smoking on acute pneumonia; therefore, former EC users were categorized as non-EC users; current CC users, current EC users, and current users of both CC and EC were categorized as CC users, EC users, and dual users, respectively.
Sociodemographic status and comorbidities
Sociodemographic variables included age, sex and other factors. Household income level was divided into national quartiles (lowest quartile, lower-middle quartile, upper-middle quartile, and highest quartile). Education level was categorized as less than elementary school, middle school, high school, and college or higher. Comorbidities included self-reported physician diagnosis of asthma, chronic obstructive pulmonary disease (COPD), hypertension (HTN), diabetes mellitus (DM), and malignancy in the KNHANES. The Charlson Comorbidity Index (CCI) was used to assess disease severity by assigning weights according to type of comorbidity for a total of 17 diseases. The CCI is classified as mild for scores of 0, moderate for scores of 1–2, and severe for scores ≥ 3.10
Statistical analysis
Clinical characteristics were compared between EC users and non-users using Student’s t-test for continuous variables and the χ2 test or Fisher’s exact test for categorical variables. All tests were two-sided, and differences were considered statistically significant at a significance level of 0.05. All statistical analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC, USA) and R software (version 3.6.3; R Statistical Foundation of Computing, Vienna, Austria).
Ethics statement
This population-based cohort study was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.11 The study was approved by the Institutional Review Board of The Catholic Medical Center (XC20ZNDI0007). Informed consent was waived because data analysis was performed retrospectively using anonymized data derived from the KNHANES in South Korea.
Go to :
RESULTS
Distribution of smoking behaviors in KNHANES participants by year
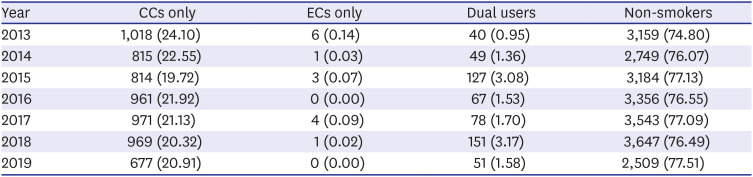
We identified 47,076 KNHANES participants from January 2013 to September 2019. Of these, 9,023 participants younger than 19, 1,336 participants who did not participate in the smoking-related questionnaire, and 7,767 former CC users were excluded (Fig. 1). Finally, 28,950 subjects were analyzed. The prevalence of current, sole EC users did not increase during the study period (Table 1).
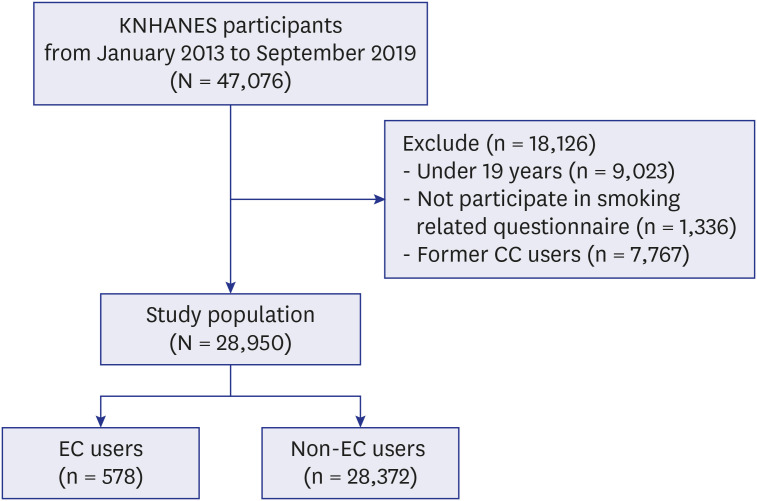 | Fig. 1Flow chart of the study population from KNHANES in the Republic of Korea.KNHANES = Korean National Health and Nutrition Examination Survey, CC = conventional cigarette, EC = e-cigarette.
|
Table 1
The distribution of smokers according to type of cigarettes in KNHANES from January 2013 to September 2019
Values are presented as number (%).
KNHANES = Korean National Health and Nutrition Examination Survey, CC = conventional cigarette, EC = e-cigarette.
![]()
Clinical characteristics
Of all participants, 578 (2.0%) were EC users, and 28,372 (98.0%) were non-EC users. The proportion of males was higher, but mean age and body mass index (BMI) were lower for EC users. The EC users showed a higher proportion of upper middle and highest quartiles of household income, and higher education level, but a lower proportion of comorbidities such as HTN, DM, and malignancies, with a high comorbidity index of 3 or more (Table 2).
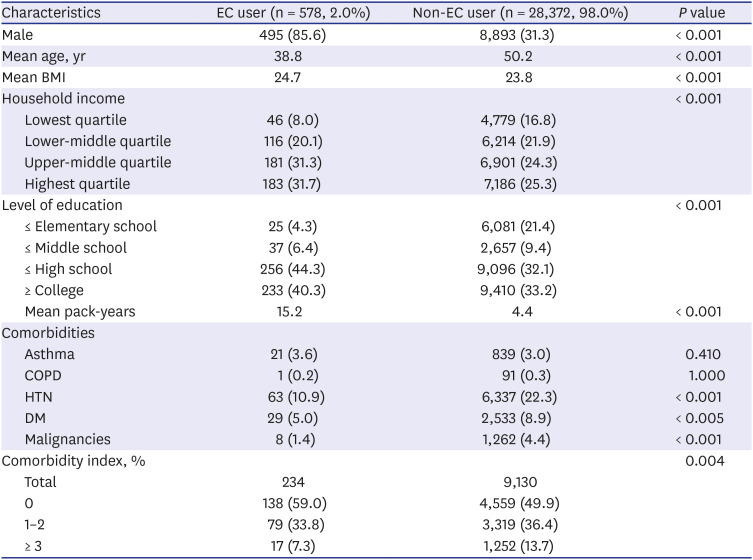
Table 2
Clinical characteristics of Korean adults (≥ 19 years) according to EC use in KNHANES (n = 28,950)
Values are presented as number (%) unless otherwise indicated.
KNHANES = Korean National Health and Nutrition Examination Survey, EC = e-cigarette, BMI = body mass index, COPD = chronic obstructive pulmonary disease, HTN = hypertension, DM = diabetes mellitus.
![]()
Clinical outcomes
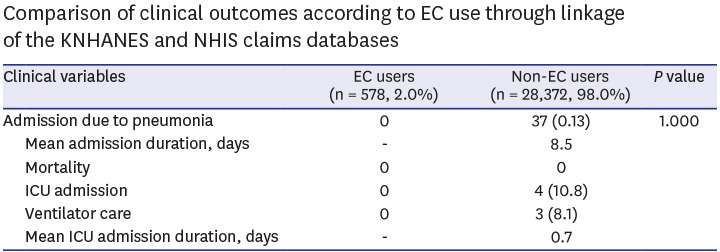
We compared severe pneumonia occurrence requiring hospital admission and clinical outcomes of pneumonia according to EC use. In the KHANES-NHIS data linkage, there were no occurrences of severe pneumonia among EC users, while 37 severe pneumonia cases were noted among non-EC users. The incidence of pneumonia occurrence was not different between the two groups (P = 1.000). In patients with severe pneumonia, the mean admission duration was 8.5 days, the rate of ICU admission was 10.8%, that of ventilator care was 8.1%, and mortality was 0.0% (Table 3).
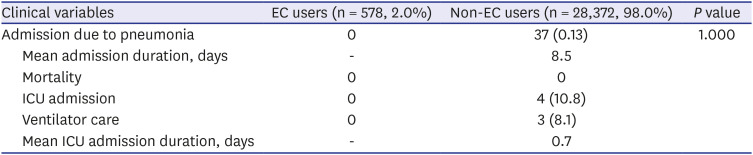
Table 3
Comparison of clinical outcomes according to EC use through linkage of the KNHANES and NHIS claims databases
Values are presented as number (%) unless otherwise indicated.
EC = e-cigarette, KNHANES = Korean National Health and Nutrition Examination Survey, NHIS = National Health Insurance Service, ICU = intensive care unit.
![]()
Go to :
DISCUSSION
To investigate the effects of EC use on occurrence of acute severe pneumonia, data from the KNHANES were linked with NHIS claim data to confirm the occurrence of EC-related pneumonia and the clinical outcomes and smoking history of patients. In the data linkage between KNHANES and the NHIS claims database, there were 578 (2.0%) current EC users and 28,372 (98.0%) non-EC users. The proportion of males, household income, and education level were higher, however, mean age and comorbidities were lower among EC users. No severe pneumonia cases occurred among EC users, and the incidence of pneumonia occurrence was not different between EC users and non-EC users (P = 1.000).
Few population studies have examined the association between EC use and pneumonia development before the recent outbreak of EVALI in the US. Tobacco and related products are evolving rapidly in diversity and are marketed aggressively in many countries. The impact of exposure to traditional tobacco smoke on lung health has been documented well. However, EC and vaping use present new challenges to clinicians.12 Even though EC are promoted as a less harmful alternative to CC, there is growing evidence that EC use is associated with increased risk of chronic respiratory diseases including chronic bronchitis, emphysema, COPD, and asthma.1314 The potential mechanisms for the association of EC use and chronic respiratory disease include pulmonary inflammation, altered immune response, and increased oxidative stress.15
In particular, due to the outbreak of EVALI in the US, interest in EC-related lung health is increasing. The Centers for Disease Control and Prevention and the US FDA have investigated causes of the EVALI outbreak that occurred in August 2019. As of February 25, 2020, a total of 2,807 hospitalized EVALI cases and 68 deaths had been reported.1 Vitamin E acetate, an additive in some tetrahydrocannabinol (THC)-containing EC, was strongly linked with EVALI, although the contribution of other chemicals, in either THC or non-THC-containing products, was not ruled out.16 Further, nicotine salts, coconut oil, and limonene were considered potential causes of EVALI.1718 Bronchoalveolar lavage fluid of EVALI patients has shown lipid-laden macrophages that were also observed in a raft of disease including lipoid pneumonia, amiodarone toxicity, and aspiration.219
We found that the acute severe pneumonia did not occur within 90 days of EC use in Korean population. These findings are contrary to the results of previous studies that have reported hazards of EC.2021 This discrepancy is probably due to differences in composition and content of harmful ingredients. According to the analytical results of suspected harmful components in domestic liquid EC released in December 2019, THC was not detected in the liquid EC distributed in Korea, and very trace amounts of vitamin E acetate, which was identified as the main cause of EVALI in the US, were detected. For vitamin E acetate, the detection range of liquid EC for EVALI patients used by the US FDA is 230,000 to 880,000 ppm. However, the detected concentration in products in distribution in Korea reported by the Ministry of Food and Drug Safety was 0.1 to 8.4 ppm, which corresponds to trace amounts compared to those in the US.22 Vitamin E acetate is an oily chemical added to THC vaping liquids to thicken or dilute them.23
A lower prevalence of EC use in Korea compared to the US and Europe might have contributed to the absence of EC-related severe pneumonia in Korea. As of 2018, the prevalence of ever-users and current users of EC in Korea was 11.2% and 4.3%, respectively.24 Similarly, the prevalence of ever-users of EC in Europe and the US was 11.6% and 12.6%, respectively.2526 In Korea, the proportion of current EC users remained constant from 2013, but that of dual users increased in 2015 and 2018. These changes in smoking behavior could be explained by the increase in the price of CC from 2,500 KRW to 4,500 KRW as a result of anti-smoking policies in Korea and the introduction of IQOS, a cigarette type of EC, in 2017.2728 CC users might think that EC pose a lesser risk than CC and might consider EC to be an effective harm reduction strategy or attractive alternative to stop or reduce cigarette smoking.29 Furthermore, EC are becoming increasingly popular among adolescent cigarette users, and a potential increase in dual use among adolescents is expected in Korea. Even though there were no cases of severe pneumonia related to EC use during the study period, but harmful effects of EC cannot be completely excluded. For these reasons, government should maintain EC regulation policies and continuously monitor the hazards of EC.
There were several limitations to this study. When EC-related severe pneumonia was defined, the ICD-10 codes included bacterial pneumonia and viral pneumonia, so the possibility could not be excluded that it included pneumonia due to other causes than severe EVALI. Second, there was no distinction between liquid-type and cigarette-type EC in the smoking-related questionnaire in the KNHANES survey prior to 2018, so there was a limit in analyzing the effects of liquid-type EC, which were the cause of EVALI in the US. Third, the peak of the EVALI outbreak in the US was from June 2019 to September 2019, but the claims data available in this study were from January 2013 to June 2019, a period that ended just before the report of the EVALI epidemic. Fourth, because we focused on acute severe pneumonia requiring hospital admission, mild diseases such as pneumonia not requiring hospital admission, bronchitis, COPD, asthma, or chronic pneumonia induced by smoking might have been neglected. Finally, the number of EC users was too small, and the baseline characteristics including age, comorbidities and socio-economic status that can affect the occurrence of pneumonia were significantly different between EC and non-EC users.
Despite these limitations, the strength of our study is that it was based on a large and representative national database and an administrative claims database, which are useful for identification of severe pneumonia requiring hospital admission according to types of smoking.
In conclusion, we conducted a retrospective analysis using linkage of data between the KNHANES and the NHIS claims databases to investigate the effects of EC use on acute severe pneumonia. Since EVALI is most likely included in acute severe pneumonia occurring within 3 months of EC use, it is considered that there might be no EVALI patients in Korea during the investigation period. In the current situation of increasing popularity of ECs, a large-scale prospective study is necessary to evaluate the effect of EC use on development of acute lung injury.
Go to :
 XML Download
XML Download