

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the novel coronavirus disease 2019 (COVID-19) was first reported in Wuhan, China in December 2019,1 it has rapidly spread worldwide as a global pandemic.2 According to the World Health Organization (WHO), COVID-19 has affected 223 countries, territories and areas with 190 million confirmed cases and 4.0 million deaths (as of July 21, 2021).3 In South Korea, the first case was identified on January 20, 2020, and as of July 21, 2021,4 COVID-19 has infected 182,265 people, resulting in 2,060 deaths.5 To control the pandemic, the Korean government has declared the highest level of public health emergency alert, and has taken rapid and comprehensive actions to limit its spread.6 The actions included enacting strict quarantine measures, improving case identification, patient diagnosis and treatment, as well as logistic support and establishing units for quarantined patients.78
During this nationwide crisis, healthcare workers (HCWs) have played a pivotal role on the frontlines.9 The distress of the HCWs responding to COVID-19 cannot be ignored. HCWs represent the frontline workers during this unprecedented crisis, treating patients with COVID-19 and attempting to prevent contagion. Pandemics, in general, expose HCWs to heavy workloads and work-related stresses. Specifically, HCWs are at a high risk of infection, and the fear of infection can pose a psychological burden.10 Evidence suggests that frontline HCWs inevitably face tremendous psychological burden in an infectious disease environment, similar to severe acute respiratory syndrome (SARS).1112 During recent Ebola outbreak, an unprecedented number of HCWs were infected, and survivors endured higher rates of post-traumatic stress disorder (PTSD).13 A systemic review conducted during COVID-19 outbreak reported that the fear of being infected and other unfavorable conditions, such as increasing number of confirmed cases, excessive workload, shortage of personal protective equipment, and intense media scrutiny, increase the risk of psychological distress among the HCWs.14 Another systematic review reported that the prevalence rates of anxiety, depression and insomnia among the HCWs were 23.2%, 22.8% and 38.9%, respectively.15 Since HCWs represent a particularly vulnerable group to infection, many studies identified that the fear of spread to family members increases work-related stress.16
The psychological distress not only increases the burden on the health and well-being of the HCWs but also hinders their ability to effectively manage infectious diseases, like COVID-19.17 However, the psychological impact on HCWs during infectious disease outbreaks, especially during COVID-19 on HCWs, has yet to be established.18 Therefore, the present study was conducted to identify the factors that likely increased the psychological distress due to COVID-19 on the HCWs. Data were collected by HCWs who have worked in a cohort of Daenam Hospital, which reported a cluster COVID-19 infections in Korea in January 2020.
Go to : 
METHODS
The Daenam Hospital cluster infection was first confirmed at a medical institution in Korea, and identified in February 21, 2020. The Korean Ministry of Health and Welfare dispatched HCWs from the National Hospitals to manage according to the institutional guidelines.7 Among 104 cases of COVID-19 infection, 92 were confirmed and 12 were not but were classified as close contacts. Antiviral treatment was administered to the confirmed cases. Following proper treatment completion, patients were considered recovered and transferred to Bugok National Hospital (BNH) for further observation and treatment of residual psychiatric symptoms. Close contacts were transferred to BNH and quarantined under close monitoring for 2 weeks. Further confirmation during the quarantine period led to the patient's transfer to an institution equipped for COVID-19 treatment; otherwise, they were released from quarantine and treated for psychiatric residual symptoms at BNH. Care for confirmed and close contacts of COVID-10 was provided by HCWs at BNH from February 21, to March 6, 2020.
Measures
We collected participants' sociodemographic data including age, gender, marital status (single/divorced or married), having child, cohabitation, and years of work experience. Psychometric scales to identify emotional distress, depression, and PTSD-related symptoms were evaluated. Finally, a questionnaire was used to collect information regarding work experience during the Daenam Hospital cluster infection.
The 12-item General Health Questionnaire (GHQ-12)
The GHQ-12 is a self-administered screening tool and a frequently used and well-standardized measure of recent subjective quality of life and emotional distress.19 The GHQ-12 consists of 12 items measured on a 4-point Likert scale (score rage = 0 to 3) with the responses “less than usual,” “no more than usual,” “rather more than usual,” and “much more than usual.” We coded the response categories on the GHQ-12 items using the GHQ-12 scoring method as recommended by Goldberg and Williams20 and calculated a total score. The reliability and validity of the Korean version of GHQ-12 were previously confirmed (Cronbach's α = 0.79).21 In the Korean version, a total score of greater than 3 was used to detect emotional distress manifested as a break from normal functioning.22 In this study, participants were categorized into distress and non-distress groups based on the results of GHQ-12.
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is an instrument enabling criteria-based diagnoses of depression in primary care.23 PHQ-9 consists of 9 items measured on a 4-point Likert scale (score range = 0 to 3) with responses “not at all,” “several days,” “more than half the days,” and “nearly every day.” Depending on the total score, 0–4 points, 5–9 points, 10–14 points, 15–19 points, and 20–27 points, patients' depression level was classified as none, mild, moderate, moderately severe, and severe, respectively. PHQ-9 has been formally translated into Korean, and the reliability and validity of the Korean version were reported previously (Cronbach's α = 0.93).24
Impact of Events Scale-Revised (IES-R)
The IES-R is a self-reported measure of subjective distress resulting from traumatic events that is distinct from daily life, and useful diagnosing and identifying the severity of PTSD.25 IES-R consists of 22 items measured on a 5-point Likert scale (score range = 0 to 4) with responses “not at all,” “a little bit,” “moderately,” “quite a bit,” and extremely.” IES-R has been formally translated into Korean, and the reliability and validity of the Korean version were confirmed previously (Cronbach's α = 0.93).26 A total score equal to or > 25 in the Korean version was suggestive of a diagnosis of PTSD, and a score equal to or > 18 was indicative of PTSD-like symptoms.
Questionnaire about work experience
A supplementary questionnaire consisting of 17 items was administered to survey the working experience during exposure to COVID-19. It was modified from a previous version developed for the hospital staff during the 2003 SARS.2728 This questionnaire alone cannot be used to diagnose or assess the severity of psychiatric conditions, including emotional stress. However, based on previous studies, it provided a comprehensive insight into the sources of distress among hospital staff under the infectious disease environment. It contains subjective elements of evaluation of hospital staff based on their perception of threat, acceptance, and concerns during the work. The questionnaire was assessed on a 4-point Likert scale (score rage 1 to 4) with responses “strongly disagree,” “disagree,” “agree,” and “strongly agree.”
Statistical analysis
All assessment scores were compared between the two groups (distress and non-distress) according to results of GHQ-12. Independent t-tests were used to evaluate the statistically significant differences between the groups in terms of the means of continuous variables. The χ2 analysis was used as a contingency test to assess statistically significant differences in categorical variables. The continuous variables were tested for the normality of distributions via the Shapiro-Wilk test, to identify the skew and kurtosis. Levene's test was performed to determine the homogeneity of variance. The effects of potential confounding variables were adjusted according to the mean of analysis of covariance (ANCOVA). A binary logistic regression model was constructed to identify factors associated with the likelihood of emotional distress, defining the distress group as the dependent variable and the non-distress group as the reference. Initial covariates selected for binary logistic model were variables that differed significantly between the distress and non-distress groups. Standard methods such as goodness of fit, which was controlled for interaction and colinearity, were used to select and validate the final model. Logistic regression was based on a forward selection method to avoid colinearity. Significance was set at P < 0.01 (two-tailed) for all tests, to reduce familywise error due to multiple comparisons. All statistical analyses were performed using SPSS 25.0 for Windows (IBM Corp., Armonk, NY, USA).
Ethics statement
A total of 99 HCWs (5 doctors, 71 nurses, and 23 certified nurse assistants) at BNH participated in the study. All participants voluntarily agreed to participate in the survey and written informed consent was obtained after the study's purpose and methodology were explained to them. Data from those caring for confirmed cases and close contacts were collected, when their work commitments were completed (March 10, 2020). The present study was approved by the Institutional Review Board of BNH (No. 2020-06).
Go to :
RESULTS
As shown in Table 1, the prevalence of emotional distress among 99 participants was 45.5% (n = 45). Distress group was more likely to be female involved in managing close contacts (χ2 = 11.428, P = 0.001 and χ2 = 5.556, P = 0.018, respectively). In addition, there were more cases of younger, single, without children, living alone, and with shorter work experience, but no statistically significant difference existed. Hence, based on the ANCOVA for continuous variables, the differences between the two group were determined after adjusting for the effect of gender and managing close contacts.
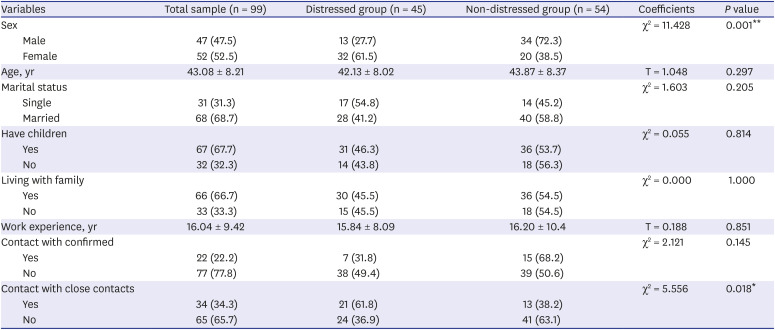
Table 1
Baseline demographics of distressed and non-distressed groups
![]()
Assessment scales and questionnaires: distressed vs. non-distressed groups
Among all participants, 33.3% (n = 33) reported a score of 10 or more in PHQ-9, and 26.7% (n = 27) reported a score of 18 or more in IES-R. As shown in Table 2, the group with emotional distress reported statistically significantly higher scores on PHQ-9 (F = 12.698, P = 0.001) and IES-R (F = 4.420, P = 0.038) than emotionally non-distressed group. In the questionnaire about work experience, the emotionally distressed group responded with higher scores involving item 1 ‘I feel unsafe working at my workplace (F = 7.176, P = 0.009),’ item 3 ‘I feel at risk to contact a COVID19 infection at work (F = 4.376, P = 0.039),’ item 6 ‘If optional, I would have chosen to work in another unit (F = 6.298, P = 0.014),’ item 7 ‘I feel COVID-19 crisis increased my workload (F = 5.672, P = 0.019),’ and item 11 ‘I feel proper infection control training was not provided to me (F = 6.789, P = 0.011)’ compared with the emotionally non-distressed group.
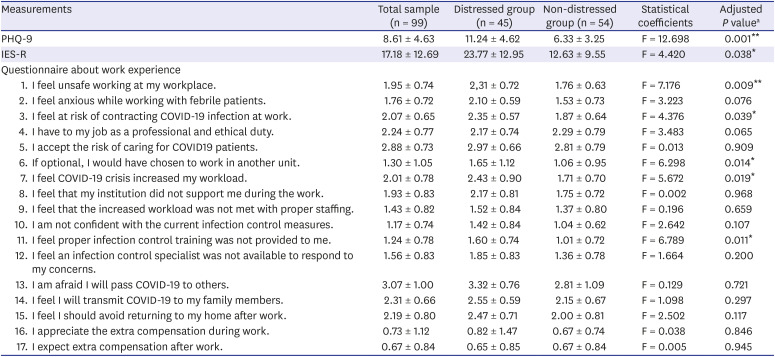
Table 2
Assessment scales and questionnaires of the distressed and non-distressed group
Values are presented as mean ± standard deviation.
PHQ-9 = Patient Health Questionnaire-9, IES-R = Impact of Events Scale-Revised, COVID-19 = coronavirus disease 2019.
aAdjusted for the effects of gender and contact with close contacts, *P < 0.05, **P < 0.01.
![]()
A binary logistic model for predicting emotional distress of HCWs
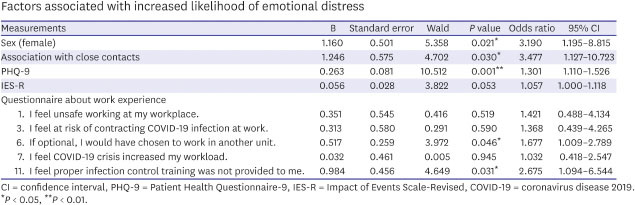
The results of a binary logistic regression model were used to identify factors associated with emotional distress involving HCWs. The Homsmer-Lemeshow goodness-of-fit test reinforced the accuracy of the logistic model (χ2 = 6.220, df = 8, P = 0.623). The initial covariates in the binary logistic model were gender, managing close contacts, total scores of PHQ-9 and IES-R, and scores on the questionnaire about work experience including item 1‘I feel unsafe working at my workplace,’ item 3 ‘I feel at risk to contact a COVID19 infection at work,’ item 6 ‘If optional, I would have chosen to work in another unit,’ item 7 ‘I feel COVID-19 crisis increased my work load,’ and item 11 ‘I feel proper infection control training was not provided to me.’ Forward selection of the model was performed to avoid issues associated with multicollinearity. As shown in Table 3, the final model explained 62.3% (Nagelkerke R2) of the variability in emotional distress, and showed that female gender (odds ratio [OR], 3.190; 95% confidence interval [CI], 1.195–8.815; P = 0.021), managing close contacts (OR, 3.477; 95% CI, 1.127–10.723; P = 0.030), a higher score on the PHQ-9 (OR, 1.301; 95% CI, 1.110–1.526; P = 0.001), and questionnaire about work experience such as item 6 ‘If optional, I would have chosen to work in another unit (OR, 1.677; 95% CI, 1.009–2.789; P = 0.046),’ and item 11 ‘I feel proper infection control training was not provided to me (OR, 2.675; 95% CI, 1.094–6.544; P = 0.031)’ were independently associated with and increased the likelihood of emotional distress among HCWs.
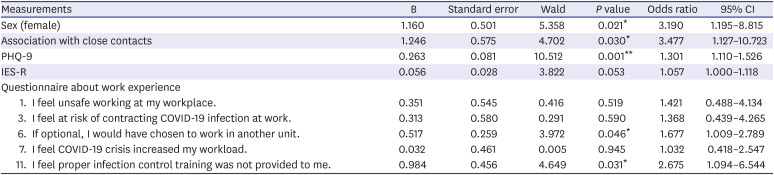
Table 3
Factors associated with increased likelihood of emotional distress
CI = confidence interval, PHQ-9 = Patient Health Questionnaire-9, IES-R = Impact of Events Scale-Revised, COVID-19 = coronavirus disease 2019.
*P < 0.05, **P < 0.01.
![]()
Go to :
DISCUSSION
Emotional distress was observed among 45.3% (n = 45) of the 99 HCWs who worked with a cohort of cluster infection at Daenam Hospital. The emotionally distressed group of subjects, compared with the non-distressed group, was more likely to be female, managing close contacts, higher scores on PHQ-9 and IES-R, a feeling of increased risk associated with coronavirus disease-related jobs and proper infection control training was not provided. Logistic regression analysis revealed that female gender, managing close contacts, higher scores on PHQ-9, and a feeling of proper infection control training was not provided were associated with emotional distress.
The rates of emotional distress, depressive symptoms, and PTSD-like symptoms among the participants were 45.5%, 33.3%, and 27.6%, respectively. In a systematic review of psychiatric symptoms on HCWs during the COVID-19 pandemic reported a prevalence rate of psychological impact ranging between 16.5% and 38.3%, which is similar to the results of this study.14 Accordingly, a study from Wuhan, China reported that 14.8% of HCWs experienced moderate-to-severe depression based on PHQ-9 results, and the rate of depression was higher in this study.29 However, it was similar to a study from Daegu, which was designated as an early epicenter for the outbreak of COVID-19 in Korea.30 The difference might be attributed to the Chinese study investigating 34 hospitals, including those at the fringes of Wuhan, whereas our study focused on a single institution. Additionally, in the other studies, nurses showed the highest risk of depression,1429 and most of the participants in this study were nurses, which may explain the difference.
Several studies reported that PTSD was the most common health condition among the HCWs.31 However, in this study, PTSD-like symptoms were not a statistically significant factor contributing to emotional distress among the HCWs. A study of 1,800 HCWs investigated the psychological impact during the initial stages of the Middle East respiratory syndrome (MERS) outbreak and one month later. Those who performed MERS-related tasks reported greater distress, and interestingly, increased the risk of PTSD symptoms after one month.32 In this study, the PTSD-like symptoms were evaluated at the beginning of the exposure, and a re-evaluation was deemed necessary after a period of time.
In particular, female HCWs who managed close contacts experienced higher levels of emotional distress. In many other studies, female nurses in close contact with COVID-19 patients appeared to manifest the highest mental health risk, specifically, the female gender enhanced the risk of depression, anxiety and contributed to higher levels of stress.3334 Although the duration of follow-up was not specified in most studies and no long-term support for HCWs existed,35 prompt utilization of interventions promoting the well-being of the HCWs facing COVID-19 was suggested for frontline workers, females and nurses.28 However, it is important to note that most studies included predominantly female participants, especially nurses, with only one study suggesting higher stress levels amongst males.36
It is interesting that HCWs who managed close contacts reported increased emotional distress. In this study, the work environment was not qualified, the HCWs who managed confirmed cases wore excessively protective equipment and reported a higher frequency of close contact with infected patients.37 Another study including 385 HCWs reported contact with confirmed and suspected patients, which were significant predictors of depression in HCWs, but only contacts with suspected patients were significant predictors of anxiety and stress.38 In addition, HCWs who had contact with patients diagnosed with suspected COVID-19 exhibited higher levels of depression, anxiety and stress. Further investigations are needed to corroborate these findings; however, uncertainty may have played an important role. Feelings of uncertainty are a central feature associated with a disastrous experience, and positively correlated with symptoms of PTSD, depressive symptoms, quality of life, fatigue and pain among disaster survivors.39 Indeed, some patients who were classified as close contacts and quarantined had repeated fever and respiratory symptoms. Finally, two out of 12 quarantined close contacts were confirmed at the end of the quarantine period, which may have increased the emotional distress of HCWs.
During a pandemic, the demands on HCWs are extraordinary and work-related stress disproportionally affects their health and well-being due to the excessive workload.40 However, the results of this study indicate that altered or increased workload was not directly related to emotional distress.
The item related to work experience including ‘I feel proper infection control training was not provided to me’ significantly increased the emotional distress. Lessons learned from the SARS outbreak in 2003 suggest that knowledge and attitudes towards infectious diseases are associated with panic levels among the population, which can further complicate attempts to prevent the disease spread.41 Multiple logistic regression analyses revealed that the COVID-19 knowledge score was significantly associated with a lower likelihood of negative attitudes and preventive practices towards the pandemic.42 HCWs lacking adequate knowledge or skills involving protective or preventive measures experienced higher levels of fear and reported increased difficulties associated with activities of their daily living.4344 Several studies, consistent with the results of this study, underscored the need for greater support through collaboration, training and education of HCWs involved in infectious disease management.4546 Appropriate education in COVID-19 infection prevention has been shown to enhance the optimism of HCWs and maintain appropriate practices, by decreasing the stress levels.4748
Many studies reported increased stress associated with the risk of disease spread among the family members of HCWs, similar to our study findings, which was a concern.16 However, in this study, there was no difference between the two groups. All participants were provided with an independent living space while working, and quarantined for two weeks after dispatch to another facility, and therefore it may not have affected their emotional distress.
It was also interesting that the higher scores of a questionnaire item regarding work experience involving ‘If optional, I would have chosen to work in another unit’ had a significant effect in increasing the emotional distress, and it may be related to occupational satisfaction. Lee et al.10 reported that occupational stress consists of four domains overwhelmed by heavy workloads, fear of infection, lifestyle changes, and psychological and physical struggles in a qualitative analysis after interviewing HCWs who directly or indirectly cared for patients during the COVID-19 epidemic. Regarding this, additional research is needed to identify the HCWs condition by as subdividing work stress domain and quantifying the work environment. In addition, psychological preparedness is necessary as a coping strategy for HCWs facing threats of natural and man-made disasters.49 The level of psychological preparedness is reflected by the degree of acceptance or willingness to perform their work.50 The association between acceptance and protection against psychological distress due to infectious disease has yet to be investigated fully. Several surveys have reported this quality frequently among HCWs, and studies have associated the intent to help with resilience against psychological disturbances like PTSD.51 A study involving hospital employees affected by the SARS outbreak reported that the acceptance of risk was negatively associated with current fear and negative impact of SARS.12 Although participants in this study scored highly on work experience-related items such as ‘I accept the risk of caring for COVID19 patients,’ a further study analyzing the effect of acceptance level on emotional distress is needed. The results of a recent review indicate that the availability of personal protective equipment/vaccine, level of training, professional ethics, family and personal safety, and worker support systems should also be evaluated.52
The study has several limitations. First, only the HCWs working at a single medical institution were included, and the sample size was small. Second, the assessment was based on self-report only, and due to the absence of a standardized tool of measurement, the work experience was evaluated using a self-administered questionnaire used in previous similar studies. Third, most of the participants were nurses, and analysis according to occupational type was not conducted. Fourth, detailed symptoms such as sleep disturbance or somatic symptoms that directly affect the emotional distress and personal characteristics such as moral injury or resilience were not evaluated. Fifth, the study does not provide details of working hours or exposure frequency. Finally, many HCWs were quarantined after work, which prevented face-to-face interviews. The study employed a cross-sectional design within 2 weeks and did not assess the symptoms of psychological stress in the following period. Nevertheless, this study identified the emotional distress of the HCWs engaged in the management of COVID-19 cases.
During the current COVID-19 pandemic, the first-line HCWs play a leading role in the fight against the COVID-19 outbreak. Inevitably, the frontline HCWs operate under great psychological stress and face many challenges and losses, along with tremendous psychological burden under an infectious disease environment. Therefore, the results of this study underscore the need for appropriate psychological interventions for HCWs involved in COVID-19 management.
Go to :
 XML Download
XML Download