

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With the rapid spread of the coronavirus disease 2019 (COVID-19) worldwide in a short period of time, the World Health Organization declared COVID-19 as a pandemic on March 11, 2020.1 COVID-19 was first reported in December 2019 in Wuhan, China, while the first case in South Korea was reported on January 20, 2020.23 Daegu, one of the largest cities in Korea, became a large scale local infected area in February 2020 with the rapid increase of confirmed COVID-19 cases in religious groups and long-term care facilities, with cumulative confirmed cases exceeding 6,000 (more than 68% of the nation's confirmed cases) by the end of March 2020.4 Finally, Daegu was declared a special disaster area on March 15, 2020.56
COVID-19 is a respiratory disease caused by a new coronavirus, called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).7 In addition, COVID-19 is so highly contagious that it is spreading rapidly around the world,8 which has a significant impact on individual lives throughout the world, including society, economy, culture, and education.9101112 In particular, many researchers have reported that the COVID-19 pandemic, which continues to exist today, is affecting many individuals psychologically and emotionally aside from its physical effects.13 A recent meta-analysis analyzed 66 studies and reported that 31.5% of the general population experienced depression, 29.8% experienced anxiety, 31.1% experienced distress, and 18.2% experienced insomnia.14 Brooks et al.15 also reported that quarantines due to COVID-19 have negative psychological effects on individuals, and the stressors affecting these negative feelings include long periods of quarantine, concerns about infections, frustration, and inappropriate information.
Students in the process of development are also affected psychologically due to COVID-19, who experience stressors such as school closure, lack of contact with peer groups, and changes in sleep patterns.1617 Childhood and adolescence are critical periods to be affected by the external environment, and mental illness such as depression, anxiety, and posttraumatic stress are reported as negative effects of COVID-19.1819 In many studies, students reported that changes in school life caused by COVID-19, such as online classes and homeschooling, have increased mental problems (e.g., internet addiction) and negative emotions (e.g., anxiety and depression), as well as worsened psychiatric diseases such as attention deficit hyperactivity disorder and obsessive-compulsive disorder.202122 However, no large scale study has investigated the psychological effects of COVID-19 across the entire region on adolescents at the time of the regional spread of COVID-19. Evaluating the psychological and mental state of the victims after a disaster allows for early interventions in this mental health crisis, preventing its occurrence and aftereffects. Furthermore, a large scale study would contribute to the development of mental health correspondence manuals and determination of mental health policies in present and future disasters.232425 The Daegu Metropolitan Office of Education commissioned the Daegu Student Suicide Prevention Center to conduct a survey of local middle and high school students’ mental health in May 2020, about 2–3 months after COVID-19 spread to the highest level, and released the results on August 31, 2020.26 In the current study, we analyzed this data to identify the changes and causes of students' psychological crisis before and during the ongoing COVID-19 pandemic, and to find out the coping strategies of their psychological crisis.
Go to : 
METHODS
In this study, we retrospectively analyzed the data of the “COVID-19 related school mental health assessment project” released by the Daegu Metropolitan Office of Education on August 31, 2020, with the approval of the institution.
Survey design and performance
The survey was conducted by the Daegu Student Suicide Prevention Center at the request of the Daegu Metropolitan Office of Education. This included 3–7 schools from each of the eight districts of Daegu, with appropriate representation considering the number and types of schools in the area. The selected schools reflected the socioeconomic status, students’ grades, and the results of the emotional behavior characteristics test of each district. The proportion of male and female, as well as general high school and non-general high school (e.g., characterization high school) students in each district were constant. From each school, 150 students (50 students from each grade) were selected at random, leading to a total of 12,300 students in this study: 6,450 students from 43/124 middle schools and 5,850 students from 39/93 high schools. The research team of psychology in Daegu Catholic University (Chang-gu Huh, research director) conducted the survey using the online survey platform of the Korea Social Science Data Center from May 29 to June 14, 2020.
The survey begins with a question asking about demographic characteristics, consisting of three main areas: health status, COVID-19 experience, and current emotional status and adaptive status. The survey was expected to take an average of 10–20 minutes. Prior to the survey, the Daegu Metropolitan Office of Education informed the students and their parents about its contents, specifically regarding the purpose of the study, participating subjects, adverse effects from the survey, and confidentiality of personal information; the survey was conducted only with their consent.
Among the survey subjects (12,300 students), 4,843 (75.08%) middle school students and 7,176 (71.38%) high school students responded. After excluding those who responded insincerely, the final analysis included 4,463 (69.19%) middle school students and 3,714 (63.48%) high school students. The response rate of this study was 66.5% (8,177/12,300).
Survey materials
Demographic characteristics and health status
The questionnaires were developed to compare the demographic characteristics of the subjects and to understand the effect of these factors on mental health and data were collected. The questionnaire contains 13 questions about the gender, school, grade, residence, school location, family information, and religion of the participants. The questionnaire also contains 13 questions regarding health status, specifically about the presence of experience of a confirmed diagnosis of COVID-19 and isolation for students and their family members, the physical health status, the experiences of psychiatric clinic visits before and during the COVID-19 pandemic, and the experiences of unbearable stress at three points: before December 2019 (“before the COVID-19 pandemic”), after January 2020 (“at the peak time of COVID-19 contagion”), and May-June 2020 (“present”). The subjects were asked to identify at which points in time they experienced unbearable stress. The term “unbearable stress” was described in the survey as stress that cause psychological and physical reactions that are serious enough to affect daily life or study beyond the scope of your control. We asked the participants in the questionnaires as follows: “Were there any unbearable stresses before the COVID-19 pandemic,” “Were there any unbearable stresses at the peak time of COVID-19 contagion,” “Were there any unbearable stresses at present.” The participants were asked to respond with “yes” or “no.”
Experiences related to COVID-19
A total of 39 questions about experiences related to COVID-19 were asked, including the degree of basic knowledge of COVID-19 and the presence of experiences of emotional crisis during the three time periods. Participants who responded that they experienced an emotional crisis were asked about the possible causes and their coping strategies at each time period. In the survey, the term “emotional crisis” was described as “a state in which negative emotions were felt for any reason, making it difficult to control yourself.” Participants were asked the question in the questionnaire as follow: “Have you experienced an emotional crisis since the spread of COVID-19? They were asked to respond with “yes” or “no.” Students who responded that there was an emotional crisis were asked to choose three of the 16 causes (family conflict, delinquent and deviant behavior, academic/career concerns, sexual problems, personality problems, conflict with peers, social withdrawal, conflict with teachers, dating relationship, mental health, lifestyle change, unsatisfied appearance, internet conflicts, paucity of information, lack of outdoor activity, others) extracted from the preliminary survey on the factors that cause the emotional crisis.
Assessment scales
The Korean version of the Patient Health Questionnaire 9
The Patient Health Questionnaire 9 (PHQ-9) is a depression screening tool developed by Spitzer et al.27 in 1999 and has since been verified for its reliability and validity. The PHQ-9 consists of nine questions, each scored from 0 to 3, with a total score of 0–27. The total scores are classified either as mild (5–9 points), moderate (10–19 points), or severe (20–27 points), with 10 points set as a cut-off score for the presence of depressive symptoms. The internal consistency reliability of PHQ-9 is Cronbach's alpha = 0.84. In this study, the Korean version of PHQ-9 was used to assess for depressive symptoms in the subject students.28
The Korean version of the Generalized Anxiety Disorder 7
Generalized Anxiety Disorder 7 (GAD-7) is a tool used to assess the severity of symptoms of and screening for generalized anxiety disorder developed by Spitzer et al.29 in 2006 and has since been verified for its reliability and validity.30 Aside from generalized anxiety disorder, its usefulness in various anxiety disorders has also been verified. The GAD-7 consists of seven questions, each scored from 0 to 3 on a 4-point Likert scale, with a total score of 0–21. The total scores would indicate either mild (5–9 points), moderate (10–14 points), or severe (15–21 points) anxiety. The cut-off score for the presence of anxiety was set at 8 points by Plummer et al.31 In this study, the Korean version of GAD-7 was used to assess anxiety symptoms in the subjects.32
Youth Resilience Scale (YRSQ-27)
The Youth Resilience Scale (YRSQ-27) is a set of 27 questions developed in 2009 by Shin et al.33 to determine resilience to stress in adolescents. It is a five-point Likert scale, with higher scores indicating higher resilience. The validity and reliability of the tool have been identified at an appropriate level.
Statistical analysis
SPSS 25.0 version (IBM SPSS, IBM Corp., Armonk, NY, USA) was used for analyzing the data. First, frequency analysis and chi-square tests were conducted to analyze the demographic data from the 8,177 survey respondents. Second, a frequency analysis for experiences related to health and COVID-19 and a χ2 test for comparisons between categorical data were conducted. Lastly, a logistic regression test was conducted for 625 students who experienced an emotional crisis to identify the factors affecting depression and anxiety; cut-off scores of 10 for PHQ-9 and 8 for GAD were used to identify the presence of depression and anxiety, respectively. The analysis was conducted by designating the demographic data, resilience, and factors that affected the emotional crisis as independent variables. Statistical significance was set at 0.05.
Ethics statement
This study is a retrospective data analysis study that utilized open survey data and did not collect or record personal identification information; this study is exempted from deliberation by the Institutional Review Board because the risk to the subject is insignificant. The present study protocol was reviewed and approved by the Institutional Review Board of the participating hospitals and Kyungpook National University Chilgok Hospital (Reg. No. 2020-12-004).
Go to :
RESULTS
Participants and demographic data
Of the 8,177 participants in the research data, there were 4,072 (49.8%) males and 4,105 (50.2%) females. There were 4,463 (54.6%) middle school students (first grade: 1,594 [19.5%], second grade: 1,512 [18.5%], third grade: 1,357 [16.6%]) and 3,714 (45.4%) high school students (first grade: 1,388 [17.0%], second grade: 1,259 [15.4%], third grade: 1,067 [13.0%]). Among them, 7,142 (87.3%) students had both parents, while 1,035 (12.7%) had only one parent. There were 2,414 (29.5%) students with a religion. There were 351 (4.3%) students who experienced dealing with a case of confirmed COVID-19 (Table 1).
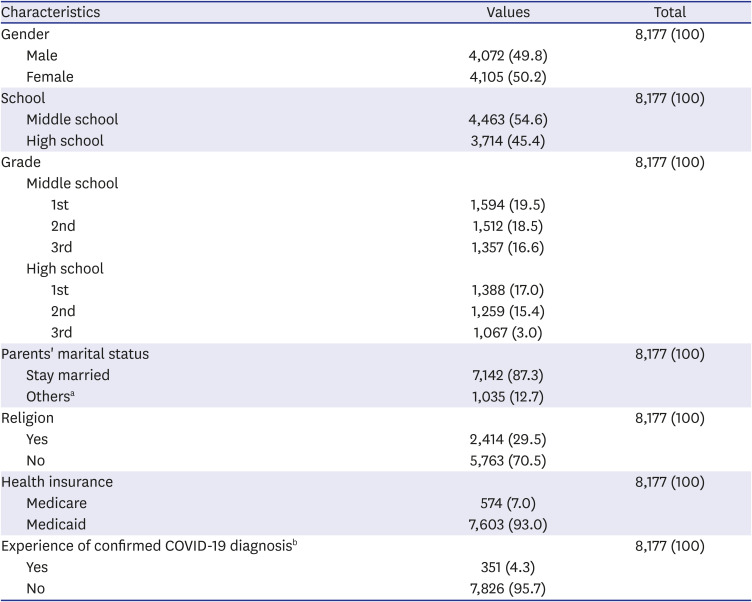
Table 1
Participants and demographic data
Values are presented as number (%).
COVID-19 = coronavirus disease 2019.
aIn a case where there is a change in marriage relationship due to separation, divorce, bereavement, etc.
bIt means that students or their family have been diagnosed with COVID-19.
![]()
Experiences of unbearable stress
Unbearable stress experiences were present in 9% of subjects before the COVID-19 pandemic, 16% at the peak of the COVID-19 contagion, and 12.7% at the time of the survey (Fig. 1).
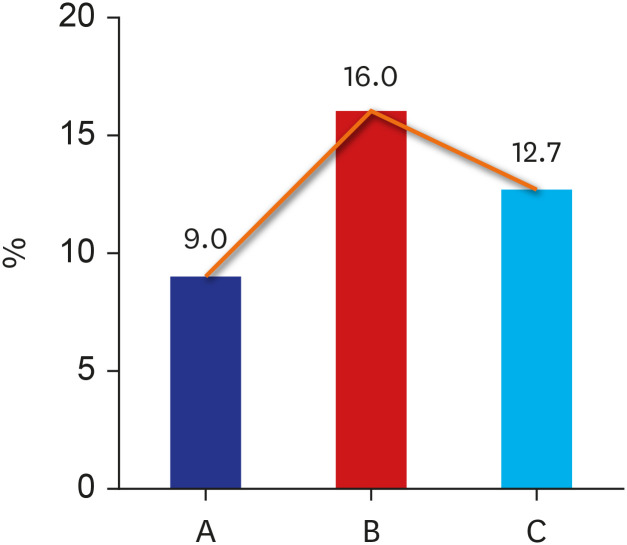 | Fig. 1Unbearable stress experiences of students at the three time-points. (A) Before the COVID-19 pandemic, (B) At the peak time of the COVID-19 contagion, (C) At the time of the survey. Unbearable stress was experienced by 9.0% of students before the COVID-19 pandemic, 16.0% of students at the peak time of the COVID-19 contagion, and 12.7% of students at the time of the survey (2–3 months after the peak of the COVID-19 contagion).COVID-19 = coronavirus disease 2019.
|
Of the students who experienced unbearable stress at the peak of the COVID-19 contagion, girls experienced more stress than boys (18.1% versus 13.8%; χ2 = 28.159, P < 0.001), while high school students experienced more stress than middle school students (19.0% versus 13.5%; χ2 = 45.437, P < 0.001). Unbearable stress was also reported more by students who experienced a confirmed diagnosis of COVID-19 compared to those who did not (21.4% versus 15.7%; χ2 = 7.997, P < 0.001).
Students who experienced unbearable stress were asked about the main reasons why they were stressed at each time point. Before the COVID-19 pandemic, the most common reasons were pressure to study (77.9%), followed by school achievement (62.6%) and friendship (47.9%). At the peak of the COVID-19 contagion, the most common reasons were having a non-routine experience (57.1%), followed by fear of infection (45.8%) and pressure to study (43.6%). At the time of the survey, these reasons were pressure to study (62.3%), school achievement (51.9%), and having a non-routine experience (32.2%) (Fig. 2).
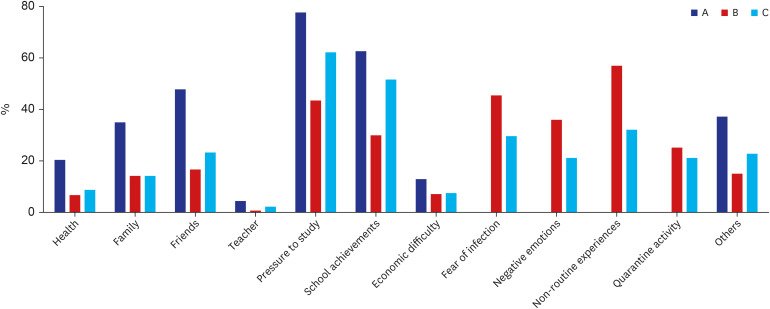 | Fig. 2Factors causing unbearable stress at the three time-points. (A) Before the COVID-19 pandemic, (B) At the peak time of the COVID-19 contagion, (C) At the time of the survey.Students who experienced unbearable stress were asked about the main reasons for being stressed at each time point. Before the COVID-19 pandemic, the most common reasons were pressure to study (77.9%), followed by school achievement (62.6%) and friendship (47.9%). At the peak of the COVID-19 contagion, the most common reasons were having a non-routine experience (57.1%), followed by fear of infection (45.8%) and pressure to study (43.6%). At the time of the survey, these reasons were pressure to study (62.3%), school achievement (51.9%), and having a non-routine experience (32.2%).
COVID-19 = coronavirus disease 2019.
|
Emotional crisis
There were 625 students (7.6% of the total) who experienced an emotional crisis. Compared to the total number of students, twice as many girls experienced emotional crises compared to boys (10.1% versus 5.2%; χ2 = 71.025, P < 0.001). More high school students also experienced emotional crises compared to middle school students (8.8% versus 6.7%; χ2 = 12.996, P < 0.001). Emotional crises were more frequently reported by students who experienced a confirmed diagnosis of COVID-19 compared to those who did not (13.4% versus 7.4%).
Among the students who experienced an emotional crisis, the following causes were identified: academic and career concerns (67.7%), mental health (38.8%), and family conflicts (35.4%) (Table 2).
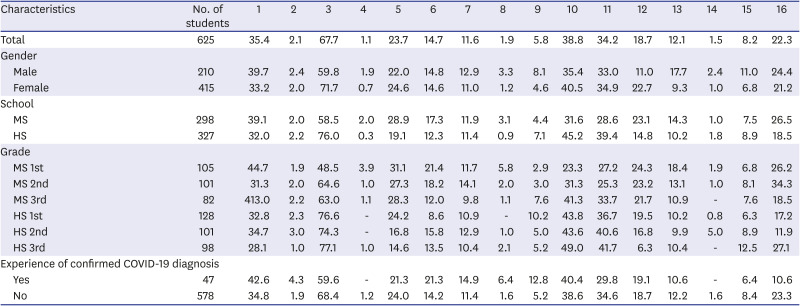
Table 2
Percentage of factors that caused emotional crisis after COVID-19 by major variables
Factors causing emotional crisis (1–16) are presented as a percentage.
All participants that responded they had experienced emotional crisis chose 3 of 16 factors caused emotional crisis.
1, Family conflict; 2, Delinquent and deviant behavior; 3, Academic / Career concerns; 4, Sexual problem; 5, Personality conflict; 6, Conflict with peers; 7, Social withdrawal; 8, Conflict with teachers; 9, Dating relationship; 10, Mental health; 11, Lifestyle change; 12, Unsatisfied appearance; 13, Internet conflict; 14, Paucity of information; 15, Lack of outdoor activity; 16, Others.
MS = middle school, HS = high school, COVID-19 = coronavirus disease 2019.
![]()
The common coping mechanisms for these students were singing or listening to music (50.9%), seeking solutions alone (46.7%), and sleeping (43.1%).
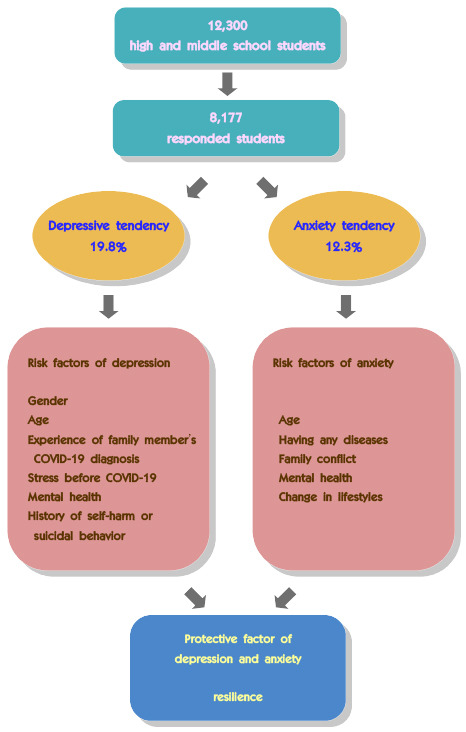
Depression
The PHQ-9 scores showed that 19.8% of all students had depressive tendencies (mild or more severe). Among them, depressive tendencies were more commonly seen in girls than boys (24.5% versus 14.9%; χ2 = 127.660, P < 0.001), in high school students than middle school students (22.4% versus 17.5%; χ2 = 30.499, P < 0.001), and in students who experienced confirmed COVID-19 diagnosis than those who did not (25.6% versus 19.5%; χ2 = 11.742, P < 0.001) (Tables 3 and 4).
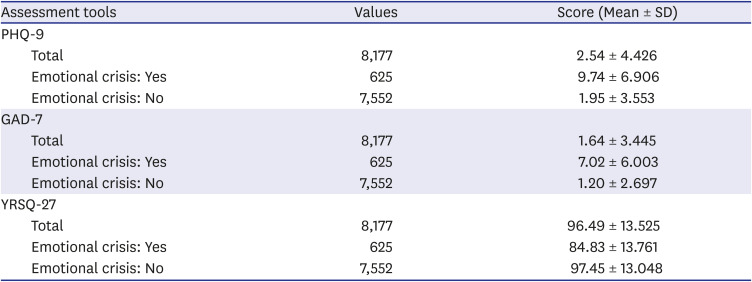
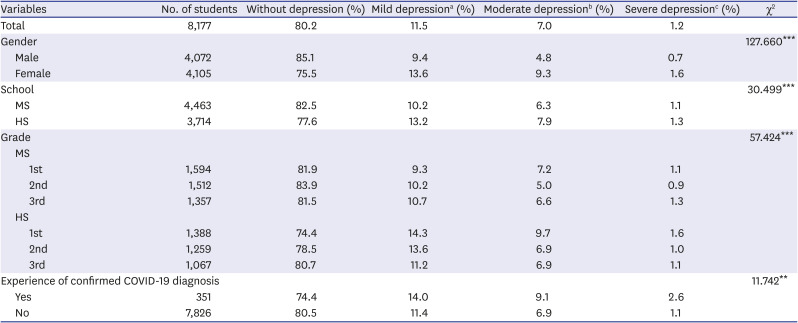
Table 3
Psychological data of the participants
Values are presented as number (%) and scores were presented as mean ± SD.
SD = standard deviation, PHQ-9 = nine-item Patient Health Questionnaire, GAD-7 = seven-item Generalized Anxiety Disorder, YRSQ = 27-item Youth Resilience Scale.
![]()
Table 4
The distribution of depression levels by major variables
MS = middle school, HS = high school, COVID-19 = coronavirus disease 2019, PHQ-9 = nine-item Patient Health Questionnaire.
aMild depression: 5–9 points in the nine-item PHQ-9, bModerate depression: 10–19 points in the PHQ-9, cSevere depression: 20–27 points in the PHQ-9.
**P < 0.01, ***P < 0.001.
![]()
Anxiety
The GAD-7 scores revealed that 12.3% of all students had mild or more severe. Among them, anxiety was seen more commonly in girls than boys (14.9% versus 9.7%; χ2 = 56.991, P < 0.001), in high school students than middle school students (14.6% versus 10.4%; χ2 = 37.796, P < 0.001), and in students who experienced confirmed COVID-19 diagnosis than those who did not (17.1% versus 12.1%; χ2 = 8.570, P < 0.05) (Tables 3 and 5).
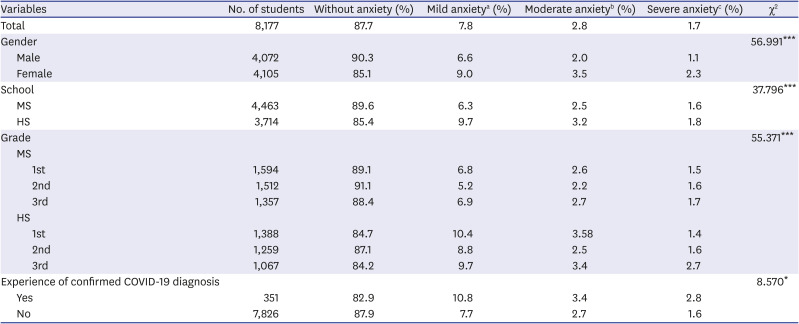
Table 5
The distribution of anxiety levels by major variables
MS = middle school, HS = high school, COVID-19 = coronavirus disease 2019, GAD-7 = seven-item Generalized Anxiety Disorder.
aMild anxiety: 5–9 points in the seven-item GAD-7, bModerate anxiety: 10–14 points in the GAD-7, cSevere anxiety: 15–21 points in the GAD-7.
*P < 0.05, ***P < 0.001.
![]()
Factors influencing depression and anxiety in students who experienced emotional crises after the COVID-19 pandemic
In this study, we conducted a logistic regression test on 625 students who experienced emotional crises during the COVID-19 pandemic to determine the factors affecting their depression (PHQ-9 score) and anxiety (GAD-7 score). The following factors affecting depression were identified: female gender, younger age, the experiences of a family member's COVID-19 confirmed diagnosis, mental health, experiences of unbearable stress before the COVID-19 pandemic, history of self-injury or suicide. The following factors predicting anxiety were identified: younger age, current physical diseases, experiences of unbearable stress before the COVID-19 pandemic, poor mental health, changes of lifestyle, conflicts in families. Both depression and anxiety had the highest odds ratio for experiences of unbearable stress before the COVID-19 pandemic. Meanwhile, resilience against stress was a protective factor for depression and anxiety (Table 6).
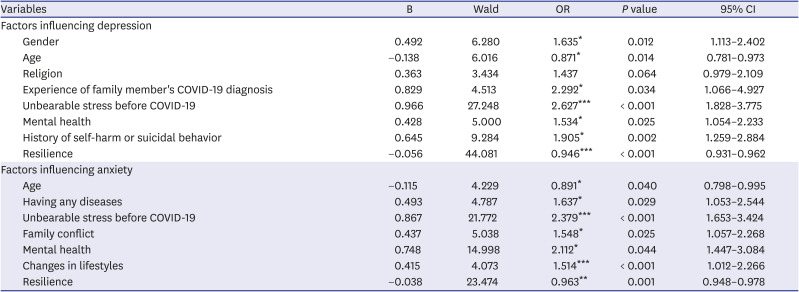
Table 6
Factors influencing depression and anxiety in students who experienced emotional crises after the COVID-19 pandemic
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
Go to :
DISCUSSION
Many people worldwide are experiencing various changes and difficulties in a short period of time during the COVID-19 pandemic. Bell et al.34 insisted that it is important to understand the COVID-19 pandemic from a disaster perspective as well as its psychological implications. Indeed, a number of papers have reported that aside from the number of COVID-19 cases during the pandemic, a variety of people have also suffered psychological difficulties such as fear, depression, anxiety, and sleep disorders.3536373839 Since the COVID-19 pandemic, there have been many changes in all parts of society around the world; some have had emotional impacts on students’ lives, including school closure, online learning, reduced physical activity, reduced contact with friends, and changes in sleep patterns.131840 Because of these reasons, we analyzed the data released by the Daegu Metropolitan Office of Education to determine the emotional impacts and the involved factors on middle and high school students in Daegu city, who experienced a massive spread of COVID-19 in South Korea before its declaration as a worldwide pandemic.
We investigated the unbearable stress that students experienced across three time periods: “before the COVID-19 pandemic,” “at the peak time of COVID-19 contagion,” and “present” (at the time of the survey). The number of students who experienced unbearable stress almost doubled at the peak time of the COVID-19 contagion compared to before the COVID-19 pandemic. Over time, although it is higher than before the COVID-19 pandemic, unbearable stress somewhat decreased at the time of the survey compared to the peak time of the COVID-19 contagion. In a study of 385 children and adolescents, Cost et al.22 reported that subjects suffered stress during the COVID-19 pandemic, which increased various psychiatric symptoms. Rothe et al.41 reported that changes such as social isolation and threats to physical health caused stresses in children and adolescents; even children and adolescents who were mentally healthy before COVID-19 deteriorated in mental happiness. Our study had similar findings. The rate of female students who experienced unbearable stress in this study was higher than that of male students. In line with the results of previous studies, we also found that females were more vulnerable to many psychiatric disorders and stress than males.4243 Moreover, high school students had a higher rate of stress experiences than middle school students in this study. Esposito et al.44 reported more sadness in subjects aged 13–19 years versus those aged 11–13 years, while Zhou et al.45 reported increased depression and anxiety in a study of adolescents aged 12–18, specifically in students in higher grade levels; these were similar to our results. When analyzing the causes behind stress, students identified these to be pressure to study and school grade/achievement as the highest cause of unbearable stress before the COVID-19 pandemic, followed by stress about their friends and peer relationships. However, at the peak time of the COVID-19 contagion, the top two causes were having a non-routine experience and fear of infection, respectively, followed by pressure to study. Thus, it can be expected that high school students, who experience higher stress from studying, are more stressed than middle school students. Having a non-routine experience was the most common reason for unbearable stress at the peak time of the COVID-19 contagion. Two to three months after, the frequency of this answer decreased; during which pressure to study and school achievements became the common causes of unbearable stress, at a similar rate to that before the COVID-19 pandemic. This is in line with a meta-analysis that found that after the peak of the COVID-19 pandemic, many people were resilient to stress and mental illness.46
During the COVID-19 contagion, 7.6% of students in this study experienced an emotional crisis, with a particularly higher rate in girls, high school students, and students with an experience of confirmed COVID-19 diagnosis. This pattern was similar to that of the experience of unbearable stress. Academic and career path concerns were most commonly cited as the cause of the emotional crisis, followed by mental health and family conflicts. Previous studies have reported stressors such as school closure and class-related problems as stress factors for students; prolonged lockdown, domestic violence, and internet abuse were also identified to affect mental health.184447
After the spread of COVID-19, the psychological scale identified depression and anxiety (mild or more severe) among 19.8% and 12.3% of all students, respectively, with higher rates in females, high school students, and students with an experience of COVID-19 confirmed diagnosis. This pattern was similar to that seen in unbearable stress and emotional crisis. Zhou et al.45 found depression and anxiety, respectively, in 43.7% and 37.4% of Chinese adolescents during the COVID-19 pandemic. Likewise, Chi et al.48 found depression and anxiety, respectively, in 48.2% and 36.7% of 1,794 Chinese adolescents. Our study showed lower rates of depression and anxiety than these studies but similarly showed higher rates of depression and anxiety in females and students in higher grade levels overall.
Lastly, we investigated the factors that affected depression and anxiety among students who experienced emotional crises during the COVID-19 pandemic. Zhou et al.45 reported that the female gender was the highest risk factor for depression and anxiety symptoms during the COVID-19 pandemic in adolescents. Zhou et al.49 also reported that the female gender was a risk factor of sleep disturbance after the COVID-19 pandemic in their study of subjects aged 10s and 20s. In this study, the female gender was related to depression but did not affect anxiety. Von Soest et al.50 mentioned that concerns about diseases and infections related to COVID-19 were associated with lower life satisfaction. Likewise, individuals with any disease were more anxious in this study. In addition, Lee et al.51 reported that information about COVID-19 from the media was a protective factor for fears of infection, prejudice of infected persons, and anxiety, but in this study, knowledge about COVID-19 did not affect depression and anxiety.
We identified family conflict as one of the factors affecting anxiety. Similarly, some studies identified positive communication among family members as a protective factor for emotional difficulty and violence, while conflict among family members was a risk factor.4452 Our study found that depression and anxiety were increased in students with unbearable stress before the COVID-19 pandemic, emotional crises related to mental health, and a history of suicide and self-harming behavior. A study in adults reported that some factors such as past history of depression, suicide, and self-harming behavior, as well as poor current health, were risk factors for the development of depression, which was similar to our findings.53 In addition, we found that resilience was a protective factor associated with reducing depression and anxiety. Likewise, Zhang et al.54 reported that resilience was a protective factor for depression, anxiety, and stress in a study of middle and high school students; a study of children and adolescents by Zhang et al.55 also found that physical activities can have a positive effect on mood states.
This study has some limitations. First, this is a cross-sectional study, not a longitudinal follow-up study, that required students to assess their past and present experiences during a single point in time. However, it is likely that there were not many memory errors because the past experiences did not happen too long ago, and the survey was also specifically designed to question their experiences before and after an important event the subjects were able to experience firsthand. Second, since the survey in this study was an online self-reported survey, the respondents' attitudes may have affected the reliability of the survey. To ensure the quality of data, we did not analyze data from respondents who completed the survey below the expected minimum survey time of 10 minutes, those who answered only the same score throughout the survey, and those who had incomplete answers.
In summary, we identified the mental health of middle and high school students in Daegu metropolitan city who experienced a rapid increase in the number of COVID-19 infections at a time when the COVID-19 pandemic began to spread. Many students experienced stress and emotional crises during the peak of the COVID-19 contagion, which caused depression and anxiety. However, we were able to confirm that stress in many adolescents reduced over time due to resilience. Factors predicting depression and anxiety among students who experienced emotional difficulties due to the COVID-19 pandemic included previous stressors and mental health, while resilience was identified as a protective factor. Our findings suggest that paying attention to students’ stress and mental health and increasing their resilience at ordinary times are ways to prevent negative emotions during life-threatening or life-changing events such as the COVID-19 pandemic.
Go to :
 XML Download
XML Download