

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Macrosomia or high birth weight infant refers to a newborn with a birth weight ≥ 4 kg, regardless of gestational age. The incidence of macrosomia is approximately 3–7%, and about 1% of babies weigh ≥ 4.5 kg.1 According to birth registration data from Statistics Korea, the incidence of macrosomia was 2.8% in 2019, which shows a decreasing trend compared to previous years, such as 3.6% in 2010.23 Around the same time, the prevalence of macrosomia in developed countries was about 5–20%, which is increasing, and the situation in developing countries is also increasing, primarily due to the increasing obesity and diabetic disorders of reproductive-aged women.4
The major risk factors for macrosomia are diabetic disease, maternal obesity, and family history of macrosomia. The prevalence of macrosomia is 13.3% among mothers with gestational diabetes mellitus (GDM) and 3.6% among non-GDM mothers. Around 6–10% of pregnant women are obese, and 19% of obese mothers are diabetic.2 In addition, hypertension, multiparity, excessive maternal weight gain during pregnancy, advanced maternal age, and male fetus are often regarded as risk factors for macrosomia.56
Macrosomia is associated with several maternal, perinatal, and neonatal complications, such as emergency cesarean section and injury to the birth canal and baby.2456 Congenital anomalies are more common, and cardiac defects occur in the majority. Macrosomias are more prone to growth and developmental retardation, hypoglycemia, hypocalcemia, polycythemia, and hyperbilirubinemia. Research regarding the complications of low birth weight infants is varied, and great advancement in understanding and outcome has been achieved. However, there are fewer studies regarding macrosomia, especially on the national incidences and outcomes in Korea.2 Only several single-center observational studies and one national epidemiologic analysis in 1996 are available.
The aim of this study was to estimate the incidence of macrosomia in Korea and to identify the growth and developmental outcomes and other neonatal complications that occur with macrosomia.
Go to : 
METHODS
Patients and data source
We initially identified 397,203 infants who were born in 2013 with birth weight ≥ 2.5 kg and examined infant health check-ups between the 1st and the 7th visit from the National Health Insurance Service (NHIS) database. Healthcare claims of almost all Korean residents, including diagnostic codes and costs of diagnostic tests and procedures, were linked to the health check-up database. The information, including birth weight and morbidities was also obtained from the International Classification of Diseases (ICD)-10 codes78 that were inputted by the hospital, or by a self-reported questionnaire in the National Health Screening Program. The infants were divided by the birth weight as 3 groups as 2.5–3.99 kg, 4.0–4.49 kg, and ≥ 4.5 kg group. The reference group was defined the infants with 2.5–3.99 kg birth weight. We used birth statistics to estimate the examination rate of the National Health Screening Program.2
The National Health Screening Program for infants and children in Korea was launched in 2007 to monitor current health issues. The program includes medical history, physical examination, anthropometric measurements, screening for visual acuity, developmental screening by the Korean Developmental Screening Test (K-DST), oral examination, and questionnaires with anticipatory guidance. The time period for the National Health Screening Program (1st to 7th) was 6 months for those aged 4–6 months, 12 months for those aged 9–12 months, 24 months for those aged 18–24 months of age, 36 months for those aged 30–36 months, 48 months for those aged 42–48 months, 60 months for those aged 54–60 months, and 72 months for those aged 66–72 months. Growth was assessed using the Korean standard growth curve. The K-DST is a screening test which verifies whether infants have normal neurodevelopmental status in the domains of gross motor, fine motor, cognition, communication, social interaction, and self-control. The participants take the test papers according to their corrected age at the time of their clinic visit and get the result as 4 categorized groups: the further evaluation, the follow-up test, the peer-level, and the high-level groups. Children who score < −1 standard deviation (SD) are categorized as the follow-up test group and they need short-term checkups for re-evaluation. Any patients with clinically important diseases, such as cerebral palsy, language delay, and autism spectrum disorders, should be referred for further evaluation.9 Poor developmental result was included as the further evaluation and the follow-up test. Growth was categorized as < 90th percentile, 90–95th percentile, and ≥ 95th percentile of weight, height, and head circumference.
Statistical analyses
The cohort was stratified according to the birth weight or age at checkup. The characteristics of the subjects were expressed as means and standard deviations for continuous variables and as percentages for categorical variables. Growth parameters were analyzed by age or according to birth weight using one-way ANOVA or chi-square test. Multiple logistic regression was used to determine the independently associated factors with macrosomia among infants with odds ratios (ORs) and 95% confidence intervals (CIs). Multivariate longitudinal data analysis was done using multivariate repeated measured model (PROC MIXED and GENMOD). All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, North Carolina). P values < 0.05 were considered statistically significant.
Ethics statement
This study used NHIS research cohort data and Infants and Children's Health Screening (2013–2018) data (NHIS-2021-1-220). All identifiable data, including claim-, individual-, and organizational-level identification numbers, were randomly regenerated by the NHIS database to protect patient privacy. The study protocol was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (IRB No. 3-2020-0502). The need for informed consent was waived.
Go to :
RESULTS
Growth outcome
The number of infants who underwent the health checkup ranged from 263,151 (66%) to 321,158 (81%). The highest number of infants (n = 321,158, 81%) was included in the health checkup at 24 months of age. The distribution of number of infants who took the infant health checkup according to birth weight group is shown in Table 1.
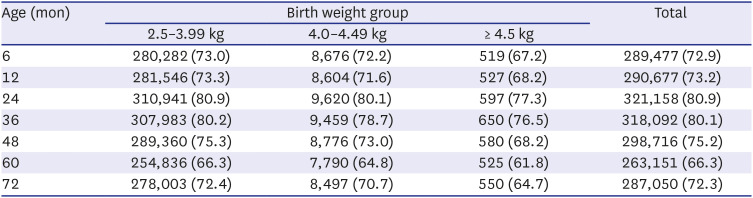
Table 1
Number of infants participating in the National Health Screening Program
![]()
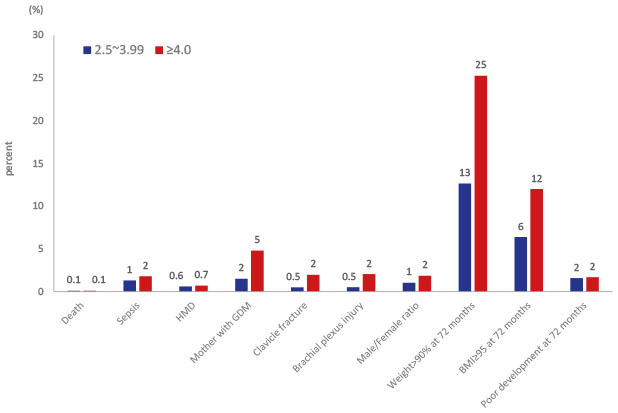
Macrosomia showed significantly higher incidence of sepsis, male sex, and mothers with GDM. In addition, higher incidence of clavicle fracture, Erb's palsy, and brachial plexus injury among macrosomia compared to the reference group was noted (Table 2).
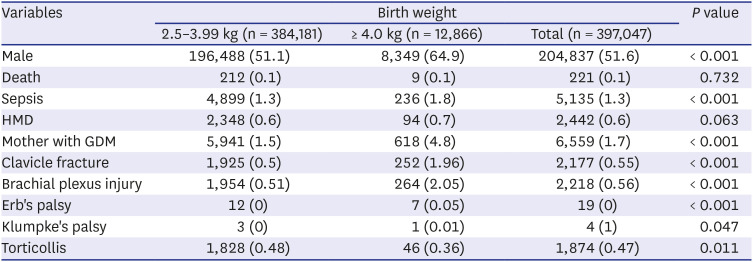
Table 2
Comparisons of demographic characteristics between the infants with 2.5–3.99 kg and above 4.0 kg
Data are presented as number (%).
HMD = hyaline membrane disease, GDM = gestational diabetes mellitus.
![]()
The mean percentiles of height, weight, and head circumference for age at health checkup are shown in Fig. 1. On longitudinal analysis, there was a significant difference in weight, height, and head circumference according to the age, birth weight, and combination of age and birth weight, respectively (P < 0.001). Those with higher birth weight showed higher mean percentiles of weight, height, and head circumference. There was a significant difference in height, weight, and head circumference between the macrosomia group (4.0–4.49 kg, ≥ 4.5 kg) and the reference group according to age at health checkup (P < 0.001 respectively).
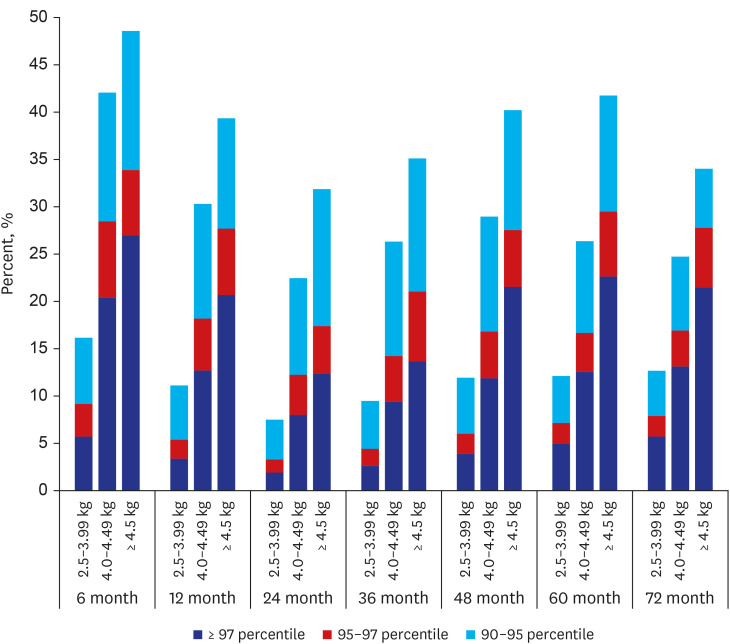
The distribution of the infants with weight ≥ 90th percentile is shown in Fig. 2. The number of infants with weight ≥ 90th percentile showed a significant difference between the macrosomia (4.0–4.49 kg, ≥ 4.5 kg) and the reference group according to age at health checkup (P < 0.001 respectively).
The distribution of body mass index (BMI) percentile at 60 month of age and 72 month of age was shown in Table 3. The mean BMI percentile (SD) showed a significant difference among the birth weight groups (P < 0.001); it was 50.6 (29.3) in infants with 2.5–3.99 kg birth weight, 63.5 (27.4) in those with 4.0–4.49 kg birth weight, 71.0 (25.6) in those with 4.5–4.99 kg birth weight, and 73.1 (29.2) in those with ≥ 5.0 kg birth weight.

Table 3
The distribution of body mass index percentile at 60 months of age and 72 months of age
![]()
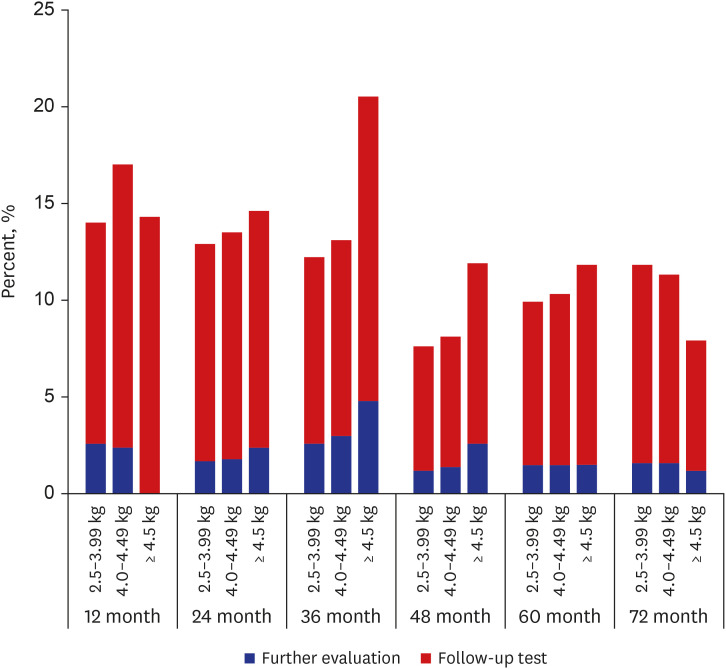
The incidence of poor developmental result at 72 months of age was 10% (29,020), with further evaluation revealing 4,572 (1.5%) infants, and the follow-up test revealing 24,448 (8.5%) infants. There was significant difference in the incidence of poor developmental result between infants with macrosomia and the reference group in 24, 36 and 48 month of evaluation, showing increased odds of poor developmental result in macrosomia compared to reference group at 24 (OR, 1.07; 95% CI, 1.01–1.13), 36 (OR, 1.13; 95% CI, 1.07–1.19) and 48 (OR, 1.12; 95% CI, 1.05–1.2) month of evaluation, respectively (Fig. 3).
Among macrosomia (n = 12,866), the comparison of outcomes between mother with GDM (n = 618) and without GDM (n = 12,248) was done. Mother with GDM showed significant higher incidence of sepsis (7.6% vs. 3.1%, P < 0.001), HMD (5.3% vs. 1.3%, P < 0.001), and clavicle fracture (4.1% vs. 2.1%, P < 0.001). Mean weight percentile (SD) at 60 and 72 months of age showed significant higher in mother with GDM than mother without GDM (70.4 [25.8] vs. 67.6 [25.8], P = 0.020, 72.4 [26.1] vs. 68.5 [26.1], P = 0.003). In addition, the incidence of infants with BMI percentile above 90th at 60 and 72 months of age showed significant higher in mother with GDM than mother without GDM (18.6% vs. 21.8%, P = 0.003, 18.9% vs. 24.8% P < 0.001). There is no significant difference of poor developmental result between mother with and without GDM.
Go to :
DISCUSSION
Macrosomia can be an important risk factor for maternal, perinatal, and neonatal complications. To the best of our knowledge, this is the most recent, nationwide epidemiologic study to consider the incidence and growth and developmental outcomes of macrosomia. This study showed macrosomia remains an issue due to persisting high BMI and poor developmental outcomes, which may lead to complications in adulthood. This study may be a great answer to the big, current health issue concerning childhood or adult metabolic syndrome, and may formulate treatment and prevention strategies. If we focus on this somewhat overlooked high-risk group, we may be able to improve their health and reduce enormous socioeconomic burden.
According to statistics from the Korean National Statistical Office, the frequency of macrosomia decreased annually from 6.7% to 2.8% between 1993 and 2019. This is thought to have been due to the improvement of prenatal maternal care, particularly the improvement of gestational diabetes treatment, which is the most important cause of macrosomia. In the past, about 60% of babies born to diabetic mothers were above the 95th percentile of the same age group in body weight, but this has recently decreased to 20–30%, due to improvements in gestational diabetes treatment.10 Cho et al.11 noted that GDM mothers are significantly more likely to deliver an infant with macrosomia. The frequency of macrosomia was 13.3% in the case of gestational diabetes but only 3.6% in mothers without gestational diabetes.11 In this study, 4.8% of macrosomia had a mother with gestational diabetes, showing that GDM as a significant risk factor for macrosomia.
A study revealed that fetal macrosomia had an incidence of 9.1%.12 A retrospective cohort study conducted at a large maternity unit in the UK between January 2009 and December 2016 showed the incidence of fetal macrosomia as 12.0%.13 Maternal BMI and diabetes are strong risk factors for macrosomia, irrespective of region, in 23 developing countries in Africa, Asia, and Latin America.8 Because infants with macrosomia show complications, a national study in the United Sates categorized macrosomia as > 4 kg, > 4.5 kg, and > 5 kg to better predict its risks.14 For our study, we stratified macrosomia in the same manner.
Postnatal catch-down growth in large for gestational age (LGA) or macrosomia may be protective against obesity and being overweight. LGA children without catch-down growth had an increased risk of overweight at 4 years of age.15 In a longitudinal growth study of 2,465 Chinese children, catch-down growth in weight, length, and ponderal index of high birth weight term infants was not achieved within 12 months of age.16 Peters et al.17 showed in their study with LGA-children of mothers without GDM that 88% showed catch-down growth within 12 months of age. Despite the catch-down growth, the differences in the mean weight, length, and HC remained until 4 years of age, and those without catch-down growth had more subcutaneous fat. Irrespective of feeding pattern, the majority showed catch-down growth. However, the catch-down could not achieve complete normalization.17 This is in line with our results, in which complete catch-down growth did not occur. Those with macrosomia remained within their growth percentile until 72 months of age. Considering these, prenatal treatment, such as GDM control and maternal weight control, is the most important factor in growth outcomes.
In meta-analysis, high birth weight or macrosomia is an independent risk factor for later overweight and obesity.18 Obese children are more likely (up to 80%) to become obese adults.19 This is consistent with our study results that BMI is consistently higher until 72 months of age in the macrosomia group. By considering that birth weight is essentially determined by in-utero condition, preventing in-utero over-nutrition by avoiding maternal overweight and/or controlling gestational diabetes will help to avoid overweight in the newborn and during childhood.
Several studies show that male gender is an independent risk factor for childhood overweight and obesity.2021 In our study, male sex was an independent risk factor for macrosomia, and macrosomia was associated with an increased incidence of sepsis. Among infants with macrosomia, hyaline membrane disease is more common, possibly due to maternal diabetes.22 Macrosomia was associated with increased mortality (OR, 2.2), and maternal diabetes and high birth weight showed synergy in mortality.2324 In our study, there was no significant difference in HMD and mortality. In a comparative study between large infants of non-diabetic mothers and a control group of infants with 3–3.99 kg birth weight, clavicular fracture, Erb's palsy, and humerus fracture were significantly more frequent in the large infant group.16 In our study, there were higher incidence of clavicular fracture, Erb's palsy, or brachial plexus palsy in the macrosomia group (2.1%) compared to in control group (0.5%).
There is a meta-analysis that statistically significant cognitive impairment in infants of diabetic mothers during the first year may result in a delay in mental performance afterwards.25 In an experimental rat study, maternal obesity associated GDM resulted in neuroinflammation by microglial activation in the newborn offspring, and the influence sustained to young adulthood by astrogliosis and derangement of the hippocampal layer.26 Generally, our study is consistent with previous studies showing the risks and poor outcomes of macrosomia. Infants with macrosomia are prone to neonatal disease, neurodevelopmental delay, and childhood overweight and obesity, particularly in boys.
Our study has several potential limitations. First, we could not be analyzed to determine a cause-effect relationship as an epidemiologic study. Second, a lack of familial background data, such as maternal and paternal height and BMI, and environmental factors like socioeconomic status and feeding pattern were not considered in this study due to the lack of data. Further studies need to incorporate these factors. Third, since the infants were included in only about 96.4% of the birth statistics, and the number of infants participated in the program was varied, and the weight was based on the questionnaire of the national health screening program for infants and children, the missing data or selection issue may potentially influence our findings. Last, diagnosis of several morbidities was identified according to ICD-10 codes of the NHIS claims database without reviewing the detailed clinical charts. The misclassification or omission have potentially affected our findings
In conclusion, macrosomia can be a risk factor for neonatal and childhood complications including obesity and developmental delay. Careful monitoring and proper strategies for prenatal care, and postnatal feeding and physical activity for catch-down growth may be helpful to prevent later adverse results.
Go to :
 XML Download
XML Download