

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Based on general consensus, treatment of abdominal aortic aneurysm (AAA) is recommended when the maximal orthogonal aneurysm diameter reaches 5.5 cm or larger in patients with acceptable operative risk because untreated AAA can potentially rupture.1 Furthermore, two-thirds of ruptured AAA occurs in patients ≥ 75 years of age and their 30-day mortality rate is 69%.2 In addition, survival rates of ruptured AAA in octogenarians was reportedly 23%, which was much lower than in non-octogenarians.3 However, controversies remain whether open AAA repair can be an acceptable treatment for elderly patients considering their high operative risks. Despite advances in medical technology, old age is a well-known independent risk factor for morbidity and mortality after open AAA repair.45 In other studies, 30-day mortality in octogenarians after elective open AAA repair was reportedly 1.1–8.5% and 1-year mortality was 11.9–17%.46789
Despite old age being one of the major obstacles with other medical comorbidities, the incidence of AAA increases as life expectancy increases, which can complicate treatment selection. The likelihood of incidental detection of AAA before it ruptures also increases as health check-up and accessibility to medical imaging increases.10 Lastly, because Korea is becoming an aging society, the frequency of AAA in elderly patients is expected to increase.
Although the first choice of treatment for AAA is endovascular aneurysm repair (EVAR), especially in elderly patients, some patients require open surgical repair.11 Questions regarding the durability of EVAR might increase the demand for open conversion surgery. Therefore, the need for open AAA repair is expected to increase.
In the present study, whether octogenarians are appropriate candidates for open AAA repair was determined by comparing outcomes between octogenarians and their younger counterparts, and the risk factors associated with postoperative mortality were identified.
Go to : 
METHODS
To select patients, the vascular surgery database in our institution, which is collected and managed prospectively, was reviewed and 963 patients were identified who underwent open AAA repair from 1996–2020. Among the patients, those with etiologies other than degenerative AAA, including ruptured AAA (n = 148), infected AAA (n = 48), open conversion after EVAR (n = 54), AAA in connective tissue disease or vasculitis (n = 38), dissecting aneurysm (n = 16), AAA combined with thoracic aortic aneurysm (n = 5), trauma related AAA (n = 1), and etiology unknown (n = 3), were excluded. For the comparative analyses, selected patients were divided into two groups, patients ≥ 80 years of age (octogenarians) and patients < 80 years of age (non-octogenarians). Finally, 650 patients were included for the analysis, 58 (8.9%) octogenarians and 592 (91.1%) non-octogenarians.
The following clinical information was collected from medical chart review: demographic information (age, sex), body mass index (BMI) at admission, medical comorbidities, American Society of Anesthesiologists (ASA) score, preoperative blood test values, preoperative symptom status, and surgical details including renal ischemic time, concomitant adjuvant procedures, and other intraoperative factors that potentially influence outcome, such as total amount of transfusion and blood loss, total operation time, and use of vasopressors. Maximal orthogonal aneurysm diameter and aneurysm location were collected through review of preoperative computed tomographic angiography images performed within 6 months before operation. In our center, surgical treatment is recommended in cases of indication of repair, except for patients with absolutely limited life expectancy. Generally, EVAR is implemented as a first method; in cases of instruction for use (IFU) violation, open AAA repair is considered.
Postoperative outcomes were compared between octogenarians and non-octogenarians in terms of postoperative medical complications (acute myocardial infarction, stroke, pneumonia, acute respiratory distress syndrome, acute kidney injury, pulmonary thromboembolism, ischemic colitis, spinal cord ischemic, ileus, and delirium) and surgical complications (bleeding requiring re-operation, graft infection or thrombosis, and wound complications). Total length of hospital and ICU stay, as well as 30-day and 1-year mortality, were compared between the two groups. Death was verified using the Korean Death and Causes of Death Statistics database that is linked to electronic medical records.
Statistical analysis
Comparison between the two groups was performed using χ2 test, Fisher's exact test, and Student's t-test. Continuous variables were expressed as median (interquartile range [IQR]) and categorical variables were expressed as proportion (%). Survival analysis was performed using Kaplan-Meier survival analysis, and differences in survival were analyzed using the log-rank test. To identify the risk factors associated with mortality, multiple logistic regression analyses were used to calculate the odds ratios (ORs). The variables with statistical significance in univariable analysis were entered into the multivariable analysis. All statistical analyses were performed using IBM SPSS Statistics Software Version 27.0 (IBM, Armonk, NY, USA), and P <0.050 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Samsung Medical Center in Seoul, Korea (IRB No. 2021-06-172). The need for informed consent was waived due to the retrospective nature of the study.
Go to :
RESULTS
The baseline characteristics are shown in Table 1. The median age was 82 years (IQR, 81–84) for octogenarians and 69 years (IQR, 63–74) for non-octogenarians. Male sex was less prevalent in octogenarians than in non-octogenarians (70.7% vs. 87.3%, P = 0.001). The mean body weight (59.5 ± 11.4 vs. 67.1 ± 10.4 kg, P < 0.001) and BMI (22.9 ± 3 vs. 24.4 ± 3.3 kg/m2, P = 0.001) at admission were lower in octogenarians compared with non-octogenarians. Comorbidities of octogenarians showed a higher proportion of hypertension (86.2% vs. 69.9%, P = 0.009) and chronic kidney disease (CKD, Cr ≥ 2) compared with non-octogenarians (13.8% vs. 4.4%, P = 0.007). Preoperative blood tests of octogenarians showed lower mean hemoglobin (11.2 ± 1.4 vs. 12.6 ± 1.9 g/dL, P < 0.001) and median albumin levels (3.6 vs. 3.9 g/dL, P = 0.001) compared with non-octogenarians. Proportion of ASA score ≥ 3 was higher in octogenarians than in non-octogenarians (84.5% vs. 53.2, P < 0.001).
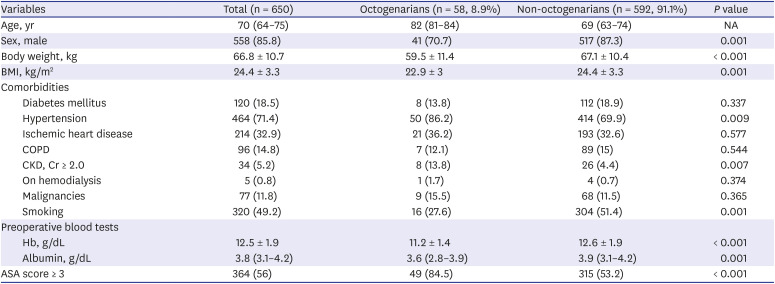
Table 1
Demographic and baseline comorbid information of octogenarians and non-octogenarians who underwent elective open abdominal aortic aneurysm repair between 1996 and 2020
Data are shown as median (interquartile range), mean ± standard deviation, or number (%).
BMI = body mass index, NA = not applicable, COPD = chronic obstructive pulmonary disease, CKD = chronic kidney disease, Cr = creatinine, Hb = hemoglobin, ASA = American Society of Anesthesiologists.
![]()
Symptom status as well as anatomic and surgical details are listed in Table 2. Symptom status, aneurysm location, or surgical details were not different between the two groups. However, the maximal median aneurysm diameter was greater in octogenarians than in non-octogenarians (60 mm vs. 54.3 mm, P < 0.001), and intraoperative transfusion amount of red blood cells (RBC) was greater in octogenarians than in non-octogenarians (1 vs. 2 units, P < 0.001). The use of vasopressors was more frequent in octogenarians than in non-octogenarians (79.3% vs. 67.1%, P = 0.056).
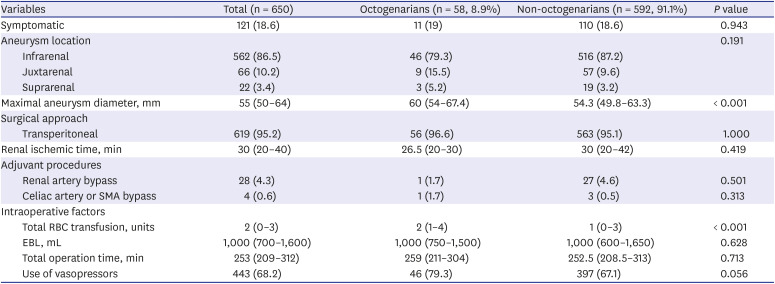
Table 2
Symptom status, anatomic and surgical details of octogenarians and non-octogenarians who underwent elective open abdominal aortic aneurysm repair
Values are presented as median (interquartile range) or number (%).
SMA = superior mesenteric artery, RBC = red blood cells, EBL = expected blood loss.
![]()
Postoperative outcomes are shown in Table 3. The median follow-up duration was shorter in octogenarians than in non-octogenarians (19.8, IQR, 3.9–41.8 vs. 37.9, IQR, 9.1–89 months, P < 0.001). During the follow-up periods, pneumonia (5.2% vs. 1.2%, P = 0.052), delirium (15.5% vs. 3.4%, P < 0.001), and wound complications (8.6% vs. 0.8%, P = 0.001) were more prevalent in octogenarians than in non-octogenarians. Other medical and surgical complications did not differ between the two groups. Total length of hospital (13, IQR, 10–15 vs. 11, IQR, 10–14 days, P = 0.031) and ICU stays (1, IQR, 1–3 vs. 1, IQR, 1–2 days, P = 0.003) were longer in octogenarians than in non-octogenarians. However, 30-day mortality (1.7% vs. 0.7%, P = 0.374) and 1-year mortality (6.9% vs. 2.9%, P = 0.108) were not statistically significantly different between the two groups.
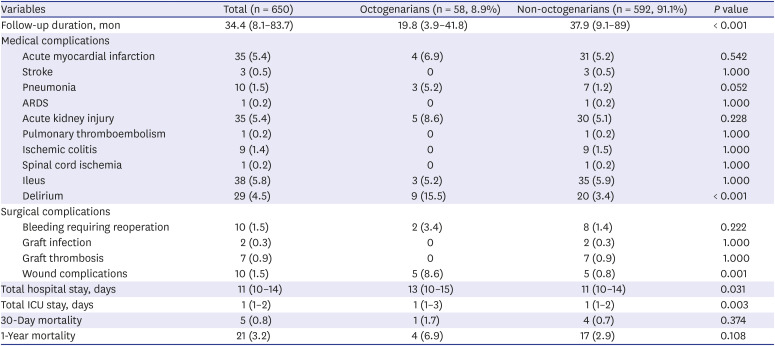
Table 3
Outcomes of elective open abdominal aortic aneurysm repair in octogenarians and non-octogenarians
Values are presented as median (interquartile range) or number (%).
ARDS = acute respiratory distress syndrome, ICU = intensive care unit.
![]()
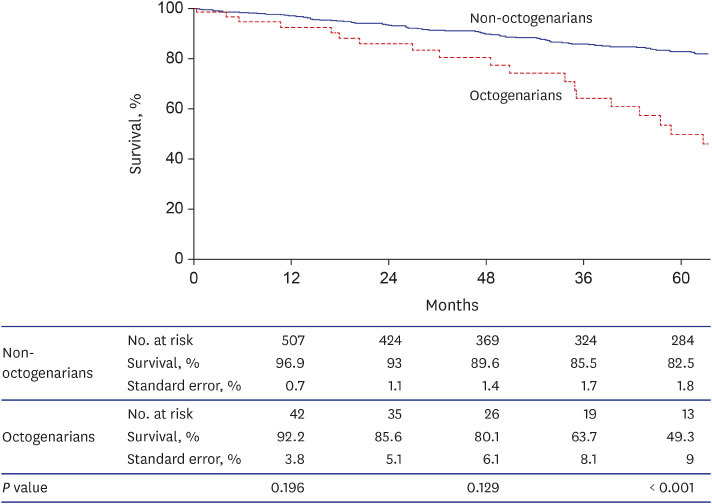
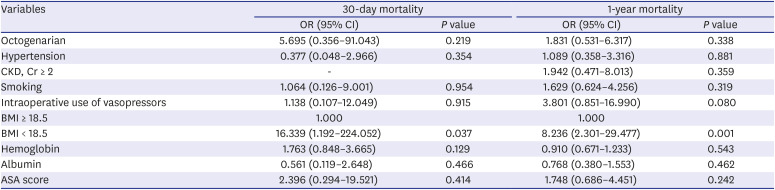
Table 4 shows the results of multivariable analysis of factors associated with 30-day and 1-year mortality after elective open AAA repair for all patients. Low BMI was associated with increased 30-day (OR, 16.339; 95% CI, 1.192–224.052; P = 0.037) and 1-year (OR, 8.236; CI, 2.301–29.477; P = 0.001) mortality in all patients. In Kaplan-Meier survival curve, significant difference was not observed in survival rate between the two groups until 36 months (Fig. 1). However, the survival rate at 60 months (49.3% vs. 82.5%, P < 0.001) was much lower in octogenarians than in non-octogenarians.
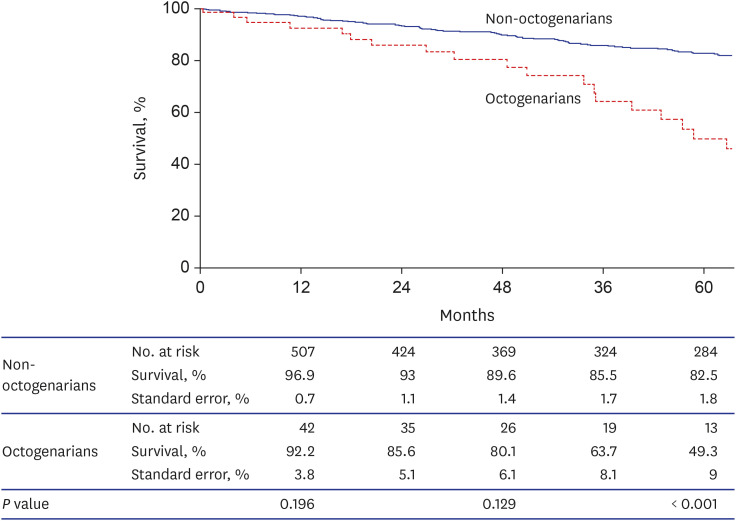 | Fig. 1Kaplan-Meier survival curve of octogenarians and non-octogenarians underwent elective open abdominal aortic aneurysm repair.
|
Table 4
Multivariate analysis of factors associated with 30-day and 1-year mortality after elective open abdominal aortic aneurysm repair (n = 650)
OR = odd ratio, CI = confidence interval, CKD = chronic kidney disease, Cr = creatinine, BMI = body mass index, ASA = American Society of Anesthesiologists.
![]()
Go to :
DISCUSSION
To the best of our knowledge, this is the first study in which the outcomes of open AAA repair in Koreans > 80 years of age were analyzed. With increased life expectancy and advances in aneurysm screening, the proportion of octogenarians among AAA patients has been increasing.1012 However, whether high operative risks and mortality after open AAA repair in octogenarians are acceptable is debatable.4131415 Considering the operative risks, the Society of Vascular Surgery (SVS) practice guideline 2018 suggests that open AAA repair be performed in centers with 10 or more cases annually and 30-day mortality rate below 5%.16 Our institution is a high-volume tertiary medical center in Korea that performs more than 50 elective open AAA repairs annually, performed by skilled surgeons with postoperative management experience.
The SVS practice guideline 2018 presents a mortality risk scoring scheme for repair of AAA, and its parameters are treatment option (EVAR or open), aneurysm size, age > 75 years, female, myocardial disease, cerebrovascular disease, chronic obstructive pulmonary disease, and serum creatinine ≥ 1.5 mg/dL.1 In the present study, octogenarians showed a larger aneurysm size and larger proportion of females and CKD compared with non-octogenarians, indicating higher overall operative risk in octogenarians. Preoperative serum hemoglobin and albumin levels were lower in octogenarians than in non-octogenarians. In previous studies, patients with moderate to severe anemia and hypoalbuminemia had higher rates of in-hospital mortality and morbidity after open AAA repair and EVAR.1718
Due to the greater amounts of RBC transfusion and vasopressor use in octogenarians, recovery in this population might be medically more demanding compared with non-octogenarians. Significant differences were not observed in surgical complications other than wound complication between the two groups; however, pneumonia and delirium were more prevalent in octogenarians. In a previous study, increasing patient age was associated with the incidence of postoperative complications after open AAA repair, including acute renal failure, pneumonia, and myocardial infarction.19 Most of these are medical complications that can contribute to longer hospital and ICU stay of octogenarians.
Despite the aforementioned factors in octogenarians, 30-day (1.7% vs. 0.7%, P = 0.374) and 1-year mortality (6.9% vs. 2.9%, P = 0.108), as well as survival rate, were not statistically significantly different between the two groups. The lower survival rate at 60 months (49.3% vs. 82.5%, P < 0.001) in octogenarians than in non-octogenarians might be affected by a relatively shorter remaining life expectancy and shorter follow-up duration. Lounes et al.20 demonstrated that excellent early and long-term outcomes can be achieved in patients unsuitable for standard EVAR in high-risk (age ≥ 80 years or ASA ≥ 3) groups after open AAA repair. The authors reported that all cause 30-day mortality was 2.2% and 5-year survival was 76% in high-risk patients. Morisaki et al.9 reported no difference in 30-day mortality rate between EVAR and open AAA repair in octogenarians, and aneurysm-related death was not observed. Based on the results of the present study, mortality outcomes of open AAA repair in octogenarians were acceptable and being elderly is not a contraindication for open AAA repair.
Davenport et al.21 reported that obese patients (30 < BMI < 35) had benefit in 30-day mortality after vascular surgery. This trend, called the "obesity paradox," might be due to differences in the metabolic makeup of obese patients and/or improved nutritional status compared with patients with lower BMI. The results of the present study indicate that aggressive nutritional and metabolic care should be included in the management of patients with AAA, especially for octogenarians in the immediate postoperative period to promote recovery after open repair. We plan to investigate this issue in future studies.
A paradigm shift has occurred in the treatment of AAA in recent decades because EVAR is preferred over open repair, especially in elderly patients with high operative risks due to the less invasive EVAR reportedly results in lower mortality during the perioperative period in octogenarians.1022 However, utilization of EVAR is associated with other difficulties. Considering operative risks and preference of a less invasive modality, IFU violation frequently occurs, ranging from 39–69% of cases.2324 In addition, the most common cause of IFU violations was unsuitability for proximal neck, which had a high-risk factor of type 1 endoleak.2526 In a previous study by Charbonneau et al.,27 EVAR was associated with a significantly worse long-term survival in patients who do not meet IFU anatomic criteria. Furthermore, their results showed the rate of at least one anatomic IFU violation for EVAR reached 43%.27 In addition, the long-term results of four major prospective randomized clinical trials confirmed a decreased early mortality advantage of EVAR.2829303132 And it was also identified in octogenarians.33
To overcome IFU violations, fenestrated EVAR and branched EVAR have been developed but have not been introduced in Korea. Furthermore, open AAA repair following EVAR results in significant morbidity and mortality, and IFU adherence of EVARs later requiring open AAA repair is markedly low.34 In addition, octogenarians is the independent risk factor of AAA sac enlargement after EVAR.35 Therefore, octogenarians not suitable for EVAR should be considered for open aneurysm repair instead of enforcement of an impractical EVAR as a minimally invasive surgery. However, low BMI might be associated with increased postoperative mortality, indicating the need for more aggressive postoperative care for octogenarians with low BMI.
The present study had several limitations. First, this was a retrospective study conducted in a single center. The total number of patients in the octogenarian group was relatively small compared with the non-octogenarian group, thus a certain degree of bias may have existed. In the future, systematic review or meta-analysis on this issue should be considered to overcome this limitation. Based on the present study results, low preoperative BMI was associated with increased mortality. However, the results have a limitation because they were analyzed for all age groups and not only for octogenarians. However, in terms of demonstrating acceptable outcomes of mortality due to open AAA repair in octogenarians, review of clinical outcomes of open surgical AAA in elderly patients should be emphasized.
In conclusion, because the mortality rate of octogenarians after elective open AAA repair was not significantly different from younger patients, being elderly is not a contraindication for open AAA repair. In the management of patients after open AAA repair, more aggressive nutritional support and metabolic care should be considered for octogenarians with low BMI which could be associated with increased postoperative mortality.
Go to :
 XML Download
XML Download