

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Oxford—AstraZeneca ChAdOx1 and Pfizer–BioNTech BNT162b2 vaccines are among the most commonly used severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; coronavirus disease 2019 [COVID-19]) vaccines worldwide. Clinical trial reports show that both vaccines exhibit excellent safety and immunogenicity12345; however, very few studies directly compare the efficacy of these vaccines,67 and the enduring public perception is that vaccine efficacy is dependent on the specific vaccine used, as well as the age and sex of the recipient. Indeed, some studies in the elderly, the group at greatest risk of severe consequences of COVID-19 infection, demonstrate that post-vaccination immunity is insufficient for protection.89
In Korea, according to the National Vaccination Plan, vaccination with the ChAdOx1 and BNT162b2 vaccines started in March 2021 for healthcare workers (HCWs) with priority.1011 In this prospective observational study, we compared the serostatus of participants, and the serum levels of anti-S antibody and neutralizing antibody of participants who were administered the ChAdOx1 vaccine with those who were administered the BNT162b2 vaccine. In addition, we investigated whether the antibody response to each vaccine (ChAdOx1 and BNT162b2) differed according to sex and age.
METHODS
Study population
From March 4 to June 15, 2021, at a general hospital in Goyang-si, Gyeonggi-do, Vaxzevria injection (ChAdOx1, adenovirus-vectored vaccine, AstraZeneca, Cambridge, UK) and Comirnaty injection (BNT162b2, mRNA vaccine, Pfizer-BioNTech; Pfizer, New York, NY, USA and BioNTech, Mainz, Germany) were administered. A total of 1,571 HCWs were vaccinated with two doses the ChAdOx1 vaccine at 12-week intervals, and 208 HCWs working in isolation wards or emergency departments received both doses of the BNT162b2 vaccine at 3-week intervals. HCWs who were vaccinated with two doses of either ChAdOx1 or BNT162b2 were invited to participate in this prospective cohort study. Following their first vaccination, HCWs who consented to participate in this study, including peripheral blood sampling, were followed prospectively.
Measurement of antibody titer and neutralizing antibody
Longitudinal blood sampling of the HCWs who received the ChAdOx1 vaccine was performed 4 and 8 weeks after the first dose. The HCWs received the second dose of the ChAdOx1 vaccine 12 weeks later, and the last blood collection was performed 2 weeks after the second dose (14 weeks after the first dose). HCWs vaccinated with BNT162b2 underwent blood sampling on the 3rd week after the first dose, followed by the second dose on the same day. Two weeks after the second dose (5 weeks after the first dose), blood samples were collected to test the antibody response.
Total anti-S antibodies (including immunoglobulin G [IgG]) against the spike (S) protein receptor binding domain (RBD) of the SARS-CoV-2 were measured by electrochemiluminescence immunoassay using the Elecsys® Anti-SARS-CoV-2 S immunoassay (Roche Diagnostics International Ltd, Rotkreuz, Switzerland). This is a quantitative assay, detecting anti-S antibody with a threshold value of 0.8 U/mL for positivity, and an upper limit of detection of 2,500 U/mL. Seropositivity rates and levels of the anti-S antibody from blood samples from trial participants after both the first and second doses of ChAdOx1 and BNT162b2 vaccines were compared. The signal inhibition rate (SIR, %) was used to assess the capacity of antibodies to neutralize, in this case a surrogate virus. The cPass™ ELISA-based SARS-CoV-2 surrogate virus neutralization antibody detection test kit (Genscript Biotech Corporation, Piscataway, NJ, USA), applies an indirect detection method via assessing antibody-mediated inhibition of SARS-CoV-2 RBD binding to the human host receptor angiotensin-converting enzyme (ACE) 2. The test is comparable to the gold standard of antibody testing in viral diseases the plaque reduction neutralization test.121314 The percentage inhibition was calculated using the equation below. For interpretation of the data, we applied a 30% cut-off value; samples were deemed positive if they exhibited an SIR greater than 30% and negative if the rate was less than 30%.

We compared anti-S and neutralizing antibody levels between ChAdOx1 and BNT162b2 vaccinees after the first dose and second dose. In addition, differences in antibody responses according to sex and age were compared and analyzed.
Statistical analysis
Continuous variables are presented as medians with interquartile ranges (IQRs) or means with standard deviations (SDs), and categorical variables are presented as frequencies. Differences between continuous variables in the vaccination groups were evaluated using the paired t-test, and for categorical variable differences the χ2 test was applied. Trends in the antibody titers and SIRs according to age were assessed using penalized smoothing splines methods to show the differences in the trends between the ChAdOx1 and BNT162b2 vaccines. The data were analyzed using R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at a 2-sided P value < 0.05.
RESULTS
Demographic data
After their first vaccination and giving consent, 211 and 107 HCWs who had received the ChAdOx1 and BNT162b2 vaccines, respectively, were followed in this prospective observational cohort study. Of the 211 HCWs enrolled in the ChAdOx1 vaccination group, three individuals did not receive the second dose and another three later withdrew from the study, leaving a cohort of 205. Of the 107 participants in the BNT162b2 vaccination group, 2 individuals who reported previous SARS-CoV-2 infections were excluded and 1 individual withdrew from the study, totaling to 104 participants (Supplementary Fig. 1). We obtained 823 blood samples from 309 study participants (615 samples from 205 ChAdOx1-vaccinated participants and 208 samples from 104 BNT162b2-vaccinated participants). The median age of the study participants was 40 years (IQR, 20–41.11), 51 participants (16.5%) were over 55 years old, and 211 (68.3%) were women. There was no difference in average age between the ChAdOx1 vaccine group and the BNT162b2 vaccine group, but the BNT162b2 group had more participants aged 55 years or older (P < 0.05). The proportion of women in the ChAdOx1 group was 74.1%, which was higher than that in the BNT162b2 group (P < 0.05; Table 1).
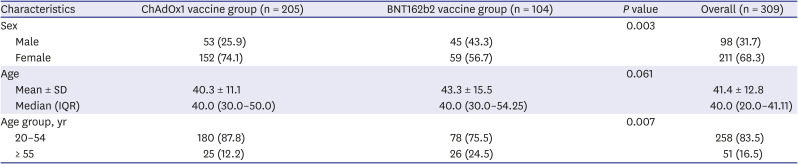
Table 1
Demographics of participants
Sex and age of the 309 participants are indicated. Values are expressed as number (%) or mean ± SD or median (IQR).
SD = standard deviation, IQR = interquartile range.
![]()
Comparison of anti-SARS-CoV-2 antibody response between ChAdOx1 and BNT162b2 vaccinees
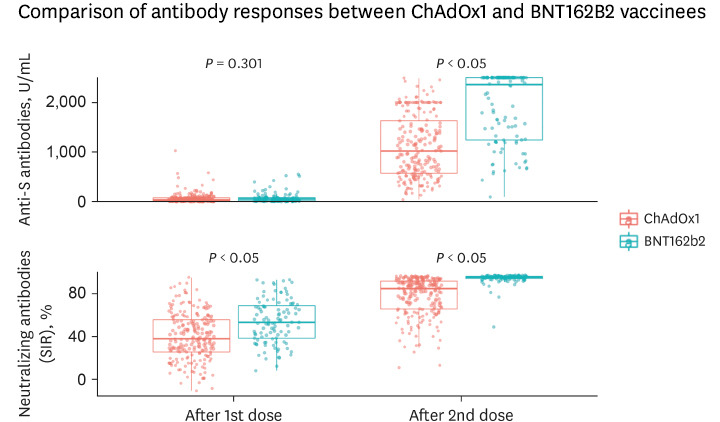
At two weeks-post second doses of both ChAdOx1 and BNT162b2 vaccines, all participants (100% in both groups) were seropositive for anti-S antibodies. In the ChAdOx1 group, 66.8% (137/205) of the participants exhibited a detectible level of neutralizing antibody after the first dose and 98.0% (201/205) of participants after the second dose. This means that following the full, two-dose vaccination schedule, four participants in the ChAdOx1 group were seronegative for neutralizing antibody. In contrast, following completion of the vaccination schedule in the BNT162b2 group, all participants (100%, 104/104) were seropositive for both anti-S and neutralizing antibodies (Table 2). There was no significant difference in the anti-S antibody titer between the ChAdOx1 and BNT162b2 groups after the first dose, but the SIR of the neutralizing antibody was higher in the BNT162b2 group (P < 0.05). After the second dose, the median level of anti-S antibody and SIR of the neutralizing antibody were all significantly higher in the BNT162b2-vaccinated group than the ChAdOx1 group (anti-S antibody, 1,020 [IQR, 571.0–1631.0] U/mL vs. 2,360 [1,243–2,500] U/mL, P < 0.05, for the ChAdOx1 and BNT162b2 groups, respectively; neutralizing antibody, 85.0 [65.9–92.1%] vs. 95.8 [94.4–96.6%], P < 0.05, for the ChAdOx1 and BNT162b2 groups, respectively) (Fig. 1, Supplementary Table 1). There were no statistically significant antibody response changes at weeks 4 and 8 after the first dose of ChAdOx1, and the results 2 weeks after the second dose showed a statistically significant change (Fig. 2). The anti-S antibody titers and the neutralizing antibody SIR showed a strong positive correlation (R = 0.89; Fig. 3).
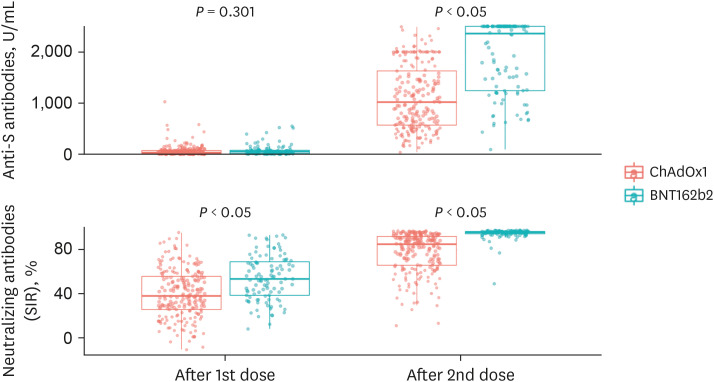
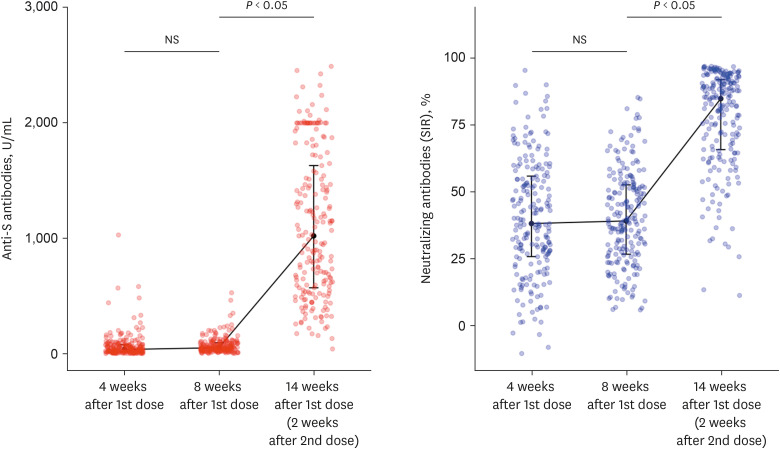
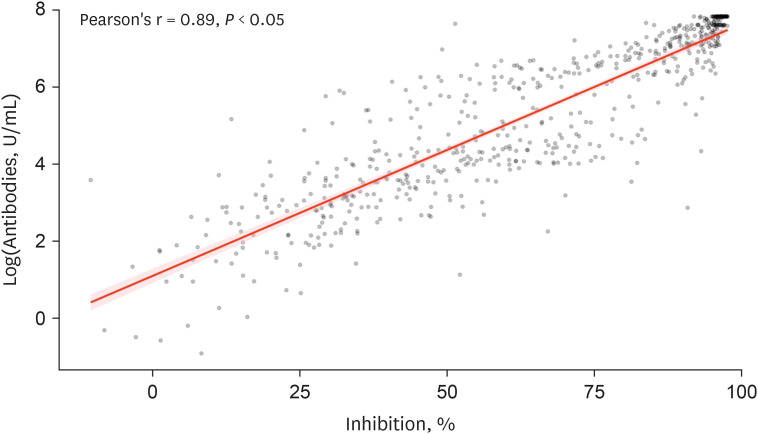

Fig. 1
Comparison of antibody responses between ChAdOx1 and BNT162b2 vaccinees. Antibody titers after 1st and 2nd doses of ChAdOx1 and BNT162b2 vaccines are shown.
SIR = signal inhibition rate.
![]()
Fig. 2
Antibody responses after 1st and 2nd dose in ChAdOx1 vaccinees. The antibody titers showed no significant difference at 4 and 8 weeks after the first dose but increased markedly after the second dose of ChAdOx1 vaccine.
NS = not significant, SIR = signal inhibition rate.
![]()
Fig. 3
The correlation between SARS-CoV-2 anti-S antibodies (U/mL) and neutralization rate (%). SARS-CoV-2 anti-S antibody and neutralizing antibody titers showed a strong positive correlation (Pearson's r = 0.89).
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
![]()
Table 2
Seropositivity of anti-S and neutralizing antibody
![]()
Differences in antibody response according to sex
After the first dose, women in the ChAdOx1 group showed anti-S antibody titers and neutralizing antibody SIRs that were significantly higher than those in men of the same group (anti-S antibody, 49.6 (20.6–86.3) U/mL vs. 21.3 (8.7–39.8) U/mL, P < 0.05, for women and men, respectively; neutralizing antibody, 44.2 (28.9–59.5%) vs. 30.2 (15.3–43.2%), P < 0.05, for women and men, respectively). However, subsequent to the second dose of ChAdOx1, there was no discernable difference related to sex of the recipient for titer of anti-S antibody while the median SIR values of neutralizing antibody remained significantly higher in women than in men (85.7 [70.3–92.5%] vs. 77.7 [59.2–91.0%]; P < 0.05, neutralizing antibody SIR in women vs men, respectively). Regarding the BNT162b2 vaccine, after the first dose, the levels of anti-S and neutralizing antibodies were higher in women than in men (anti-S antibody, 57.1 [25.4–87.0] U/mL vs. 34.5 [13.1–72.9] U/mL; P = 0.147, for women and men, respectively; neutralizing antibody, 61.6 [44.9–71.2%) vs. 47.3 (34.5–58.3%), P < 0.05). On completion of the vaccination schedule (two doses), there was no demonstrable difference in respect to sex of the participants in the BNT162b2 group in either the titer of anti-S antibody or the SIR of neutralizing antibody (Fig. 4, Supplementary Table 2).
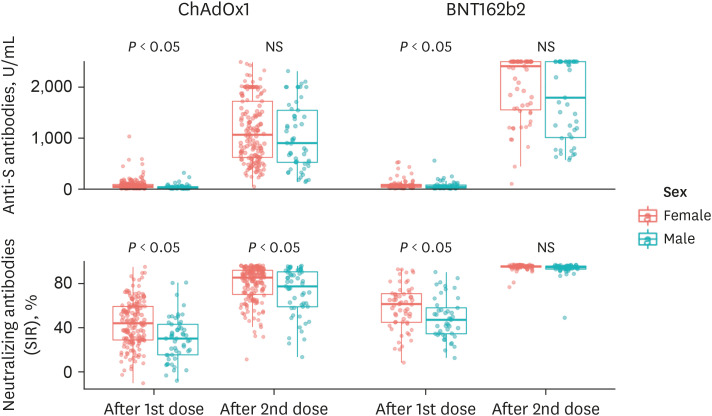
Fig. 4
Difference in anti-S titers and neutralizing antibody titers between two sexes. After the 2nd dose of ChAdOx1 vaccine, the neutralizing antibody titer was higher in females than in males. Regarding the BNT162b2 vaccine, after the 1st dose, the levels of anti-S and neutralizing antibodies were higher in females than in males, but there was no difference in the antibody titers between the sexes after the 2nd dose.
NS = not significant, SIR = signal inhibition rate.
![]()
Differences in antibody response according to age
To compare the age-related differences in antibody responses between the ChAdOx1 and BNT162b2 groups, the study groups were categorized as 20–54 years, and 55 years and older. Following the initial dose of ChAdOx1, blood samples from the participants showed no significant age-related differences for either anti-S antibody titers or neutralizing antibody activities. However, following the second dose, neutralizing antibody SIR was significantly higher in the younger age group (20-54 years) than in the older group (85.4 [66.9–92.3%] vs. 75.6 [58.1–89.5%]; P < 0.05, neutralizing antibody SIR in the younger age group vs. the older age group, respectively), while anti-S antibody titers showed no difference (Fig. 5A, Supplementary Table 3). Analysis of the overall trend of anti-S antibody and neutralizing antibody SIR according to age, anti-S antibody showed a decreasing trend with age, but the difference was not significant (R = −0.093; P = 0.190), and the neutralizing antibody SIR showed a significantly decreasing trend with increasing age (R = −0.18; P < 0.05; Fig. 5B).

Fig. 5
Level of anti-S and neutralizing antibodies according to the age. (A) In ChAdOx1 vaccine group, the neutralizing antibody titer was slightly higher in the younger age group than in older age group after the second dose. In the BNT162b2 group, there was no significant difference in the antibody response according to age after the second dose. (B) For anti-S and neutralizing antibody, the antibody levels of individuals are plotted against patient age in both vaccine groups with the best fit lines, Pearson's correlation (R) and P value (P). In both vaccine groups, neutralization tended to decrease with age.
SIR = signal inhibition rate.
![]()
In the BNT162b2 group, both anti-S antibody and SIR were significantly higher in the younger age group than in the older age group after the first dose (Fig. 5A, Supplementary Table 3). Although there was no significant difference in anti-S antibody and SIR in HCWs aged < 55 years and those aged ≥ 55 years after the second dose, when the trend was analyzed for all age groups, even after the second dose of BNT162b2, the anti-S antibody (R = −0.24; P < 0.05) and SIR (R = −0.28; P < 0.05) both tended to decrease significantly (Fig. 5B).
DISCUSSION
In this study, we investigated the antibody responses in a pool of HCWs who had been vaccinated with either ChAdOx1 or BNT162b2. Both SARS-CoV-2 ChAdOx1 and BNT162b2 vaccines elicited a robust immune response after two doses, with 98% to 100% of the participants in both groups being seropositive for the anti-S and the neutralizing antibody. This study demonstrated a significantly higher humoral immune response to the BNT162b2 vaccine compared to that of the ChAdOx1 vaccine. In the ChAdOx1 group, the women had significantly higher neutralizing antibody levels than the men. Both the anti-S antibody titer and neutralization rate showed a tendency to decrease as participant age increased, irrespective of vaccine type.
To the best of our knowledge, this study is the first to provide a direct comparison of antibody titers and neutralizing antibody SIR between the ChAdOx1 and BNT162b2 vaccines, and to demonstrate the efficacy of these two major vaccines according to sex and age.
The main proteins of SARS-CoV-2 are the spike, small envelope, membrane, and nucleocapsid proteins.151617 The first step for the virus to invade host cells is to bind to the ACE2 receptor, where the role of the spike protein is important, and several experiments have shown that blocking the RBD of the S protein is the most important target of the COVID-19 vaccine.18192021 In addition, it was found that the appearance of neutralizing antibodies against the RBD of the S protein coincided with the actual protective effect.22 Thus, the basic strategy of the COVID-19 vaccine is to neutralize the RBD of the S protein of SARS-CoV-2.17
In the phase 1/2 clinical trial, at 28 days-post primary vaccination the ChAdOx1 vaccine elicited a result of 157 ELISA units (EU) (IQR, 96–317; n = 127) of anti-spike (S protein) IgG antibodies and following the second dose a result of 639 EU (IQR, 360–792; n = 10). Neutralizing antibodies were formed in 91% of recipients and 100% of recipients after the booster.2 The Phase 2/3 clinical trial showed various antibody titers and neutralizing antibodies according to age. In the case of ChAdOx1, older adults and younger adults showed similar immunogenicity across all age groups after the booster.3 In phase 3 clinical trials, the overall vaccine efficacy observed in the UK, Brazil, and South Africa was 70.4% (95.8% confidence interval [CI], 54.8–80.6).2 When the BNT162b2 mRNA vaccine was administered twice in the 30 mcg administration group, the antibody against the spike protein was well expressed (young people 9,136, the elderly 7,985), and the neutralizing antibody was expressed slightly lower in the elderly people.4 In the BNT162b2 vaccine Phase 3 clinical trial, the vaccine efficacy was 95% (95% CI, 90.3–97.6).1
There are still a few reports of antibody response after vaccination in Korea; however, there is a report that 100% of the antibodies measured by two different methods were confirmed in the 1st and 2nd weeks in a study of 289 HCWs who had completed the BNT162b2 vaccination.23 It is difficult to directly compare the results with those of previously published studies because the measurement methods and population composition are diverse. In this study, when the second dose was completed, the ChAdOx1 vaccine showed a 100% seropositivity rate of anti-S antibodies and a 98.0% seropositivity rate of neutralizing antibodies. The BNT162b2 vaccine showed higher levels of anti-S and neutralizing antibodies and SIR than the ChAdOx1 vaccine. Although high levels of anti-S antibodies, seropositivity rate, or SIR of neutralizing antibodies cannot fully explain the protective effect against SARS-CoV-2 infection, a correlation between vaccine-elicited immune response and protection has been established.2224 Measuring antibody levels is much easier than direct measurement of vaccine efficacy over time.22 We observed a correlation between neutralization activity and anti-S antibodies in the serum; this result is consistent with that reported in previous studies.2526
Previous studies have shown that women have a stronger immune response to infection and vaccination and have higher antibody responses to vaccines than men.2728 Women have an overall tendency to have higher antibody responses, and faster waning of antibodies has been shown following several vaccines.2930 This may be related to sex hormones, X-chromosome, and environmental factors.3132 In addition, in patients with COVID-19, T-cell activation occurred more strongly in women than in men, which also affected the response period.273334 In this study, the overall antibody titer was high in women after the initial dose in both vaccine groups; however, this sex-associated difference was eradicated by the second vaccination of the BNT162b2 vaccine. In the ChAdOx1 vaccine group, after the second dose, the anti-S antibody showed no sex-related significant difference, but the SIR of neutralizing antibody remained slightly higher in women.
The elderly population (adults over 65 years of age) is at particularly high risk for severe COVID-19, accounting for approximately 80% of hospitalizations and a higher fatality rate, and require prioritization in vaccination campaigns.935 In both vaccines, it was reported that antibodies were identified even in the elderly group in clinical trials and some reports, and that they had a protective effect.13436 However, it is well known that vaccine responses are low in the elderly, who also have more rapid waning of antibodies and immunosenescence.29 Delayed and reduced antibody and T-cell responses after BNT162b2 vaccination were observed in a German study comparing vaccine-elicited humoral and cellular responses in elderly persons (71 persons, median age 81 years) and healthy young HCWs (123 persons, median age 34 years).8 The BNT162b2 vaccine showed a significant difference according to age at the first dose, but this difference was not observed after the second dose. In this study, based on two age group categories, the level of antibody response to either vaccine was not significantly associated with age. A slight negative correlation between antibody titer and age was noted, that is, the antibody titer decreased as participant age increased, but the relationship between the variables was weak. Specifically, the results of this study indicate that the antibody response following one dose of vaccine in the elderly population may be slightly lower than that of the younger population, however, focusing on infection control and prevention, on completion of the full vaccination schedule, an appropriate protection level can be achieved irrespective of age.
This appears to be due to the prominent increase in anti-S and neutralizing antibodies by the boosting effect, thus implying that the second dose is indeed very important. However, whether an additional booster dose is required after the second dose is still controversial, and additional research is needed on waning immunity over time, and the need for a booster dose may arise depending on the durability of the vaccine-induced antibody.
This study had some limitations. First, we did not measure the antibody titers before vaccine administration. Second, we aimed to compare the antibody titer and SIR between the ChAdOx1 and BNT162b2 vaccines, but this was not a randomized clinical trial for a head-to-head comparison of these two vaccines. However, the study population could not choose the vaccine, and the vaccine was provided according to the vaccine priority defined by the Korean government (KCDC). As shown in Table 1, the ChAdOx1 and BNT162b2 vaccine groups did not show significant differences in baseline characteristics. Therefore, we believe that the trends in the antibody titers and SIR of the ChAdOx1 and BNT162b2 vaccines in the present study can reflect real-world practice. Third, the vaccine-derived humoral immune response may be stronger in women, and the relatively high proportion of women among the study HCWs may have created some bias. To the best of our knowledge, sex- and age-related data directly comparing the antibody responses of the ChAdOx1 and BNT162b2 vaccines are limited. Understanding these sex- and age-associated variables may contribute to optimizing vaccine policy in the target population, and consequently, data that details the efficacy of different vaccines will contribute to decision making.
In conclusion, both the ChAdOx1 and BNT162b2 vaccine groups showed high anti-S antibody and high neutralizing antibody seropositivity after the second dose in this prospective observational cohort study. The ChAdOx1 vaccine showed a higher tendency for SIR by neutralizing antibodies in women. Enhanced antibody responses were observed with the BNT162b2 vaccine compared to the ChAdOx1 vaccine. Additional research is required to determine the longevity of the immune response to vaccination; furthermore, contingent on the persistence of the immune response or the emergence of new variants, booster vaccinations may be necessary. Real-world data on clinical vaccine efficacy are imperative.
 XML Download
XML Download