

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial septal defect (ASD) is among the most commonly reported congenital heart diseases (CHDs), accounting for about 10% of all CHDs in children,1) with secundum ASD comprising approximately 80% of the ASDs.2)
Some patients with a large ASD remain asymptomatic until adulthood2); however, if left untreated, symptoms such as dyspnea, arrhythmia, reduced functional capacity, right heart failure, respiratory infections, and stroke may present through right ventricle (RV) volume overload and pulmonary overflow.2)3)
Although both transcatheter and surgical closures yield excellent short and long-term ASD treatment outcomes,4) several studies have reported the superiority of transcatheter closure to surgery in terms of hospitalization duration, costs, and rates of treatment-related complications and infections.4)5)
As a part of ASD treatment, diuretics are occasionally administered to reduce the rate of RV volume overload for the control of heart failure-related symptoms6); however, the effect of diuretics on ASD size change remains unclear. This study aimed to evaluate the efficacy of diuretics in ASD size reduction by comparing patients who received and did not receive diuretic treatment, and their outcomes.
METHODS
Ethical statement
This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 2003-191-1112) and the need for consent was waived owing to the retrospective study design.
Patient characteristics
We retrospectively reviewed the medical records of pediatric patients diagnosed with a large secundum ASD (size ≥10 mm), as observed on echocardiography, at the Seoul National University Children's Hospital between 2005 and 2019. Patients with other concomitant CHDs, such as a ventricular septal defect or patent ductus arteriosus, and those aged ≥10 years were excluded. Patients were divided into two groups based on their diuretic reception status. Patients who received diuretics and were followed-up for a sufficient duration (approximately 2 years) were assigned to the diuretic group. If parents wanted device closure to be performed after the patient had grown a little more while not requiring immediate ASD closure, diuretics were given for the purpose of RV volume unloading. Age-matched patients who were not treated with diuretics for a sufficient duration during study period were assigned to the non-diuretic group. Data regarding the patients' gestational age, weight, height, genetic defect, clinical symptoms, and the use of diuretics and treatment, including transcatheter and surgical closures, were collected.
Echocardiographic measurement of atrial septal defect
Of the ASD images recorded from various angles, the largest measured ASD size was selected, and for data consistency, the ASD size was re-evaluated from the ASD images measured at the same view wherever possible. Since the patient's somatic growth occurred during the administration of the diuretics, the indexed ASD diameter was also evaluated to compare the ASD size over the patient's body surface area (BSA) for the correction of body size differences. From the available images, aortic, superior vena cava (SVC), inferior vena cava (IVC), posterior, and mitral rim measurements were performed. Rim deficiency was defined as a rim size <5 mm. The presence of a floppy interatrial septum, multiple ASDs, and other heart anomalies were evaluated. All patients' echocardiography findings, as obtained during follow-up, were investigated for serial changes in the ASD size. To decrease the degree of inter-observer variability, the ASD size was remeasured by a cardiologist who was blinded to the patients' information, including their diuretic administration status; these measurements were averaged with the previously recorded ASD size.
Outcome measurements
The primary outcome was the effect of diuretics on ASD size reduction and treatment outcomes. The secondary outcome was the identification of the risk factors associated with a lack of ASD size reduction and those related to the need for surgical closure despite diuretic use. Owing to concerns pertaining to growth retardation related to diuretic administration, the percentiles of the patients' height and body weight were evaluated before initiating diuretics and after the reception of follow-up echocardiography. To determine the sex and age-specific percentiles for height and body weight, Korea Centers for Disease Control and Prevention data were used.7)
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as mean ± standard deviation or median (interquartile range: 25th to 75th percentile) and categorical variables as numbers and percentages. Continuous variables were compared using either Student's t-test or Mann–Whitney U tests and categorical variables by employing χ2 or Fisher's exact tests. Linear mixed model analysis was performed for the identification of meaningful factors associated with ASD diameter and indexed ASD diameter change. A p value of <0.05 was considered statistically significant.
RESULTS
Baseline characteristics
Seventy-three patients with an ASD diameter ≥10 mm were enrolled in this study. Diuretics were administered in 40 of them. The patients' baseline characteristics are shown in Table 1. The initial age at ASD diagnosis was not significantly different between the diuretic and non-diuretic groups (2.8±1.7 vs. 2.5±2.0 years, respectively, p=0.526). The follow-up duration was also not significantly different between two groups (22.3±11.4 vs. 18.7±13.2 months, respectively, p=0.224). Patients in the diuretic group were prescribed, on average, a starting dose of 0.77±0.19 mg/kg/day furosemide and 0.81±0.19 mg/kg/day spironolactone and the diuretic dosage rose with increasing body weight. The definite treatment age was higher in the diuretic group (5.3±1.4 vs. 4.0±1.8 years, p=0.003).
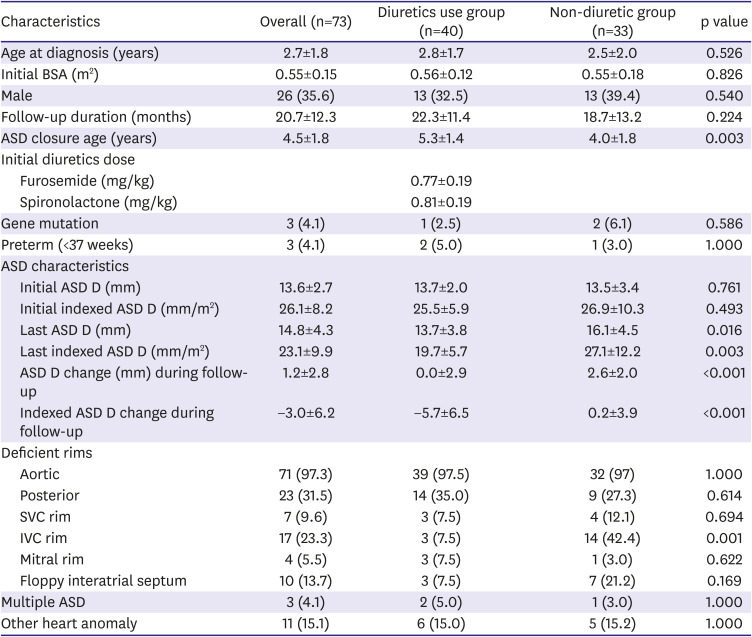
Table 1
Baseline characteristics and ASD size changes
Values are mean ± standard deviation or number (%).
ASD = atrial septal defect; ASD = atrial septal defect; ASD D = atrial septal defect diameter; BSA = body surface area; IVC = inferior vena cava; SVC = superior vena cava.
![]()
Changes in atrial septal defect size over time
Echocardiography was usually performed every 6 months or 1-year and the changes in the ASD size were investigated until just before transcatheter or surgical ASD closure. Data regarding the ASD size changes are presented in Table 1. The ASD diameter at initial diagnosis (13.7±2.0 vs. 13.5±3.4 mm, p=0.761) and the indexed ASD diameter (25.5±5.9 vs. 26.9±10.3 mm/m2, p=0.493) were not significantly different between two groups. At the last follow-up, the ASD diameter (13.7±3.8 vs. 16.1±4.5 mm, p=0.016) and the indexed ASD diameter (19.7±5.7 vs. 27.1±12.2 mm/m2, p=0.003) were significantly smaller in the diuretic group. During the follow-up, the non-diuretic group (2.6±2.0 mm) showed significantly increased ASD diameter change compared with the diuretic group (0.0±2.9, p<0.001). The indexed ASD diameter significantly decreased in the diuretic group during follow-up (−5.7±6.5 vs 0.2±3.9 mm/m2, respectively, p<0.001) (Table 1).
We used linear mixed model analysis to investigate the degree of ASD size changes with echocardiography examinations adjusted for follow-up duration in both groups. Both the ASD and indexed ASD diameter changes showed significant differences over time in both groups; the patients who received diuretics showed a significant ASD size-decreasing tendency compared to the non-diuretic group (ASD diameter, p for interaction<0.001; indexed ASD diameter, p for interaction<0.001; Figure 1).
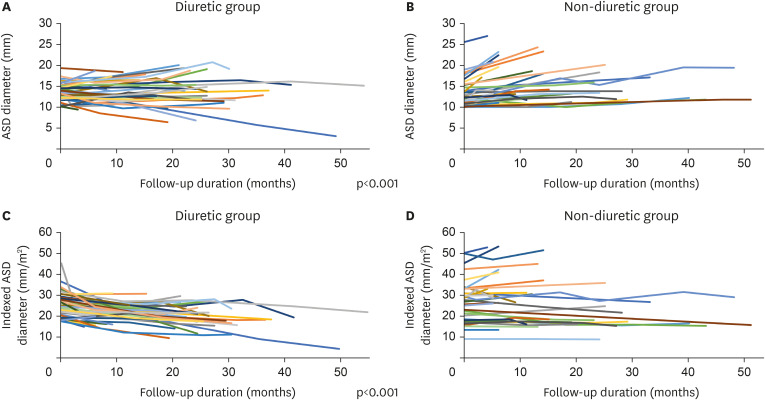
Figure 1
ASD size changes over time. (A, B) Patients who received diuretics showed a significantly decreasing tendency of absolute ASD diameter (mm) over time (p for interaction<0.001). (C, D) Patients who received diuretics showed a significantly decreasing tendency of indexed ASD diameter (mm/m2) over time (p for interaction<0.001).
ASD = atrial septal defect.
![]()
We investigated the distribution patterns in the two groups based on the ASD diameter change status and divided the patients into the decreased, stationary (within ±1 mm), and increased groups. In the diuretic group, the ASD diameter was decreased, stationary, and increased in 20.0%, 45.0%, and 35.0% of the patients, respectively. In the non-diuretic group, none of the patients showed ASD diameter decrease, and it was stationary and increased in 18.2% and 81.8% of the patients, respectively (Figure 2).
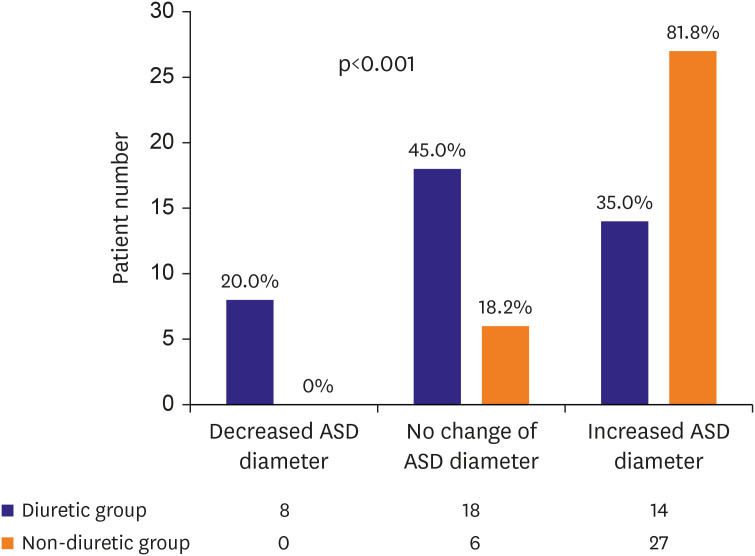
Figure 2
Distribution of ASD diameter change (mm) in the two groups. The absolute ASD diameter was decreased in 20.0%, maintained in 45.0%, and increased in 35.0% of the patients in the diuretic group. In the non-diuretic group, there was no decrease in the absolute ASD diameter; in 18.2% of the patients, the value was maintained and in 81.8%, it was increased (p<0.001).
ASD = atrial septal defect.
![]()
Factors affecting atrial septal defect size change
Table 2 presents the results of linear mixed model analyses of ASD diameter change and indexed ASD diameter change. The use of diuretics was the significant factor independently associated with ASD diameter decrease during follow-up (p for interaction<0.001). Initial ASD diameter (p<0.001) and IVC rim deficiency (p=0.002) also showed significance for ASD diameter change. In the analysis for indexed ASD diameter change (mm/m2), the use of diuretics was the significant factor associated with reductions in the indexed ASD diameter during follow-up (p for interaction<0.001). In addition, IVC rim deficiency was a significant factor for indexed ASD diameter increase (p=0.001). Initial ASD diameter (p=0.039) and initial indexed ASD diameter (p<0.001) also showed significance for indexed ASD diameter change.
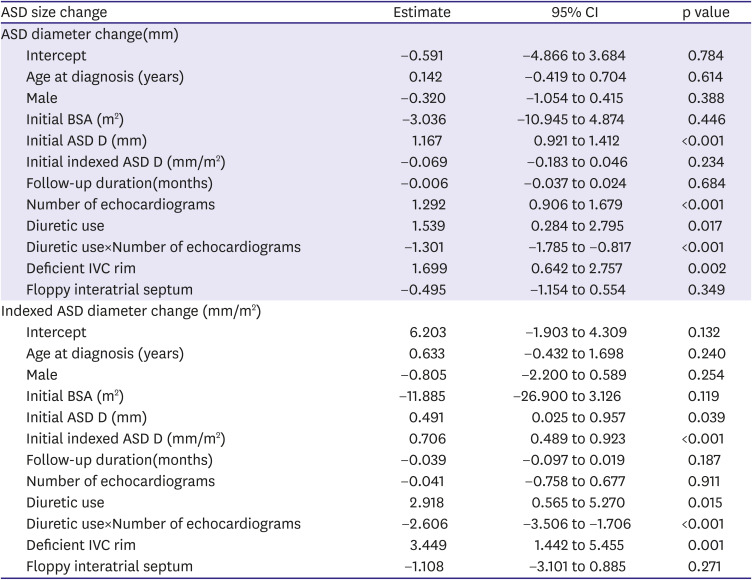
Table 2
Linear mixed model analysis for ASD diameter change and indexed ASD diameter change
ASD = atrial septal defect; ASD D = atrial septal defect diameter; BSA = body surface area; IVC = inferior vena cava.
![]()
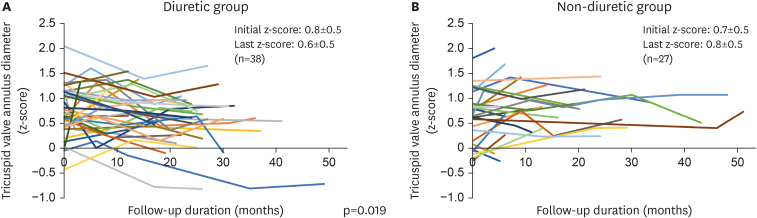
We assumed that the use of diuretics would be related to the difference in right atrium (RA)/RV dimensions, and to investigate this, we measured the tricuspid valve (TV) annulus diameter in a 4-chamber view on echocardiogram. And the z-score values of the TV annulus diameter were compared in the two groups.8) In the diuretic group, the TV annulus diameters of 38 patients were measured. The mean initial tricuspid annulus z-score was 0.8±0.5, and the last TV annulus z-score was 0.6±0.5. On the other hand, in the non-diuretic group, the TV annulus diameters of 27 patients were measured. The mean initial TV annulus z-score was 0.7±0.6, and the last TV annulus z-score was 0.8±0.5. The TV annulus z-score change showed a significant difference over time between the two groups. (p for interaction=0.019, Figure 3).
Furthermore, we investigated the characteristics of the three subgroups according to the ASD size change in the diuretic group. None of the clinical features including age, initial ASD size, and follow-up duration showed significant differences between the three groups (Table 3). Posterior rim deficiency was the only factor that showed significant differences between the groups (p=0.006). The decreased ASD size subgroup had no posterior rim deficiency; the stationary and the increased ASD size subgroups included 35.7% (n=5) and 64.3% (n=9) of the patients with posterior rim deficiency, respectively.
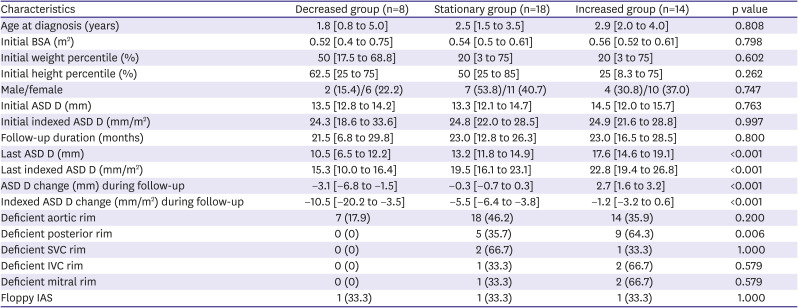
Table 3
Characteristics of each group according to ASD size change in the diuretic group
Values are median [25% to 75% range] or number (%).
Decreased group, patients with decreased ASD diameter; Stationary group, patients with unchanged ASD diameter (within ±1 mm); Increased group, patients with increased ASD diameter.
ASD = atrial septal defect; ASD D = atrial septal defect diameter; BSA = body surface area; IAS = interatrial septum; IVC = inferior vena cava; SVC = superior vena cava.
![]()
Growth-rate difference between the diuretic and non-diuretic groups
Table 4 shows the average body weight and height percentiles both in the diuretic and non-diuretic groups. While the initial weight and height percentiles were not significantly different, they tended to be higher in the non-diuretic group. Moreover, both the weight and height percentiles at the last measurement were not significantly different. Depending on the usage of diuretics, both the weight and height percentile changes over time did not show any significant difference between the diuretic group and the non-diuretic groups (p=0.11 and p=0.06, respectively).
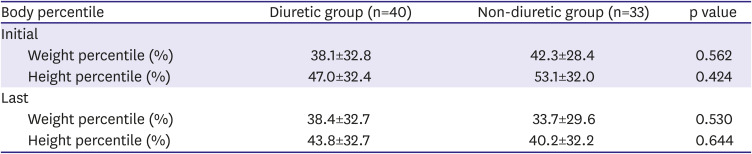
Table 4
Average percentiles of body weight and height in the diuretic group and non-diuretic group
![]()
Differences in the distribution of atrial septal defect treatment methods between the diuretic and non-diuretic groups
Figure 4 shows the distribution of the ASD treatments both in the diuretic and non-diuretic groups. Significant differences were observed for the distribution of treatments methods between the groups (p=0.001). In the non-diuretic group, surgery was the most commonly used treatment method (n=18 [54.5%]) followed by device closure (n=13 [39.4%]). The ASD size did not decrease to an extent that would render treatment unnecessary in any of the patients, while two patients were lost to follow-up. Conversely, in the diuretic group, 30 patients (75%) underwent device closure which was the most commonly used treatment method followed by surgery (n=6 [15.0%]). ASD size was reduced to a range that rendered treatment unnecessary in two patients in the diuretic group. A 6-month-old male patient whose initial maximal ASD diameter was 13.5 mm showed a decreased ASD diameter of 3.1 mm following 4.1 years of diuretic use. Another patient, a 2.1-year-old male individual, showed an initial maximal ASD diameter of 11 mm; following 1.6 years of diuretic use, it was decreased to 6.4 mm. The other two patients in the diuretic group were lost to follow-up.
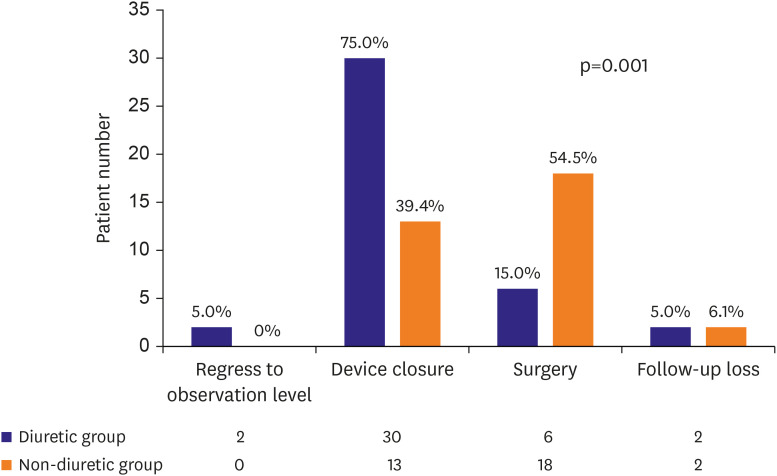
Figure 4
Distribution of ASD treatment in the two groups. The treatment distribution for ASD according to the diuretic administration. The patients with diuretics underwent more non-invasive treatments such as observation or device closure than surgical closure with statistical significance (p=0.001).
ASD = atrial septal defect.
![]()
DISCUSSION
In this study, diuretic administration seemed to be associated with changes in ASD size in pediatric patients with a large secundum ASD. In addition, it may be associated with reducing the need for early surgical ASD closure and increasing the rate of transcatheter closure. To the best of our knowledge, no studies have focused on effect of diuretics on ASD size changes until now.
The success rate of transcatheter ASD closure is approximately 95%, with the feasibility and safety of the technique being previously established.9)10) The prevalence rate of complications is favorable, as it is 1% in the case of transcatheter ASD closure.11)12)13) Accordingly, transcatheter secundum ASD closure is preferred over surgery and is being attempted at a younger age;2)14)15)16) however, recent studies reported both lower periprocedural success rates and an increased risk of periprocedural and long-term complications with the use of transcatheter closure either when body weight is ≤15 kg or in the presence of a large secundum ASD (≥20 mm/m2).11)17)18) Therefore, for improved procedural success rates and reduced complication rates, it is reasonable to delay the procedure until the weight is approximately 15 kg.
In general, when the ASD diameter is ≥10 mm, it is known to cause a significant L-R shunt, resulting in RV volume overload.2) We used diuretics for RV volume unloading and expected to use a smaller sized device later through ASD size reduction. We hypothesized that the use of diuretics reduces preload and cause RA and RV volume unloading, thereby reducing the overall RA and RV dimensions and ASD diameter, thus making it possible to use a smaller device. In reality, as shown in Figure 3, the TV annulus z-score showed a significant difference over time between two groups according to the use of diuretics.
In our study, the ASD size was significantly reduced in the diuretic group compared with the non-diuretic group, and even two patients in the diuretic group showed an ASD size decrease to a level that rendered treatment unnecessary.19)
Diuretics are used to reduce preload in some patients with CHD.20) Although there are some concerns about hearing loss associated with the use of high doses of furosemide, recent studies have reported that furosemide and hearing loss are not significantly associated.21)22)23)24) There is still no clear evidence for complications from long-term use of oral diuretics in children and may be controversial. While concerns might exist regarding the long-term use of diuretics, there were no complications, including those regarding growth retardation at the diuretic dose within 1 mg/kg/day that we used.
We investigated the diuretic group by dividing it into three subgroups according to the response to diuretics (Table 3). In the three groups, clinical features did not show any significant difference, and only posterior rim deficiency showed a significant difference and did not have a chance of ASD diameter decrease. The characteristics of the three subgroups according to the ASD size change in the non-diuretic group are presented in Supplementary Table 1. We found that the ASD size was increased in all patients with posterior rim deficiency in the non-diuretic group. Moreover, all patients with IVC rim deficiency showed an increased ASD diameter in the non-diuretic group. In this study, ASD size reduction was not found in patients with posterior rim deficiency, even among those who received diuretics. Therefore, for patients with posterior rim deficiency, the use of diuretics is likely to be partially effective.
In addition, in our patient group, the number of patients with IVC rim deficiency was significantly higher in the non-diuretic group (7.5 vs. 42.4%, p=0.01), and this difference in distribution of rim deficiency between two groups may have an effect on the difference in treatment trends. So, we investigated whether the distribution of treatment methods was different in the diuretic group and the non-diuretic group even within each subgroup with rim deficiency (Supplementary Table 2). Since the number of patients in each subgroup is small, there is a limit for analysis, however, when looking at patients with posterior rim deficiency, there was a significant difference in treatment distribution between the diuretic and the non-diuretic group (p=0.046). In addition, while all patients with IVC rim deficiency in the non-diuretic group underwent surgery, one patient in the diuretic group was able to undergo successful device closure, although the number of patients was limited to evaluate it. However, there is still no clear explanation for the relationship between rim deficiency and diuretic effect. Nonetheless, as shown in our data, regardless of the diuretic use, there seemed to be a little possibility of ASD size reduction in case of rim deficiency other than the aortic rim.
Notably, in this study, the mean ASD diameter remained unchanged while the indexed ASD diameter in the diuretic group decreased significantly compared to that in the non-diuretic group. Therefore, in the non-diuretic group, the ASD size increased in accordance with the increase of body growth; However, the use of diuretics seemed to be associated with preventing an increase in the ASD size according to body growth.
While the effect of diuretics on reducing the ASD size and the resulting outcomes may vary across patients, our data showed that the patients in the diuretic and non-diuretic groups showed significantly different treatment distribution patterns (p=0.001, Figure 4). The patients with diuretics underwent more non-invasive treatments such as observation or device closure than surgical closure. In addition, even within the diuretic group, the distribution of treatment methods differed depending on whether the patients responded to diuretics (p=0.016, Supplementary Figure 1). In the group with a decreased ASD size following the use of diuretics, none of the patients underwent surgery. However, 5.6% and 35.7% of the patients in the stationary and the increased groups, respectively, underwent surgery. A patient's response to diuretics positively correlated with the probability of transcatheter device closure than surgical closure.
We investigated patients who underwent surgery in both groups (Supplementary Table 3). If the ASD size was relatively large and had several rim deficiencies including posterior rim deficiency at the same time, surgical closure was performed more frequently. Though device closure could have been performed in some cases, the surgery was performed according to the preference of the physician or the request of the patients with the large ASDs with several rim deficiencies.
Interestingly, the weight and height growth rates over time did not show any significant difference in the two groups. Of course, it is premature to conclude that the growth rate was not retarded in the diuretic group only from our data, but at least the likelihood of developing specific side effects from diuretic use does not appear to be alarmingly high.
Our study has several limitations. Because of its retrospective design, the potential presence of various biases including selection bias cannot be completely excluded. We included patients with a follow-up period of approximately 6 months or longer, excluding those who were treated immediately after diagnosis, and the follow-up period was similarly matched in both groups. However, it cannot be completely excluded that the consideration of the timing of treatment may have influenced the decision to take diuretics. Additionally, since the total number of patients and the number of patients in each subgroup were small, limitations exist regarding the evaluation of the effect of diuretics, which necessitates the need of randomized controlled trial to get more concrete evidence of the effect of diuretics on ASD size reduction; however, we observed statistically significant differences in the degree of ASD size reduction in diuretic compared to the non-diuretic group.
In pediatric patients with a large secundum ASD (diameter ≥10 mm), diuretic administration seems to be associated with changes in ASD size. The patients receiving diuretics may have a lower possibility to undergo surgical closure. The diuretics administration may be associated with the use of smaller ASD devices for transcatheter treatment through ASD size reduction.
 XML Download
XML Download