

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD) refers to a disease in which blood circulation is impaired in the heart muscle due to narrowing or blockage of the lumen in the coronary artery. Drug-eluting stents (DESs) have recently been used to treat this disease.1)2) DES refers to a coronary artery stent coated with an immunosuppressant such as sirolimus or everolimus or a cell proliferation inhibitor to suppress restenosis on a bare-metal stent (BMS).3)4)
The first-generation DES, Cypher (Cordis, Santa Clara, CA, USA), significantly reduced in-stent restenosis compared to BMSs that had previously been used as sirolimus-eluting stents.3) Since then, second-generation drug-releasing stents, such as Xience V (Abbott, Sligo, Ireland) and Endeavor (Medtronic, Dublin, Ireland) stents, have been developed with various eluting drugs and stent platforms. Recently, it has been coated with biodegradable polymers to improve thrombosis and performance.5)6)7) Nowadays, SYNERGY™ (Boston Scientific, Marlborough, MA, USA), XIENCE Sierra™ (Abbott Vascular, Green Oaks, Illinois, USA), Orsiro (Biotronik, Bülach, Switzerland), and BioMimestents (Meril Life Sciences, Gujarat, India)) are used clinically as third-generation DESs with a blood-compatible polymer coating.8)
DESs are still reported to lead to very late stent thrombosis in which blood clots occur within the stent more than 1 year after stent insertion. Since stent thrombosis has a high mortality rate, its prevention is clinically important.9) The causes of stent thrombosis include delayed endothelialization, early cessation of antiplatelet drugs, hypersensitivity reaction of DESs to polymers, resistance to antiplatelet drugs, and lesion patterns branched lesions, and presence of risk factors such as diabetes and kidney failure.10)11)
To prevent stent thrombosis, the coated polymer used in the stent should be minimized, and after the drug is eluted, it is completely degraded, and only the metal stent only in the body. Also, inflammation caused by polymer degradation should be reduced.
D+Storm™ DES is a sirolimus-eluting stent coated with polylactic acid (PLA), sirolimus, and ascorbic acid, which is expected to reduce restenosis and inflammatory reactions. Although sirolimus, an anti-proliferative drug, inhibits the growth of smooth muscle cells (SMCs) to inhibit neointimal proliferation, the growth of endothelial cells (ECs) must be promoted to prevent late thrombosis. Ascorbic acid is one of the drugs known to be effective in promoting the growth of ECs, inhibiting the growth of SMCs and increasing the production of nitric oxide.12)13) Vascular ECs are inhibited by tumor necrosis factor (TNF), which may affect atherosclerosis. In the cell experiment, ascorbic acid effectively blocked the growth inhibition and apoptosis of TNF-mediated vascular ECs, and ascorbic acid alone increased the growth of ECs.14) Ascorbic acid may also reduce oxidative stress and inflammation of the entire vessel wall in inflammatory conditions such as cardiovascular disease.12)13)
The objective of the present study (in vitro) was to evaluate a biodegradable poly-L-latic acid-based sirolimus coated stent in comparison with a commercial everolimus-eluting stent with a permanent polymer in a porcine coronaty restenosis model on a short-, mid-, and long-term basis.15)
In this first-in-man study, D+Storm™ DES and BioMatrix Flex™ DES were compared in terms of their safety and efficacy.
Go to : 
METHODS
Ethical statement
This protocol was approved by the Institutional Review Board of 5 medical institutions: Seoul National University Hospital (D-1608-029-783), Hanyang University Medical Center (HYUH 2016-08-016-033), Yonsei University Wonju Severance Christian Hospital (CR216014), Gachon University Gil Medical Center (GOIRB2017-286), and Korea University Anam Hospital (MD17017). Written informed consent was acquired from all subjects.
Patient population
This pivotal study is a prospective, multicenter, subject single-blind, randomized clinical study conducted from March 2017 to April 2019 to compare the safety and efficacy of the D+Storm™ DES and BioMatrix Flex™ DES. Of the patients with CAD in 5 institutions, 112 patients scheduled for one-vessel percutaneous coronary intervention (PCI) were enrolled for this study. Among the patients aged 20–80 years diagnosed with stable angina, unstable angina, silent ischemia, and non-ST-elevation myocardial infarction, those who meet the criteria of stenosis >50% on angiography, reference vessel diameter 2.25–4.0 mm, lesion length ≤40 mm, and thrombolysis in myocardial infarction flow behind the lesion ≥ grade 1 were selected as subjects in this study. Patients with ST-elevation myocardial infarction (STEMI), cardiogenic shock, chronic total occlusion, restenosis lesion, left main CAD, graft vessel lesion, systemic bleeding, and coagulation disorders, and those who contraindicated to antiplatelet drugs (such as aspirin, clopidogrel, heparin, sirolimus, biolimus A9) were excluded. Additionally, patients with intracranial bleeding within 6 months before participation in clinical trials and patients who underwent DES, drug-eluting balloon, and BMS procedures within 12 months before participation in clinical trials were excluded from this study.
Drug-eluting stent (D+Storm™ drug-eluting stent and BioMatrix Flex™ drug-eluting stent)
D+Storm™ (CG Bio Co., Ltd., Seoul, Korea) and BioMatrix Flex™ (Biosensors Interventional Technologies Pte, Ltd., Singapore) were applied to the investigational group and comparator group, respectively. D+Storm™ DES is a coronary stent made of cobalt-chromium (Co-Cr) material that elutes sirolimus to treat CAD. D+Storm™ DES platform is a waved semi-open cell type. It is flexible even in complex and curved blood vessels due to its S-shaped and symmetrical strut (thickness; 70 μm). It is remarkably flexiblein that it enables smooth movement and allows radial force that secures space by supporting constricted lesion vessels. In addition, recoil and foreshortening, which are important for accurate positioning of the stent.
D+Storm™ DES is coated at a thickness of 5 μm with sirolimus (1.4 μg/mm2) and PLA carrier, a biodegradable polymer. To minimize systemic exposure of sirolimus, only the stent's abluminal side was coated (abluminal top coating). BioMatrix Flex™ DES was selected as a comparator group in this study for the following reasons. BioMatrix Flex DES is a stent for coronary artery, and like D+Storm™ DES, it is coated using PLA, a fully biodegradable polymer. In addition, the drug coated on BioMatrix™ Flex DES is Biolimus A9, which is a lipophilic derivative of Sirolimus coated on D-Storm™ DES. (Table 1).15)
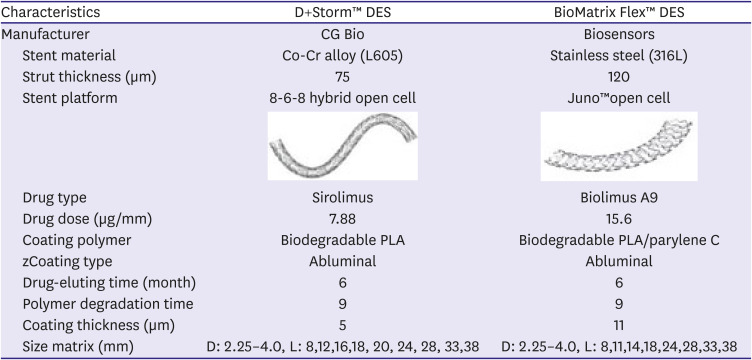
Table 1
Technical characteristics of D+Storm™ and BioMatrix Flex™ DES stent


![]()
Study procedure
Before the intervention procedure, oral dual antiplatelet therapy formulations (aspirin; 300–325 mg and clopidogrel; 300–600 mg, prasugrel; 60 mg, ticagrelor; 180 mg) were administered at a recommended loading dose at the discretion of the investigator, and additional antiplatelet agents such as cilostazol were administered, if necessary. Heparin was administered at a dose that could allow the acceleration time to be maintained at an appropriate level (≥250–300 seconds) during the procedure according to the guidelines. Glycoprotein IIb/IIIa inhibitors (abciximab, tirofiban) were administered according to the operator's clinical judgment. Dual antiplatelet therapy was performed daily in combination with aspirin (75–300 mg/day) after intervention (clopidogrel; 75 mg/day, prasugrel; 10 mg/day, ticagrelor; 180 mg/day). The combination therapy was based on the following 2 guidelines: 2011 American College of Cardiology Foundation (ACCF)/American Heart Association (AHA)/Society for Cardiovascular Angiography and Interventions Guideline for PCI and 2013 ACCF/AHA Guideline for the Management of STEMI.
PCI was performed using standard interventional techniques. A guiding catheter was inserted through the femoral or radial artery after injecting a local anesthetic into the groin or wrist. After the guiding catheter was placed at the beginning of the cardiovascular system, a contrast agent was injected. Subsequently, radiation was used to photograph the coronary artery to evaluate the cardiovascular system structure and degree of stenosis. After a guiding wire was used to go through the blocked or narrowed blood vessel, pre-dilation was performed with a high-pressure balloon catheter, following which a stent was applied within the rated burst pressure. Following the clinician's judgment, a stent that is 3 mm or longer than the lesion's length was used. Post-dilation was additionally performed when the residual stenosis was >30% after the stent's insertion, and in the case of a long lesion, 2 overlapping stents were applied.
Follow-up
Clinical follow-up was performed immediately after the procedure (baseline), at 4 weeks, 12 weeks, and 36 weeks. For efficacy evaluation, quantitative coronary angiography (QCA) and intravascular ultrasound (IVUS) were performed at the baseline and 36 weeks. QCA results were analyzed using CAAS workstations (Pie Medical Imaging, Maastricht, the Netherlands), and IVUS results were analyzed using Indec Systems (Mountain View, CA, USA). According to the independent evaluation manual, the QCA and IVUS test images were objectively evaluated by an independent evaluator (in Severance Hospital) not related to this clinical trial. For safety evaluation, abnormal case investigation, laboratory examination, vital signs investigation, and electrocardiogram examination were conducted.
Efficacy evaluation
Regarding the primary endpoint, in-segment late lumen loss was evaluated on QCA examination at 36 weeks compared to the baseline. Secondary endpoints were evaluated in terms of QCA and IVUS test results and clinical aspects. On QCA examination, in-stent late lumen loss at 36 weeks compared to baseline, in-segment, or in-stent restenosis rate and restenosis status were evaluated. On IVUS examination, intimal hyperplasia rate and incidence of late stent malapposition at 36 weeks compared to baseline were evaluated. The clinical aspects evaluated were overall death, cardiac death, myocardial infarction, target vessel/lesion revascularization, and stent thrombosis incidence. Stent thrombosis was determined according to the academic research consortium criteria. The procedure was considered successful in the following condition: while the internal diameter stenosis in the stent was <50%, death during hospitalization, myocardial infarction, target vascular/target lesion reconstruction, or stent thrombosis did not occur. The proportion of subjects corresponding to this among all subjects was evaluated as the procedure success rate.
Definitions
In-segment, in-stent late lumen loss shows the degree of intrasegment/intrastent stenosis in QCA results. In-segment refers to a portion including within 5 mm of each of the distal and proximal portions at the boundary of the inserted stent. Therefore, in-segment late lumen loss is defined as the difference (mm) in the minimum lumen diameter within the segment at 9 months from baseline. In-stent late lumen loss is defined as the difference (mm) in the minimum lumen diameter within the stent at 9 months from baseline.
Restenosis is most commonly defined as luminal narrowing of greater than 50% (binary angiographic restenosis). In-stent restenosis refers to restenosis in the stent, whereas in-segment restenosis refers to restenosis within the stent and in areas that include 5mm proximal or distal to the stent margin on follow-up angiography. In volumetric analysis through IVUS, stent's intimal hyperplasia rate was defined as the relative percentage (%) of the overgrown intimal volume, assuming 100% of the stent volume. The procedural success rate was defined as the proportion of patients with <50% internal stenosis of the stent and no major cardiovascular complications (death, myocardial infarction, target revascularization, target lesion reoperation, and thrombus in the stent) during hospitalization.
Statistical analysis
This study is a clinical trial demonstrating that D+Storm™ DES is non-inferior compared to BioMatrix Flex™ DES in the values of in-segment late lumen loss, the primary efficacy evaluation variable after 36 weeks after the stent procedure. Therefore, we tried to use the difference in the effect between DES and BMS, a procedure used before DES, as the basis for setting the non-inferiority limit. According to previous studies, when DES coated with sirolimus was applied 36 weeks after the procedure, the difference in the late lumen loss effect was 0.57, 0.61, and 0.67 in 3 studies, respectively, with an average of 0.58. In this study, the non-inferiority threshold was more conservatively set to 0.25, which is less than the 50% level of this value. Under the one-sided significance level of 0.025 and statistical power of 80%, the minimum number of subjects required to demonstrate the non-inferiority of the investigational group compared to the comparator group was calculated as 50 subjects per group (total of 100 subjects). Considering the dropout rate as 10%, a total of 112 people were registered and analyzed. All efficacy analysis involved the full analysis set group.
Continuous variables were expressed as mean and standard deviation, whereas categorical variables were expressed as frequency and ratio. Depending on the type of variable, between-group comparisons were performed using a 2-sample t-test or Wilcoxon's rank-sum test or Pearson's χ2 test or Fisher's exact test, or 2-sample z-test. All analyses were carried out using SAS ver9.3 (SAS Institute, Cary, NC, USA). The test significance level of the primary efficacy variables was 2.5% (0.025) on one side, and the significance level of the test on all other efficacy variables was 5% (0.05) on both sides.
Go to :
RESULTS
Patient enrollment and follow-up
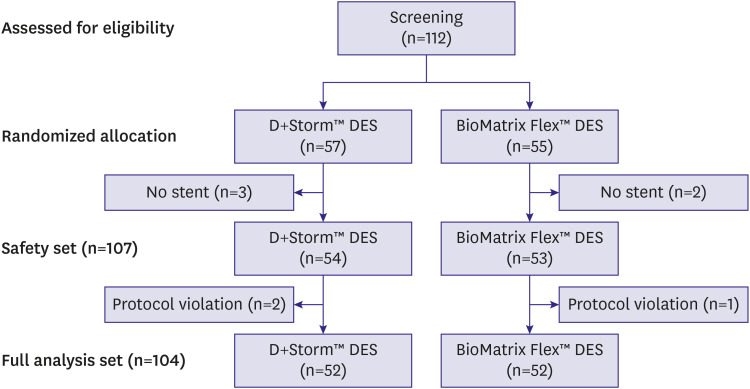
From March 2017 to April 2019, 112 patients from 5 institutions in Korea—57 patients in the D+Storm™ DES group and 55 patients in the BioMatrix Flex™ DES group—were enrolled and randomly assigned in this clinical trial. Among these, a safety set of 107 patients in total (54 in D+Storm™ DES group, 53 in BioMatrix Flex™ DES group) were used in the analysis of safety results, excluding 5 patients who did not have medical devices applied (3 in the D+Storm™ DES group, 2 in BioMatrix Flex™ DES group). Of these, 3 patients (2 in the D+Storm™ DES group and 1 in the BioMatrix Flex™ DES group) were excluded because they were not evaluated on primary efficacy variables. Therefore, 104 patients were included in the efficacy outcome analysis as a full analysis group (52 in the D+Storm™ DES group and 52 in the BioMatrix Flex™ DES group) (Figure 1).
The baseline clinical characteristics are shown that none of the items showed statistically significant differences between the 2 groups in demographic information (age, sex, height, weight, BMI, smoking, smoking amount, alcohol, and alcohol consumption) and disease information (diagnosis and disease period) (Table 2). There were no significant differences between the 2 groups in the lesion characteristics (Table 3). PCI procedural characteristics (method, stent diameter, stent length, pre-dilation, stent overlap, and post-dilation) mostly did not differ between groups (Table 3). However, the pre-dilation pressure was significantly different between the 2 groups with 10.31±3.05 atm in the D+Storm™ DES group and 12.92±3.99 atm in the BioMatrix Flex™ DES group (p=0.001). The first stent insertion was performed on 100% in both groups. The first stent insertion pressure was 13.31±4.03 atm in the D+Storm™ DES group and 11.06±4.38 atm in the BioMatrix Flex™ DES group, showing a significant difference between the 2 groups (p=0.007).
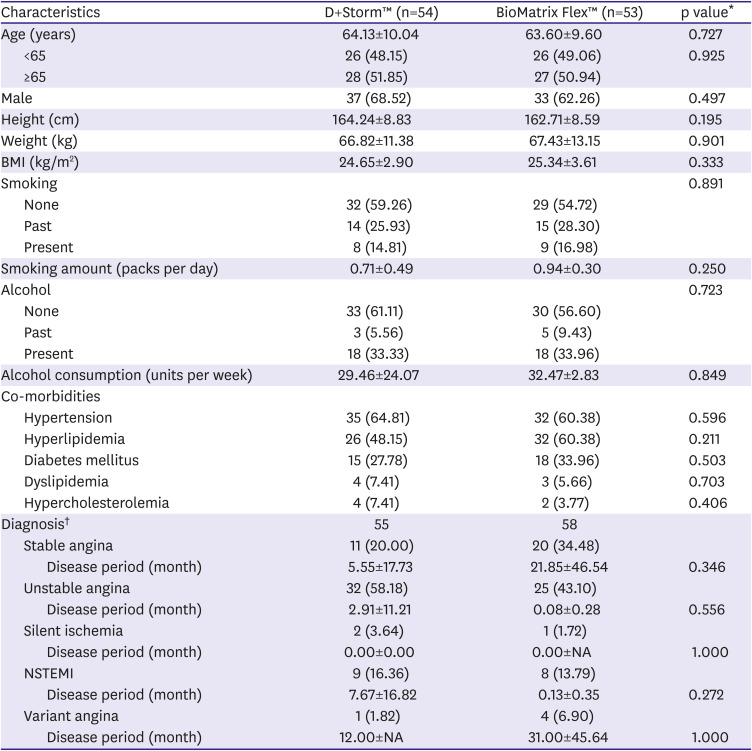
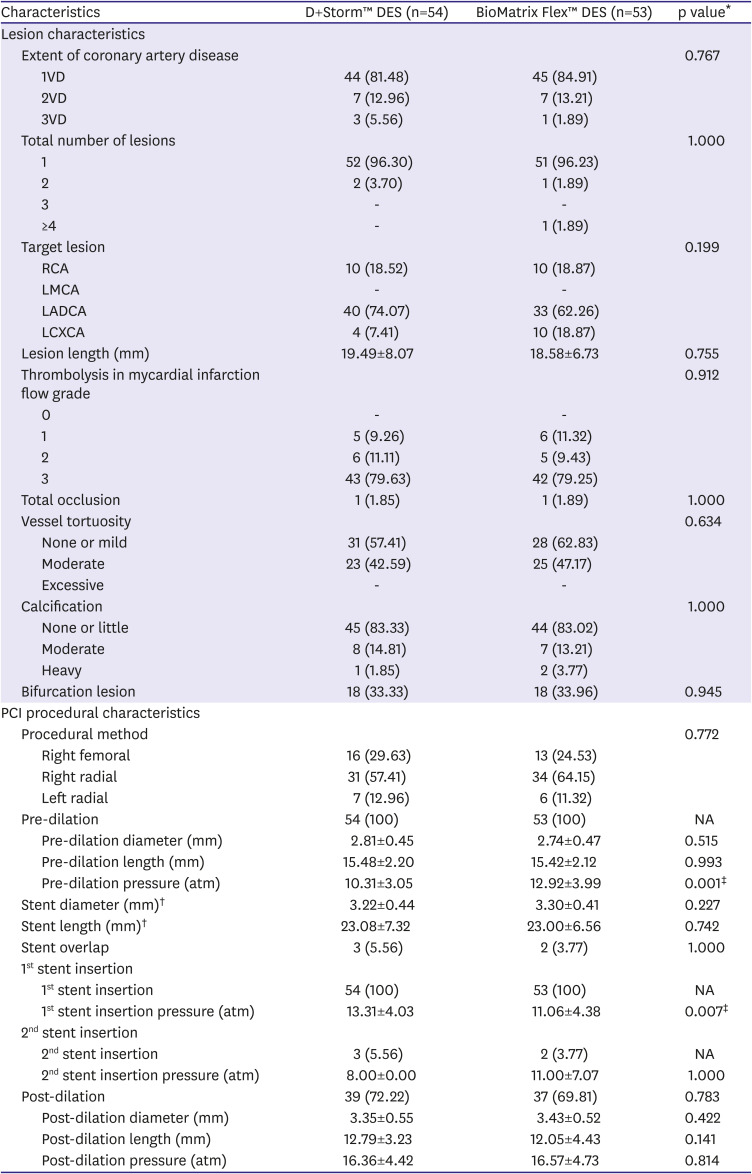
Table 2
Baseline clinical characteristics (safety set)
Data are shown as mean±standard deviation or number (%).
NA = not applicable; NSTEMI = non-ST-elevation myocardial infarction.
*Two sample t-test or Wilcoxon's rank-sum test or Pearson's χ2 test or Fisher's exact test or 2-sample z-test; †Multiple diagnoses can be collected in one subject.
![]()
Table 3
Lesion and PCI procedural characteristics (safety set)
Data are shown as mean±standard deviation or number (%).
DES = drug-eluting stent; LADCA = left anterior descending coronary artery; LCXCA = left circumflex coronary artery; LMCA = left main coronary artery; NA = not applicable; PCI = percutaneous coronary intervention; RCA = right coronary artery; VD = vessel disease.
*Two sample t-test, Wilcoxon's rank-sum test, Pearson's χ2 test, or Fisher's exact test; †Values excluding the results of 5 subjects who had stent overlap; ‡Statistically significant value; p<0.05.
![]()
Clinical effects of the D+Storm™ drug-eluting stent
QCA analysis was performed at 36 weeks for the full analysis group (52 in the D+Storm™ DES group, 52 in the BioMatrix Flex™ DES group). The primary endpoint, an average of in-segment late lumen loss, was 0.08±0.13 mm in the D+Storm™ DES group and 0.14±0.32 mm in the BioMatrix Flex™ DES group, with no significant difference between the 2 groups (p=0.879). The difference between the 2 groups was 0.06, and the lower limit of the 97.5% one-sided confidence interval was −0.04, which was greater than −0.25 set as the non-inferiority margin, demonstrating that the D+Storm™ DES group was not inferior to the BioMatrix Flex™ DES group (Table 4).
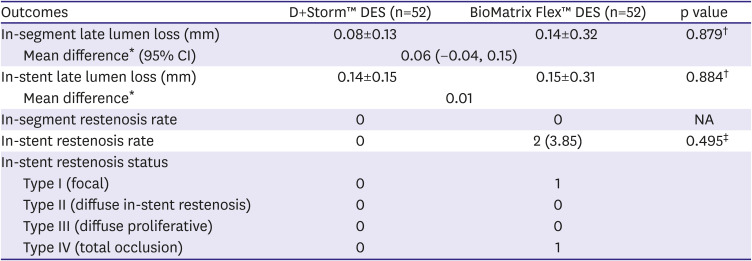
Table 4
Quantitative coronary angiography outcomes at 36-week follow-up
Data are shown as mean or mean±standard deviation or number (%).
CI = confidence interval; DES = drug-eluting stent; NA = not applicable.
*Mean difference=comparator group (BioMatrix Flex™)−investigational group (D+Storm™); †Two sample t-test or Wilcoxon's rank-sum test; ‡Pearson's χ2 test or Fisher's exact test.
![]()
The average of the in-stent late lumen loss was 0.14±0.15 mm in the D+Storm™ DES group and 0.15±0.31 mm in the BioMatrix Flex DES group, which was not significantly different (p=0.884).
In-segment restenosis did not occur in both groups; however, in-stent restenosis occurred in 2 cases (2/52, 3.85%) in the BioMatrix Flex™ DES group (p=0.495), corresponding to type 1 (focal) and type 4 (total occlusion), respectively (Table 4).
A volumetric analysis through IVUS was performed at 36 weeks, with no item showing significant differences between the groups (Table 5). The intimal hyperplasia rate was 3.78±7.03% in the D+Storm™ DES group and 3.57±5.41% in the BioMatrix Flex™ DES group, not significantly different (p=0.612). Late-stage stent malapposition on IVUS occurred in only one patient (1.96%) in the BioMatrix Flex™ DES group (p=0.495).
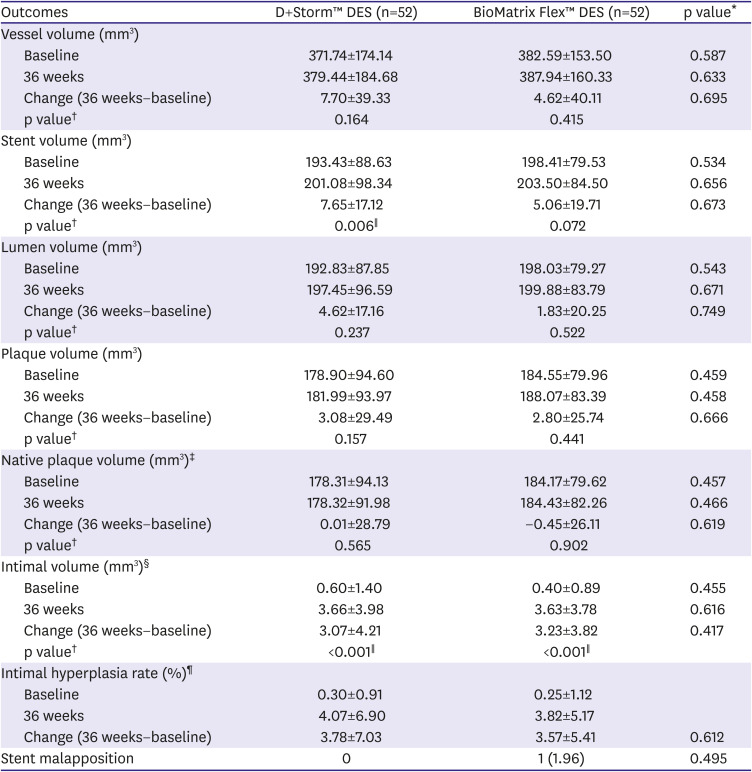
Table 5
Intravascular ultrasound analysis outcomes at 36-week follow-up
Data are shown as mean±standard deviation or number (%).
DES = drug-eluting stent.
*Two sample t-test or Wilcoxon's rank-sum test; †Paired t-test or Wilcoxon's signed rank test; ‡Native plaque volume=vessel volume−stent volume; §Intimal volume=plaque volume−native plaque volume; ∥Statistically significant value; p<0.05; ¶Intimal hyperplasia volume = intimal volume×100/stent volume.
![]()
Safety of the D+Storm™ drug-eluting stent
No overall death, cardiac death, myocardial infarction, and target vessel revascularization (TVR) occurred in both groups during the trial period. (Table 6). Target lesion revascularization (TLR) and stent thrombosis occurred in 1 patient (1.92%) each in the BioMatrix Flex™ DES group alone. The procedural success rate was 100% (52 people) in the D+Storm™ DES group and 96.15% (51 people) in the BioMatrix Flex™ DES group (p=0.495). There were severe adverse events in 4 cases (7.41%; nasal bone fracture, cerebral infarction, Intracranial aneurysm, bacteraemia) in the D+Storm™ DES group and 5 cases (7.55%, angina pectoris, acute myocardial infarction, orthostatic hypotension, chest pain, spinal compression fracture) in the BioMatrix Flex™ DES group. One serious adverse device event of acute myocardial infarction occurred in 1 patient (1.89%) in the BioMatrix Flex™ DES group only.
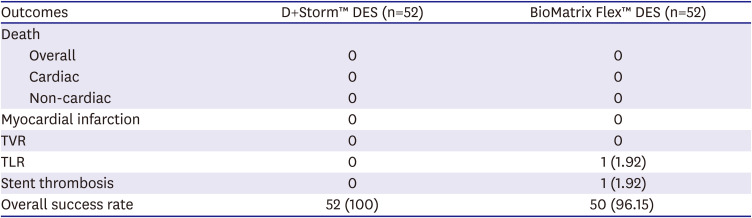
Table 6
Clinical outcomes at 36-week follow-up
Data are shown as number (%).
DES = drug-eluting stent; TLR = target lesion revascularization; TVR = target vessel revascularization.
![]()
Go to :
DISCUSSION
This prospective, multi-center, randomized, comparative, and pivotal clinical study in patients with coronary artery occlusive disease showed that in-segment late lumen loss of D+Storm™ DES group was non-inferior to BioMatrix Flex™ DES group. The procedural success rate was 100% (52 patients) in the D+Storm™ DES group and 96.15% (51 patients) in the BioMatrix Flex™ DES group. The incidence of adverse events was also not significantly different between groups.
When BMSs were used for coronary stent surgery in the past, in-stent restenosis due to excessive intima-hyperplasia resulted in revascularization rates reaching 20–30%.16)17) This led to the development of the first-generation stainless-steel DES, which releases drugs such as anticoagulants and immunosuppressants. In the RAVEL18) and SIRIUS3) studies, the first-generation DES significantly reduced the revascularization rate due to restenosis compared to BMSs. However, in the case of first-generation DES, concerns over late stent thrombosis due to delay in re-endothelialization were raised.19)20) ECs in contact with blood inhibit platelet adhesion and protein aggregation,10) and late stent thrombosis occurred as the re-endothelialization process was delayed, where the stent area was covered with vascular ECs.21)22) To overcome this, the 2nd generation DES was developed with a thinner strut by using a Co-Cr material instead of stainless steel, and more focused on vascular healing by applying a biocompatible polymer for drug release.
Customer demand surveys have shown that dangerous situations in which stents are separated from the delivery system often occur according to the conditions of the stent during the stent procedure. It is designed to compensate for these problems. Since the D+Storm stent has 6 & 8 cell structure with 8 cells at both ends, the stent and the delivery system are designed to increase the coupling force so that the stent does not deviate from the delivery system. It is easy to move smoothly and flexibly even in complex and curved blood vessels with an open cell stent design with a thin strut size of 75 μm. It is easy to enter and mount the vascular lesion with a strut of S-shaped and symmetrical structure, and can be accurately positioned by minimizing recoil and foreshortening.
Atherosclerosis is a disease of initial inflammation and subsequent oxidative damage. Since vitamin C has the potential to counteract both of these processes, it represents a practical solution for the early prevention of the disease. While a role for ascorbate in preventing human atherosclerosis still remains to be defined, mounting evidence supports a role for the vitamin in preventing endothelial dysfunction, plaque stabilization, and macrophage-dependent oxidative modification of low density lipoprotein. Although there is a wealth of in vitro, cellular, and animal data supporting a protective role for antioxidant vitamins and nutrients in the atherosclerotic process, the best clinical trials have been negative. This may be due to the fact that antioxidant therapies are applied “too little and too late.”23)
In this study, In-segment restenosis was not present in both groups, but in-stent restenosis occurred in 2 cases in the BioMatrix Flex™ DES group only.10) Responsible factors for in-stent restenosis can be classified into 3 categories: patient-related (age, female, diabetes, and genetic factors), lesion-related (lesion type, lesion length, complex lesions, ostial lesions and bifurcations, small vessels, and multi-vessel disease), and procedural-related (stent type, the number of a stent, stent length, stent overlap, and minimal lumen diameter).14) The proportion of patients with diabetes was slightly higher in the BioMatrix Flex™ DES group than in the D+Storm™ DES group but there was no statistically significant difference between groups. In some cases, several diseases were diagnosed in one patient, but the diagnosed diseases were not significantly different between groups. Five patients diagnosed with variant angina were diagnosed with mixed variant angina, and PCI was performed. In addition, the 2 groups showed no significant differences in demographic information, lesions, and procedural characteristics (the number of a stent, stent length, stent overlap, and minimal lumen diameter) except for the implanted stent type. Although there was a significant difference between the 2 groups in first stent insertion pressure (p=0.007), the clinical implication of this difference would be small. The initial pressure may also be affected by factors such as the diameter of the selected stent. In this study, the optimal apposition of the stent was confirmed through the imaging modality, not the initial pressure. Major cardiac adverse events (MACEs) of BioMatrix Flex™ DES were reported as follows. The incidence of MACE was 3.8/5.1% at 6/12 months in the STEALTH I study (Germany and Brazil, 120 patients),24) 4.8/6.5% at 6/12 months in the BEACON I study (Asian, 292 patients), 10) and 4.5% at 12 months in the BEACON II study (Asian, 497 patients).25) In this study, total mortality, the incidence of TVR were not present in both groups. None of the adverse events showed statistically significant differences between the 2 groups. However, 1 case of TLR and 1 case of stent thrombosis were reported only in the BioMatrix Flex™ DES group. Serious medical device adverse reactions occurred only in the BioMatrix Flex™ DES group (1.89%, 1 case), acute myocardial infarction. Therefore, the safety of the D+Storm™ DES group at 36 weeks was also demonstrated through this study.
This study has several limitations. First, the study was underpowered for clinical outcomes due to the small number of patients. Large-scale clinical trials are required to demonstrate reduction in-stent thrombosis on high-risk lesions or all-comer patients after PCI in patients with CAD. Second, stent malapposition was analyzed only by IVUS-based PCI. In most image-based PCI follow-up clinical outcomes, there was no difference between the 2 images, but optical coherence tomography is known to be more accurate for observing stent malapposition.26)
In conclusion, this pivotal clinical trial of the D+Storm DES showed excellent clinical efficacy in QCA, IVUS, and clinical outcomes over a 36-week follow-up period and demonstrated safety in CAD patients.
Go to :
 XML Download
XML Download