

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease is a leading cause of mortality and morbidity, producing “immense economic and health burdens” globally.1) Thus, novel treatments for heart failure (HF) and cardiovascular disease in general, have the potential to save millions of lives. One major reason cardiovascular disease remains highly fatal is the limited ability of cardiomyocytes to proliferate after injury.2) Existing therapies help the heart to accommodate following injury, and limit disease progression, but there is currently no method to repair or replace injured myocardium. In patients who progress to end-stage HF, heart transplantation is an option, but organ availability is extremely limited, and rejection remains a challenge.3) Cardiac regeneration has the potential to repair or replace injured myocardium to prevent, making it an attractive avenue for clinical applications.
Existing therapies for cardiac regeneration can be organized into 2 major categories: i) cell-based and ii) bioactive molecules. Cell-based therapies involve the delivery of a cell suspension in order to repair or replace lost muscle tissue. For true cardiac regeneration, it is important that the delivered cells have the ability to differentiate into mature and functional cardiac tissue. Human embryonic stem cells (hESCs) and human induced pluripotent stem cells (hiPSCs) are considered more attractive than cardiac progenitor cells (CPCs) and cardiac stem/stromal cells (CSC) in the recent decade for cell-based therapies, because use of questions about the origin and efficacy of CPCs and CSCs, and the need for isolation from myocardial tissue, unlike hiPSCs and hESCs.4) In addition, hiPSCs and hESCs have essentially unlimited cell division capability and can be differentiated into cardiomyocytes in vitro prior to delivery to the heart. hiPSCs are most attractive, as they are derived from somatic cells, which could potentially be autologous to the patient,4) avoiding the potential for immune rejection, as well as ethical concerns that are associated with hESCs. However, there are still many challenges regarding cell-based therapies. Injection of cells alone has a low survival and retention rate. Moreover, if the desired cell population undergoes incomplete differentiation or ineffective isolation, there is a risk of the formation of teratomas after transplantation.5) Optimal differentiation, maturation, and tissue organization require cells to be supplied with topographical guidance, proper biochemical signaling, and mechanical support.4)6) Pairing cell-based therapies with biomaterial solutions could help optimize clinical applications.
Bioactive molecules harness paracrine effects to enable endogenous cardiac regeneration, as opposed to formation of tissue from directly injected cells. One category of such molecules is growth factors, which are signaling molecules involved in a variety of cellular processes such as aging and survival. It is essential that the delivery of growth factors be local and scheduled due to the pleiotropic functions of most of these bioactive molecules.4) Another class of bioactive molecules that have potential for cardiac regeneration therapy is non-coding RNA, such as microRNA (miRNA) and small interference RNA. In one study, 2 miRNAs (hsa-miR-590 and hsa-miR-199a) were demonstrated to promote cardiomyocyte proliferation in neonatal and adult animals as well as promote cell cycle re-entry of adult cardiomyocytes ex vivo. Though non-coding RNAs have great potential, circulating miRNAs are at risk to be cleaved by RNases when circulating in biofluids and the strong negative charge of soluble nucleic acids leads to inadequate cellular uptake.4) Thus, as with cell-based therapies, efficient and effective delivery of bioactive molecules remains a major challenge for use in the heart, but biomaterials-based approaches have the potential to provide solutions to optimize clinical application (Figure 1).
Figure 1
Biomaterials-based approaches for cardiac regeneration. Traditional therapies including cell-based therapies and bioactive molecules can be directly administered to the heart. The 3 biomaterials-based approaches discussed in this review for administering these traditional therapies as well as novel therapies are: extracellular vesicles, cardiac patches, and injectable hydrogels. While these therapies can be directly administered, extracellular vesicles can also be administered using injectable hydrogels or cardiac patches.
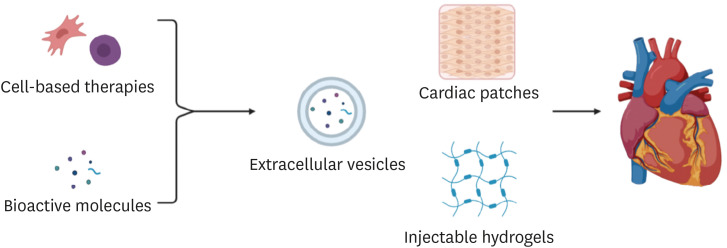
There are three major biomaterials-based applications that have great potential for cardiac regeneration therapies: Extracellular vesicles, Injectable hydrogels, and Biomaterial-based cardiac patches. Briefly, extracellular vesicles are natural carriers that deliver bioactive molecules for the regeneration of tissue. Injectable hydrogels and cardiac patches are different methods using transplantable scaffolds of either synthetic or natural biomaterials that help to deliver therapeutics and reinforce an extracellular environment for cellular approaches to cardiac repair. There are many important considerations regarding biomaterials-based approaches for cardiac regeneration, such as biocompatibility, immunogenicity, and allowance for angiogenesis and vascularization to support contained cells.7) This review will dive into the recent advances, remaining challenges, and future directions for the clinical application of biomaterials-based approaches for cardiac regeneration.
EXTRACELLULAR VESICLES FOR CARDIAC CELL THERAPY
Lipid bound extracellular vesicles (EV), secreted by cells have the ability to be harnessed for drug delivery, as their nucleic acid content (i.e., messenger RNA [mRNA] and mitochondrial RNA) can be transferred to and affect target cells.8) Since EVs are natural carriers of bioactive molecules, they have great potential for cardiac regeneration therapies.9) EVs can be of plasma or endosomal membrane origin, called microvesicles and exosomes, respectively. These vesicles usually contain proteins, mRNA, and miRNA, suggesting their role in mediating cell-cell communication.8) This method of drug delivery has a wide array of advantages, including ease of uptake by target recipient cells, the ability to promote angiogenesis, and limited immunogenicity (Figure 2).4) However, EVs have a short half-life, making sustained delivery a challenge. Moreover, isolation of EVs via traditional cell culture is labor intensive, posing another hurdle for the clinical application of EV-based therapies.10)
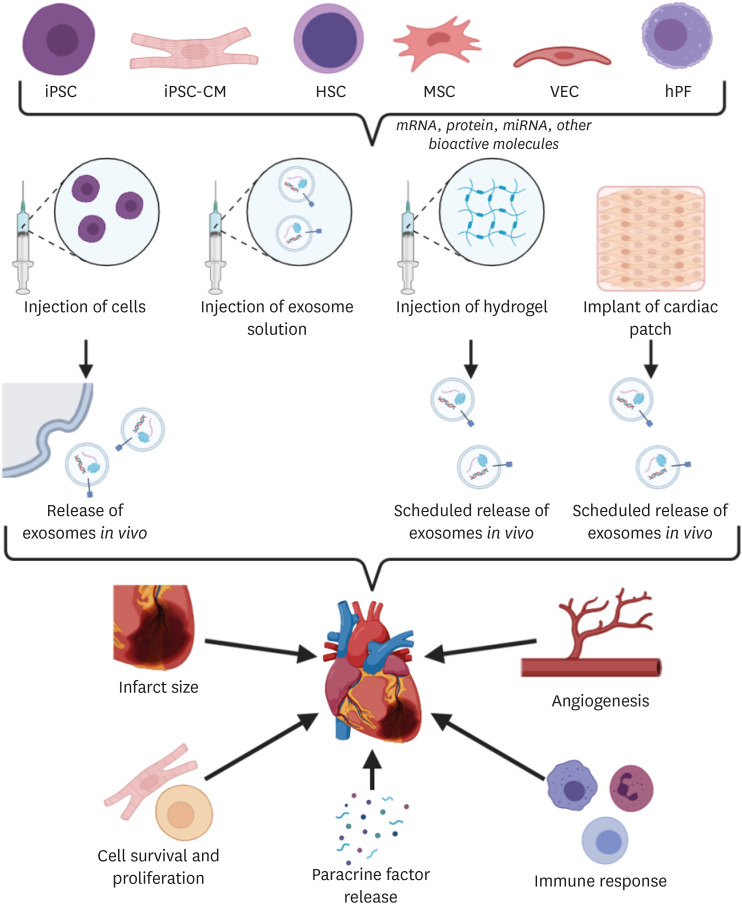
Figure 2
Extracellular vesicles for endogenous cardiac regeneration. Extracellular vesicles derived from many origins, including iPSCs, iPSC-CM, HSCs, MSCs, VECs, and hPF, have shown potential for cardiac regeneration therapy. Exosomes may include mRNA, proteins, miRNA, and other bioactive molecules that facilitate a range of effects including angiogenesis, reduction of infarct size, cell survival and proliferation, paracrine factor release, and modulation of immune response. Delivery of extracellular vesicles through hydrogels and cardiac patches can enable the tailored release of extracellular vesicles, while the injection of parent cells leads to variable release in vivo.
hPF = human pericardial fluid; HSC = hematopoietic stem cell; iPSC = induced pluripotent stem cell; iPSC-CM = cardiomyocytes derived from induced pluripotent stem cells; miRNA = microRNA ; mRNA = messenger RNA; MSC = mesenchymal stem cell; VEC = vascular endothelial cell.
Currently, most EVs are isolated from supernatants through differential ultracentrifugation of cells cultured in fetal calf serum. EVs are then separated from protein aggregates and other nonmembranous particles due to their relatively low buoyant density. EVs of different sizes can be differentiated by floatation velocity.11) EVs of cardiac relevance are most commonly derived from either hiPSC-derived cardiomyocytes (hiCM-EV) or naive hiPSCs (hiPS-EV). A different study, while researching neuronal development, found that use of organ specific cell-derived EVs (e.g., EVs from astrocytes) led to enhanced electrophysiological function12, which suggests that achievement of optimal improvements in cardiac function may require the use of cardiac-specific EVs (e.g., EVs from cardiac fibroblasts). Due to being enriched in cardiomyocyte-specific miRNA, hiCM-EVs in theory have greater potential for cardiac therapeutics in vivo than hiPS-EVs.13) In the past decade, EVs secreted from other types of cells, including hematopoietic stem cells (HSCs), human pericardial fluid, vascular endothelial cells (ECs), and mesenchymal stem cells (MSCs), have also become prominent (Figure 2).10)13)14)15)16)
To increase the efficiency of EV delivery, various advances have been made regarding EV targeting. In 2018, Antes et. al. developed the method of “cloaking,” which involves chemical modification of EVs. Specifically, cloaking involves a process of adding modified glycerol-phospholipid-poly(ethylene glycol) (PEG) conjugates to a solution of isolated EVs. The alternative approach, “surface display”, refers to the genetic modification of parent cells. Both methods have enabled more targeted EV delivery in rats.17) Exosomes engineered with the ischemic myocardium-targeting peptide (IMTP) CSTSMLKAC have been shown to target ischemic myocardium in vitro more efficiently than control exosomes. Genetic modification of exosomes to express the cardiac-targeting peptide-Lamp2b on the exosomal membrane has been demonstrated to enhance exosome delivery to heart cells and heart tissue in mice, both in vitro and in vivo.18)
Use of EV-based therapeutics has shown significant promise in pre-clinical animal trials. For the treatment of myocardial infarction (MI), multiple animal studies on pigs, rats, and mice have been conducted. In one such study, CD34+ hematopoietic stem cells modified for exosome-mediated delivery of the pro-angiogenic factor sonic hedgehog (Shh) were delivered to the heart of mice with acute MI, resulting in preservation of cardiac function compared to control. In addition, the study demonstrated that the injection of Shh-modified CD34+ hematopoietic stem cells reduced infarct size and increased MI border zone capillary density compared to the injection of unmodified CD34+ hematopoietic stem cells as well as the empty vector control.14) In a separate study of mouse MI model, MSC derived Lamp2b membrane protein-enriched exosomes engineered with the IMTP CSTSMLKAC resulted in attenuation of inflammation and apoptosis, reduced fibrosis, and enhanced vasculogenesis and cardiac function.18) A third study in pigs demonstrated that exosomes secreted by cardiosphere-derived cells (CDCs) attenuate adverse remodeling, reduce scarring, and improve left ventricular (LV) ejection fraction after MI. In addition, it was observed that the exosomes delivery decreased cardiomyocyte hypertrophy and LV collagen content, while increasing vessel density.19) Another study found that exosomes secreted by hiPSC-derived cardiac cells improved myocardial recovery without increasing the frequency of arrhythmogenic complications in pigs experiencing MI.20)
Apart from the treatment of MI, various studies on EV-based therapeutics for treatment of ischemia-reperfusion injury have been conducted in vitro using heart-on-chip assays, and in vivo in mice, rats, and pigs. One study developed a human heart-on-chip ischemic reperfusion injury assay to demonstrate that endothelial-derived EVs increase the respiratory capacity of normoxic cardiomyocytes, as well as reducing cardiac cell death and loss in contractile capacity during and after simulated ischemic reperfusion injury in an uptake- and dose-dependent manner.10) Another study using mice and pigs found that exosomes secreted from human endothelial stem cell-derived MSCs reduce myocardial ischemia reperfusion injury.16) A different study in a rat model of acute myocardial ischemia found that after miR-126-enriched treatment, exosomes derived from adipose-derived stem cells decreased the myocardial injury.21) Moreover, treatment with miR-126-enriched exosomes demonstrated a decrease in cardiac fibrosis and inflammatory cytokine expression, as well as the promotion of blood vessel formation in the region of infarction.
A third impactful avenue of EV research is for the treatment of pediatric dilated cardiomyopathy. Preclinical trials in pigs as well as phase 1 clinical trials in patients have identified miR-146a as an important paracrine mediator of the antifibrotic function of CDCs in pediatric dilated cardiomyopathy.22)
Finally, while use of engineered EVs in the heart, whether by direct delivery or via release from injected cells, shows great promise an emerging direction for EV-based therapeutics is their use in combination with injectable patches to further improve therapeutic efficacy. For example, it has been demonstrated that an injectable hydrogel patch that slowly releases EVs secreted from hiPSC-derived cardiomyocytes allows for extended delivery of EVs, prolonging the therapeutic effect, which are notoriously short-lived for EVs delivered alone due to very temporary retention.13) When implanted into infarcted rat hearts, the EV-releasing hydrogel patch was demonstrated to promote recovery of LV function, reduce arrhythmic burden, and decrease cardiomyocytes apoptosis 24 hours post-infarction, and reduced infarct size and cell hypertrophy at 4 weeks after infarction. In another study, a cardiac patch fabricated with PGSA-g-EG polymer enabled the controlled delivery of EVs in vitro for an extended period of more than 14 days.23)
ENGINEERED TISSUE PATCH CONSTRUCTS FOR CARDIAC REGENERATION
Cardiac tissue patches are another major focus of research in cardiac regeneration approaches (Figure 3). Fabrication of cardiac patches stems from two sources of biomaterials: synthetic polymers and natural biological materials. It is critical for the cardiac patch to contain a microstructure that physiologically mimics the native heart, that provides a microenvironment for the incorporated substrates, and mechanical support for the construct itself.24) Natural biomaterials are commonly used in patch fabrication due to their improved biocompatibility. Specifically, materials of natural sources can better recapitulate the extracellular matrix (ECM) microenvironment and facilitate in vivo biochemical signaling. Natural materials used in cardiac patches commonly include decellularized ECM,25)26)27) polysaccharides such as chitosan (CS),28)29)30) and peptides such as collagen,20)21)22)23)24)25)26)27)28)29)30)31)32)33)34) gelatin,35)36)37) fibrin,38)39) and silk fibroin (SF).28)40)
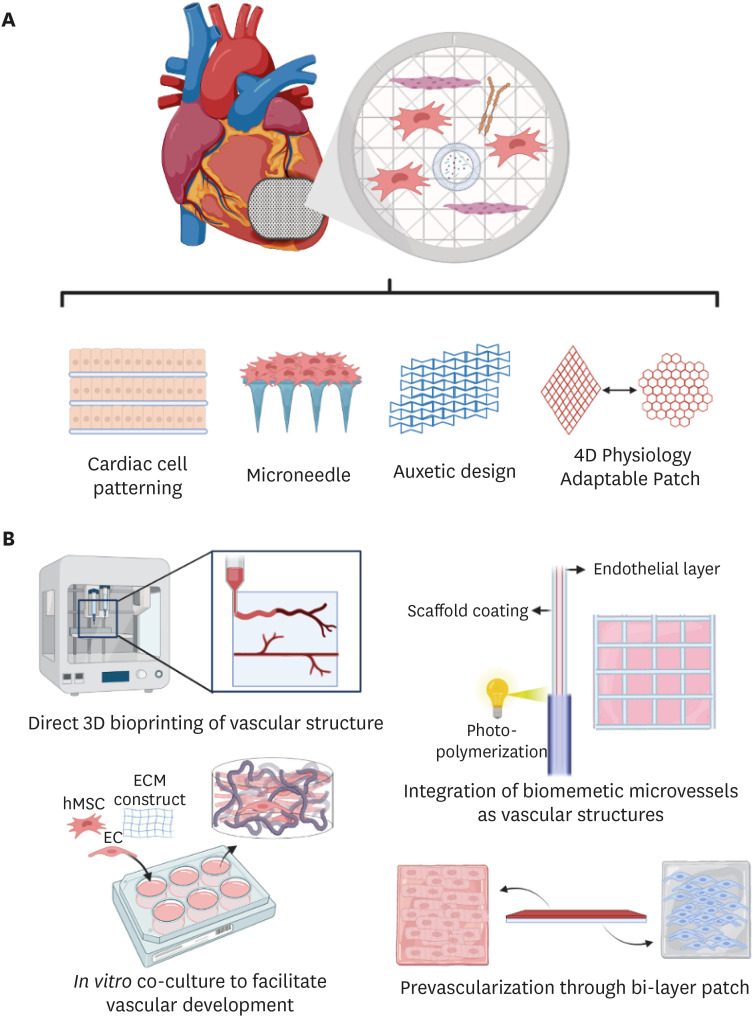
Figure 3
Overview of engineered cardiac tissue patches. Cardiac patches are laboratory-manufactured sheets generally consisted of a scaffolding base and embedded therapeutic molecules that can be applied to the heart to ‘patch’ damaged tissue and help improve cardiac function after injury. Patches come in unique designs and structures such as cell patterning, microneedles, auxetic design, and 4D Physiology Adaptable Patch (A). Vascularization in the patch construct is critical for function of incorporated cells. Several strategies including direct 3D printing, co-culture, bi-layer patches, and BMVs have been employed to achieve higher degree of angiogenesis (B).
3D = 3-dimensional; BMV = biomimetic micro-vessel; EC = endothelial cell; ECM = extracellular matrix; hMSC = human mesenchymal stem cell.
Synthetic polymers are of interest due to their high customizability. Particularly, the mechanical properties, biodegradability, and biocompatibility of the patch can all be tuned by varying the concentrations of the contained polymers. In addition, synthetic materials can be engineered with biological cues to interact with the physiological microenvironment.41) Over the past decade, materials such as poly(ε-caprolactone) (PCL),37)42) poly(glycerol sebacate) (PGS),43)44) poly(lactic-co-glycolic acid) (PLGA),45) biodegradable polyurethane (PU),46) poly(l-lactide) (PLLA),47)48) poly(vinyl alcohol),49) and polyethylene glycol(+)24)35)36)50)51) have been commonly used for the engineering of cardiac patches. However, whether synthetic materials can fully mimic physiological conditions of the ECM remain questionable, as their structural composition drastically differs from their biological counterparts. Therefore, hybrid scaffolds consisting of both natural and synthetic materials are of interest, as this technology takes advantage of both classes of materials. These scaffolds provide the customizability of synthetic materials while maintaining native ECM components for the creation of a better biomimetic cardiac patch. Recently, a PCL/gelatin patch seeded with MSCs effectively restricted ventricular dilation and reduced adverse remodeling of the ventricular wall after MI, while protecting contained MSCs from the hypoxic conditions in the infarct zone.37)
Most cardiac patches rely on the therapeutic components they contain to assist myocardial regeneration and angiogenesis in the infarct area. These substrates may include cells or bioactive molecules such as growth factors, EVs, miRNAs, and even therapeutic drugs. One recent study incorporated alginate microparticles in a collagen-based patch to provide controlled release of hepatocyte growth factor and insulin-like growth fator-1 to enhance endogenous cardiac stem cell migration and proliferation.33) Other acellular patches employ growth factors such as VEGF and bFGF32) or therapeutic drugs such as adenosine45) to directly facilitate paracrine interactions with the host myocardium. Patches without any biomolecules are also able to support cardiac function through mechanical support of the scaffold that facilitates cell migration, angiogenesis,34) increased cell infiltration, and macrophage accumulation.27)
MSCs have been used extensively in cardiac patch applications due to their well-established regenerative and anti-inflammatory effects, many of which are mediated via paracrine mechanisms. For example, a study employing a CS/SF nanofibrous cardiac patch demonstrated improved retention and viability of adipose-derived MSCs contained in the patch, and showed therapeutic potential, including improvement in cardiac fibrosis, inhibition of apoptosis, and promotion of angiogenesis.28) Paracrine signaling from the seeded MSCs can also be modified, as a cardiac patch generated from bone marrow-derived MSCs co-cultured with hepatocyte growth factor expressing-MSCs facilitated continuous secretion of paracrine factors after implantation into a mouse MI model, achieving greater cardiac function 8 weeks after implantation.52)
hiPSC-CMs have the potential to be used for the generation of patient-specific human cardiac patches.53) Co-injection of hiPSC-CMs and supporting cell types (ECs and smooth muscle cells [SMCs]) in a cardiac patch have achieved greater cell engraftment and improvements in myocardial wall stress, apoptosis, vascularization, metabolism, contractile function, and cell viability in porcine39) and murine36) MI models. Another study has also employed hiPSC-CM to create cardiac strips improving LV function after transplantation.54) However, scale-up production remains a challenge for this cell source due to its difficulty expanding in large volumes.
Translation of cardiac patch applications to clinical use presents several practical hurdles to be overcome. First, to proceed to clinical use, a cardiac patch needs to achieve a size relevant to the typical infarct size in human myocardium. A patch of clinically relevant dimension (4×2 cm ×1.25 mm) was generated through suspension of hiPSC-derived CMs, ECs, and SMCs, and was shown to significantly reduce infarct size and reduce LV wall stress.55) However, with increased thickness and size of a patch, it is critical to ensure adequate vascularization within the tissue construct, which is critical for nutrient and signal exchange between the cardiac patch substrates and the host cells, as well as to maintain viability and growth of the seeded cells. Several strategies can be employed while designing the patches to facilitate the development of microvascular networks. Pre-vascularization in the cardiac patch can be achieved through co-culture hMSC and ECs in an aligned nanofibrous ECM construct, where hMSCs translate the scaffold alignment and guides formation of microvascular structure. Stacking of these vascularized patches can achieve a physiologically relevant 3-dimensional (3D) tissue with embedded vascularization throughout the structure.26) Vascularization can also be generated through fabrication of biomimetic micro-vessels (BMVs) through hydrodynamic focusing. Alignment of these BMVs in a CSC patch created a protective microenvironment for the CSCs and facilitated release of angiogenic signals after patch transplantation in rat MI model.50) A bilayer approach with a hiPSC-CM patch layer and a self-assembled human micro-vessel layer can also provide vascularization. In one study a hiPSC-CM patch paired with a micro vessel patch composed of human blood outgrowth ECs and pericytes and attached with thrombin allowed for increased density of microvasculature network and angiogenesis within the CM layer after 4 weeks of in vivo transplantation in rat MI model.56) Lastly, 3D printing using a bio-ink composed of decellularized human omentum tissue hydrogels, iPSC-CM, and iPSC-ECs can be used to directly imprint a vascular network onto a cardiac patch. This specific paradigm allows for creation of autologous, patient-specific cardiac patches, which can drastically reduce the risk of adverse immune response after implantation.57)
Another cardiac patch design consideration includes incorporation of structural cues from surface topography to improve the maturation of seeded cardiomyocytes and better recapitulate the phenotype of the myocardium.58)59)60) One study fabricated PEG-DA based hydrogels with aligned micro grooves of and ridges of 400nm and 500nm in width, which are within the range of native ECM dimensions. These nanopatterned grooves facilitate adhesion, migration, proliferation, and differentiation of seeded CDCs.61)62) Transplantation of the nano-structured scaffold in a rat model of MI improved myocardial repair with increased wall thickness and improved ECM organizations compared to controls.63) Another study achieved nanopatterning from electrospinning polyacrylonitrile to generate an anisotropic nanofibrous patch. The nanopattern design proved important, as while cardiac patches designed using either anisotropic or random PAN electrospun nanofibers both facilitated neovascularization, the cardiac patch with random nanofiber alignment seeded with CMs and ECs lead to severe adverse remodeling and deterioration compared to the unseeded patches, while seeded anisotropic cardiac patches improved cardiac function post infarction in a rat model.64) To make cardiac patches cost-effective and scalable, some studies developed substrates including biocompatible polymers using PLGA and PU, biodegradable composite hydrogels consisting of PEG dimethacrylate and gelatin methacrylate, and even free-standing PCL thin films that were successful in regulating cellular alignment.65)66)67) Thermoresponsive nanofabricated substratum is a cell sheet engineering technique that can provide the necessary topography for contact guidance, enabling cell sheet alignment and transfer.68)69) Because of the versatility of this technique, researchers are able to efficiently stack individual layers of cells to create dense, scaffold-free tissues.70)
Besides the surface topography that guides cardiomyocyte maturation, other design considerations can improve cardiac patches by improving alignment with the shape change inherent during contraction of the human heart. One study generated an auxetic micropatterned cardiac patch in a ‘bowtie shape’ with a conducive composite of polyaniline and phytic acid through excimer-laser micro ablation. The mechanical property of the material was tuned to match that of the native heart while preserving conductive properties. Once implanted, the cardiac patch stretched according to the movement of the native heart tissue without detrimental effects on cardiac function.28) To achieve higher morphological adaptability of cardiac patches, another study developed a 4D patch with gelatin methacrylate and polyethylene glycol diacrylate that fully recapitulates anisotropic alignment in the human heart. The construct exhibits a dynamic stretchability that prevents material deformation during the shift between the diastole and systole phase, which improved in vivo cell engraftment and vascularization when implanted onto a murine MI model.32) Patch design can also be modified to enhance delivery of signaling molecules secreted by seeded cells. In one example, a microneedle patch made of polyvinyl alcohol was engineered to provide channels for improved transport of signaling molecules into the host myocardium. Despite direct insertion into the tissue, the damage to the host myocardium was negligible. In this study, CSCs encapsulated in fibrin gel were seeded on the back of the microneedle patch and significantly improved thickness, viability, and LV ejection fraction of the infarct wall, reduced mal-adaptive remodeling, and facilitated cardiac repair in rat and pig MI models.42)
Lastly, incorporation of other material constructs into cardiac patch design can provide unique properties. Gold is one material being actively investigated due to its capability to be synthesized in a wide variety of shapes and sizes to achieve desired functional effects. In one study, a bilayer cardiac patch was constructed using an elastic collagen hydrogel layer and an electroconductive fiber layer made with gold particles and collagen. Under electrical simulation, the nano-gold-containing patch enhanced the number of connexin 43 positive cells, increased vascular density, and decreased myocardial scar size post infarction in a rat model.31) A different application utilized the property of gold to be locally heated upon irradiation to provide a suture-free engraftment of the cardiac patch when incorporated into the heart.71) Electrical conductivity for engineered cardiac tissue constructs is also highly desirable, where the incorporation of materials including graphene, acid-modified silk fibroin-poly(pyrrole), and nafion with physiologically relevant nano-topographies have led to improved integration with the cellular environment.72)73)74) To measure electrical conductivity, 3D microelectrode arrays (MEAs) and nano MEAs have emerged as promising tools to detect electrical activities of tissues both in vitro and in vivo.75)76)
INJECTABLE HYDROGELS FOR CELL DELIVERY AND CARDIAC REGENERATION
Another promising approach to cardiac regeneration that has had a large amount of preclinical data is the use of injectable hydrogels. These are transplantable biomaterials that can be both natural and synthetic, helping to deliver therapeutics and reinforcing an extracellular environment for cellular approaches to cardiac repair. Typically, hydrogels are directly injected to the damaged myocardial site. This approach allows for immediate contact with the area of interest, potentially leading to better cell localization and retention, as well as minimal invasion compared to the epicardial method or catheter method, both of which typically enter through the left ventricle with risk of puncture.50) Generally, the hydrogel material is designed to be injected as a liquid solution, and upon reaching the target area will undergo gelation into a 3D polymeric network that rapidly integrates with the surrounding tissue. This gel phase transition allows for easy delivery while in liquid form, as cardiac muscle tissue is continuously in contractile motion, yet upon gelation, can still create a protective environment to enhance cell viability and/or biomolecule activity.51)
The number of hydrogels that have potential for injectable cardiac tissue engineering is vast, and in the past decade have come to include novel combinations of materials. These are typically split into natural hydrogels such as collagen, fibrin, Matrigel, hyaluronic acid, alginate, and chitosan, and synthetic materials, which include PEG, polylactide, PLGA, PCL, and polyacrylamide.77) Careful considerations when using these materials are to make sure that they are biocompatible once placed into the body, but still being tailored to provide important functional properties needed to optimize cardiac tissue regeneration. Hydrogel-based approaches that do not incorporate cells are closely related field to the field of cardiac injectables. For example, 3D bioprinting of decellularized ECM is a strategy that, while still imperfect in fostering adequate vascularization and elaborating architectural features, is attractive due to its capacity for integration of electroactive materials into cardiac prints.78)79) Advancements in bioprinting in the areas of extrudability, shape fidelity, rapid cross-linking, and cytocompatibility highlight the strong potential of this platform to allow for more effective regenerative therapies, as well as high-throughput drug screening.80)81) Acellular hydrogels by themselves have also been shown to provide benefit as bulking agents that attenuate the maladaptive geometric changes that result after infarction due to ECM breakdown resultant adverse remodeling.82)
There have been several experiments already involving injecting hydrogels for cardiac regeneration in humans. For example, the AUGMENT-HF clinical trial was an international, randomized, controlled program to evaluate the effects of alginate-hydrogel treatment on patients with advanced chronic HF.83) By evaluating markers including exercise capacity, severity of HF symptoms, and echocardiograms, it was discovered that the addition of the alginate-hydrogel to standard care was more effective than standard care alone. A part of the AUGMENT-HF trial, Algisyl-LVR™ is a calcium-alginate hydrogel that underwent a randomized study to assess its efficacy of LV augmentation in the treatment of advanced HF patients with both ischemic and non-ischemic cardiomyopathies.83) Through magnetic resonance images obtained pre and post treatment, implantation of this material was found to be safe and decrease LV wall stress reduction compared to the control, a major hallmark in treating HF. Ongoing studies seek to investigate potential long-term benefits of Algisyl-LVR™ in patients.
In another joint international effort, a bioabsorbable cardiac matrix was developed to attenuate adverse LV remodeling following large MIs.84) Through a randomized, double-blind, controlled trial involving more than 300 subjects, it was found that there was no significant chance in LV end-diastolic volume index at 6months. While efficacy was not shown, this probes further investigation into the use of alginate in a cardiac treatment setting. More recently, an injectable ECM developed by Ventrix Inc. underwent Phase 1 clinical trial to study the effects of percutaneous administration of VentriGel—“the first product of its kind that contains myocardial specific extracellular matrix components”—following MI.85)86) Previously, this material had been demonstrated in infarcted pigs to have improvement in cardiac function, ventricular volumes, and global wall motion scores 3 months after treatment. The clinical trial saw that the transendocardial injection of VentriGel in post-MI patients with LV dysfunction was both safe and feasible, prompting evaluation in larger trials and efficacy testing.
Injectable hydrogels incorporating cell-based therapy is another area with promising therapeutic potential. Various approaches have incorporated ESCs, bone marrow-derived stem cells, and even CSCs.87) The major goals of hydrogel-based cell therapy are for incorporated cells to have cardiomyogenic potential when implanted into the infarcted area and a high capability for expansion. Currently, three clinical studies combining cell therapy and hydrogels for cardiac tissue treatment, mostly conducted through cardiac patchwork.88) In the clinical feasibility study termed the Myocardial Assistance by Grafting a New Bioartificial Upgraded Myocardium (MAGNUM) trial, bone marrow cells and collagen matrix were implanted to treat patients presenting LV postischemic myocardial scars.89) The addition of the collagen seemed to normalize cardiac wall stress and limit harmful ventricular remodeling, thus making the biomaterial safe and potentially efficacious. In another clinical case report, embryonic stem cell (ESC)-derived cardiac progenitor cells embedded in fibrin was implanted into a patient with severe HF, and after 3 months, the patient symptomatically improved from New York Heart Association functional class III to I.90)
A more recent materials area that has been investigated is hydrogel-based nanocomposites, i.e., the incorporation of nanoparticles, nanotubes, and nanofibers into injectable hydrogel technology. Desirable properties for cardiac tissue engineering such as electrical conductivity, strong cell adhesion, and angiogenesis have been achieved with nano-formulations including rosette nanotubes, carbon nanofibers, and gold-loaded Laponite nanoparticles.91) Three-dimensional myocardial matrix-graphene composite scaffolds that mimic the electrical, mechanical and biochemical environmental cues are currently in transition to injectable forms that would allow for testing in vivo.92) Other approaches seek to activate beneficial cellular processes to improve cell viability and retention when deposited. In the past decade, injectable hydrogels have become increasingly investigated for clinical potential. Several findings coming out of preclinical studies with small- and large-scale animal models have pointed to safety and feasibility results that prompt human clinical trials. A summary of recent injectable biomaterials that have gone through preclinical study can be found in Table 1.93)94)95)96)97)
Table 1
Summary of injectable biomaterials for cardiac tissue regeneration

| Biomaterial | Type | Implementation | Reference |
|---|---|---|---|
| Collagen-chitosan | Natural | Chitosan was added to an injectable collagen matrix to improve cell therapy efficacy. | 93 |
| Sericin, a silk-derived protein | Natural | An injectable form of sericin was prepared and led to infarct size reduction. | 94 |
| Oligo(poly[ethylene glycol] fumarate) | Synthetic | OPF may serve as a carrier for ESCs for MI treatment to improve cell retention. | 95 |
| Calcium cross-linked alginate | Natural | Intracoronary injection of alginate prevents adverse LV remodeling after MI. | 96 |
| Elastin-like recombinamers | Synthetic | An ELRs-based hydrogel was developed to prevent ischemic heart disease progression. | 97 |
CONCLUSION AND FUTURE PERSPECTIVE
Biomaterials-based approaches have the potential to augment and solve many of the shortcomings of existing therapies for cardiac regeneration, enabling translation to clinical application. Clinical trials in both animals and humans have been conducted for therapies involving extracellular vesicles, cardiac patches, and injectable hydrogels, revealing the great promise of these approaches. Though there remain shortcomings and challenges, the promising results of numerous clinical trials demonstrate the potential of biomaterials for clinical applications regarding cardiac regeneration (Table 2).4)8)10)11)13)14)18)19)20)21)23)24)25)34)35)36)37)42)43)44)45)46)47)48)49)50)51)52)56)65)77)82)87)91)98)99) With the advent of stem cell-based and genome editing technologies for cardiac engineering, the translational potential of these biomaterials-based approaches will continue to grow.100)
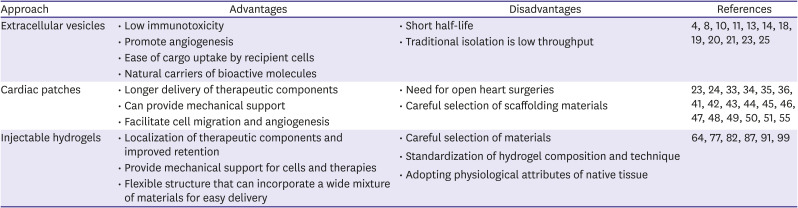
Table 2
Comparison of biomaterials-based approaches for cardiac regeneration
| Approach | Advantages | Disadvantages | References |
|---|---|---|---|
| Extracellular vesicles | • Low immunotoxicity | • Short half-life | 4 8 10 11 13 14 18 19 20 21 23 25 |
| • Promote angiogenesis | • Traditional isolation is low throughput | ||
| • Ease of cargo uptake by recipient cells | |||
| • Natural carriers of bioactive molecules | |||
| Cardiac patches | • Longer delivery of therapeutic components | • Need for open heart surgeries | 23 24 33 34 35 36 41 42 43 44 45 46 47 48 49 50 51 55 |
| • Can provide mechanical support | • Careful selection of scaffolding materials | ||
| • Facilitate cell migration and angiogenesis | |||
| Injectable hydrogels | • Localization of therapeutic components and improved retention | • Careful selection of materials | 64 77 82 87 91 99 |
| • Provide mechanical support for cells and therapies | • Standardization of hydrogel composition and technique | ||
| • Flexible structure that can incorporate a wide mixture of materials for easy delivery | • Adopting physiological attributes of native tissue |
In summary, although extracellular vesicles provide a promising method for administration of therapeutic bioactive molecules, a shortcoming is the short half-life, which limits the clinical relevance of this approach and may necessitate repeated administrations. One potential future direction is harnessing injectable hydrogels and patches, which could enable more sustained delivery of extracellular vesicles to have a greater clinical impact. Treatment using extracellular vesicles targeted at a specific cell type within an organ has the potential to improve the efficacy of the therapy by minimizing adverse effects.98) As discussed in this review, various advances such as the development of “cloaking” have been made regarding EV targeting. However, there is yet to be extensive clinical studies on cardiac treatment using EVs tailored to target specific cell types within an organ, and thus this is another area for further research. Moreover, the constituents of EVs are not uniform and largely dependent on the physiological state of the parental cells. Therefore, research regarding the variability of cargo among as well as within EVs must be conducted before this therapeutic has clinical relevance for cardiac regeneration.
For cardiac patches, in recent years multitudes of preclinical studies have supported for the ability of cardiac patches to promote cardiomyogenesis, angiogenesis, and restoration of heart function after MI. Advances in utilizing different combinations of therapeutic ingredients, material compositions, and patch designs have resulted in improved regeneration in infarcted heart tissue. Despite these encouraging results, the transition to clinical trials remains a challenge for the field of tissue engineering. First, current methods in implementing the patch construct require open chest surgery. Many patients remain too fragile to withstand the damage of such invasive procedures, and novel methods of implantation need to be considered. In addition, the properties of the scaffolding material need to be tailored to patients, retaining their ability to support cardiac regeneration while maintaining high biocompatibility and biodegradability. Next, the vascularization and the structure of cardiac patches need to be optimized to allow for faster and more mature vessel development after implantation. Multitude of strategies have been imposed for pre-vascularizing the platform or developing an adaptable cardiac patch. Further development of a highly vascularized adaptable patch that can better recapitulate the native myocardium may provide more clinically relevant results. Finally, in patches that incorporate cells, the efficiency in obtaining sufficient numbers of therapeutic cells and the maturity of hiPSC-CMs where they are used need to be considered. With recent advances in cellular engineering to obtain more mature hiPSC-derived tissues, combination strategies may allow for use of autologous, patient-specific cardiac patches to minimize the risk of rejection.
Finally, injectable hydrogels, with an increasing amount of clinically-backed evidence to support both safety and efficacy, have a clear pathway for translation to clinical use in a variety of cardiac conditions within the next decade. The advantages of direct localization at the damaged site, minimally invasive delivery, and the flexible suite of hydrogels, biomolecules, and cells that can be incorporated into this technology contribute to the strong therapeutic potential of this approach. However, the road to clinical translation continues to be present challenges, as factors such as deployment volume, preclinical model relevance, and the accuracy of metrics used to determine cardiac tissue recovery continue to result in variability in the findings between pre-clinical studies and clinical trial results. Stem cell therapy in general continues to face economic and logistical issues that have limited the path for the development of mainstream cell-based therapies. Yet, as the global demand for novel cardiac therapies grows, creating a consistent, high-throughput standard for biomaterials-based treatment approaches will be a major priority. More recent studies of hydrogels incorporating various cells, biomolecules, nanoparticles, and other materials show a promising future for injectable hydrogels to mimic the physiological and functional properties of native myocardium.
 XML Download
XML Download