

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cancer patients have functional limitations and symptoms that affect their health-related quality of life.1 Fatigue, pain, and chemotherapy-induced peripheral neuropathy can restrict activities of daily living.23 Cancer-related impairments are caused by adverse neural, musculoskeletal, and cardiopulmonary events, metastatic and regional tumour spread, and cancer treatments,4 Impairment-driven cancer rehabilitation5 can improve quality of life by controlling aggressive symptoms and enhancing physical function and performance.6 Increasing evidence indicates that multidimensional rehabilitation programmes benefit cancer survivors.7
Advanced cancers are associated with more severe symptoms and greater impairment.8 Although most patients (88%) with metastatic cancer would benefit from rehabilitation, few patients (21%) receive physician-directed rehabilitation therapy.4 A cross-sectional study from Norway observed that 63% of cancer patients reported a need for at least one rehabilitation service, while 40% reported unmet needs.9 Although the utilisation of rehabilitation is tailored to the needs and values of individual patients,7 it is heavily influenced by health insurance policy. In Korea, insurance claims for rehabilitation therapy are categorised according to treatment type and duration,10 similar to the system in Taiwan. Cancer rehabilitation therapies are not currently reimbursed11; medical treatments are reimbursed by reference to disease codes. To meet the need for rehabilitation, there is a need to revise the current reimbursement criteria for rehabilitation in the insurance system, as well as the associated fees for cancer patients.
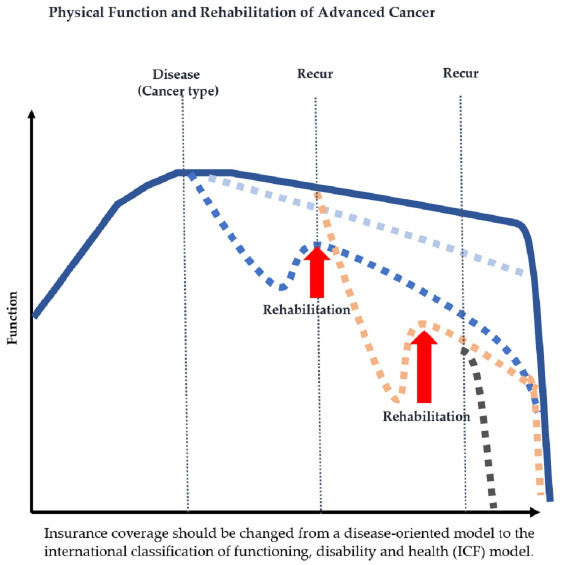
In Korea, insurance benefits focus on treatments for disease, and the basic payment scheme follows a pay-per-service model. Rehabilitation therapy can also be reimbursed based on disease status with a focus on the central nervous system (CNS) and bone lesions, rather than impairment status. The International Classification of Functioning, Disability, and Health model is not embedded in the current scheme. In this study, we investigated rehabilitation therapy utilisation by patients with cancer, using nationwide data that represent the whole population in Korea. We also analysed whether patient characteristics, including cancer type and stage, were associated with rehabilitation therapy utilisation We used data from the National Cancer Registry, which is linked to the claims database of the National Health Insurance Service (NHIS).
METHODS
Data source
We obtained data from the Korea Central Cancer Registry (KCCR) for the period January 1, 2011 to December 31, 2015. This was linked to data on health insurance claims and death rates for the 9-year period from January 1, 2009 to December 31, 2017 provided by the Korean NHIS (Research No: NHIS-2018-1-184). We included all cancer patients older than 18 years who were diagnosed during 2011–2015 and listed in the KCCR, which can be linked to claims data from the NHIS.
The KCCR is a nationally representative, population-based cancer registry covering > 99% of patients diagnosed with cancer in South Korea. It contains nationwide cancer incidence and survival data from 1999 onward.12 Diagnoses are made in accordance with the Surveillance, Epidemiology, and End Results (SEER) system. The SEER stages are as follows: localised (limited to the organ of origin), regional (tumour extends beyond the organ of origin), distant (away from the primary tumour), and unknown. We considered the distant SEER stage to correspond to advanced cancer.
The NHIS is a mandatory medical insurance program in South Korea that was introduced in 1977 and achieved universal coverage by 1989.1314 The NHIS contains data on diagnoses, procedures, prescriptions, demographics, direct medical costs, and mortality, with no duplications or omissions. Diagnoses are coded according to the International Classification of Diseases, 10th edition (ICD-10).
The direct medical costs are in South Korean Won (KRW) (1 USD = 1,138.5 KRW). Only insured services are considered. In this study, rehabilitation costs included those for physical, occupational, and speech/swallowing therapy.
Rehabilitation therapy utilisation
We assessed the utilisation of rehabilitation therapies by identifying claims with procedure codes for therapeutic exercise to improve functional performance, one of physical therapy (PT), not just for symptom management (e.g., manual, heat and electrical therapy) and other rehabilitation (e.g., occupational therapy (OT), swallowing therapy for dysphagia, complex decongestive therapy for lymphedema, and biofeedback therapy for pelvic floor dysfunction) from the same year in which patients were newly registered as cancer patients.
The NHIS has various rehabilitation therapy categories. In the ICD-10, the categories are based on the cost of an insurance claim, not the severity of disability. For therapeutic exercise, the categories are “simple,” “moderate,” and “special.” Taking therapeutic exercise as an example, special claims correspond to a program delivered by highly skilled physical therapists according to the full-time physiatrist's prescription, respectively, with sessions lasting at least 30 minutes. In Korea, special therapy is prescribed mostly for CNS disorders. Moderate claims correspond to muscle strengthening exercise and functional training at least 30 minutes. Simple claims correspond to 10 minutes of exercise, which is too short to be considered rehabilitative.
RESULTS
Characteristics of the study population
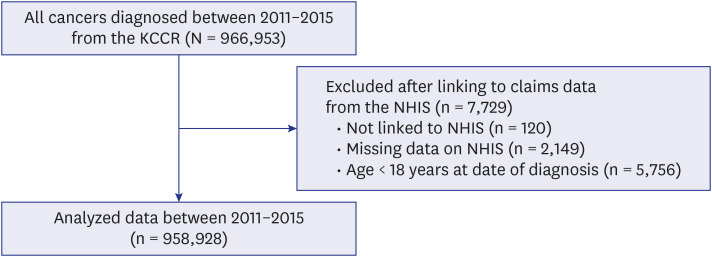
We identified 966,953 patients registered in the KCCR from 2011 to 2015, but 7,729 patients were excluded from analysis because of not linking to NHIS (n = 120), missing data on NHIS (n = 2,149), or younger than 18 years at date of diagnosis (n = 5,756). A total of 958,928 incident cancer cases registered in the KCCR were linked with health insurance claims data (Fig. 1). For the years 2011 to 2015, the KCCR contained 192,835 (20.1%), 197,800 (20.6%), 196,921 (20.5%), 188,288 (19.6%), and 183,844 (19.1%) patients with cancer who met the study inclusion criteria, respectively. The average patient age was 60 ± 14.4 years and 50.4% were male. The proportion of patients classified with distant cancer was 18.3% (n = 175,548). During follow-up, 305,102 (31.8%) of all cancer patients died, including 139,210 (79%) classified with distant cancer.
Rehabilitation therapy utilisation
Of the cancer patients, 61,059 (6.4%) had claims for rehabilitation therapy. The numbers of patients who had claims were 52,292 (5.5%) for total therapeutic exercise (simple:moderate:special = 34,456 [3.6%]:16,378 [1.7%]:7,564 [0.8%]). The utilisation rate increased during the study period, from 6.0% (11,504) of 192,835 newly diagnosed patients in 2011 to 6.8% (12,455) of 183,084 newly diagnosed patients in 2015 (Fig. 2). The number of patients who had claims for therapeutic exercise also increased from 9,980 (5.2%) in 2011 to 10,555 (5.8%) in 2015. The number of patients who received total rehabilitation therapy within 1 year after a diagnosis of cancer (total 96,877) increased gradually throughout the study period, from 18,689 in 2011 to 19,870 in 2015. The mean interval from diagnosis to the initial rehabilitation therapy was 76.5 days (range: 78 days).

Rehabilitation therapy according to patient characteristics
Table 1 shows the characteristics of newly diagnosed cancer patients who did and did not claim rehabilitation treatments categorized as therapeutic exercise subdivided as simple, moderate or special therapy and other rehabilitation. The prevalence of therapeutic exercise is calculated by dividing the number of persons who claim the therapeutic exercise by the number of individuals registered, while the prevalence of special therapy by dividing the number persons who claim the special therapy by dividing the number of persons who claim the therapeutic exercise. Females were more likely to claim for physical rehabilitation than males in total therapeutic exercise claims (female vs. male = 29,232 [6.1%] vs. 23,060 [4.8%]), while males were more likely to claim for special therapy (female vs. male = 2,940 [10.1%] vs. 4,624 [20.1%]). The median ages of rehabilitation nonusers, users of total therapeutic exercise and special therapy were 60.3, 61.5 and 66.4 years, respectively. Among patients in their 60s and 70s, there were slightly more users of total therapeutic exercise and special therapy than nonusers. The proportion of users of total therapeutic exercise and special therapy were slightly higher among those receiving medical aid compared to those with a high monthly income, respectively (2,935 [6.8%] vs. 11,429 [5.3%], 578 [19.7%] vs. 1,531 [13.4%]).
Table 1
Utilisation of rehabilitation therapy according to patient characteristics
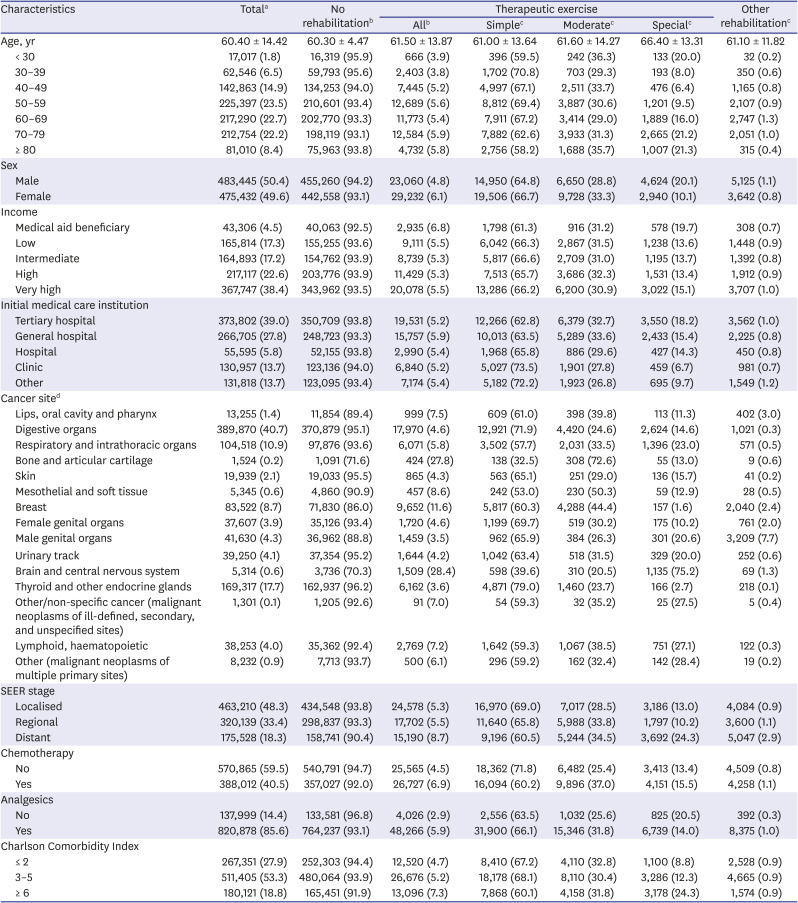
Values are presented as mean ± standard deviation or numbers (%).
SEER = Surveillance, Epidemiology, and End Results.
aPercentage of the total; bPercentage of the total in each subgroup; cPercentage of the total in each subgroup receiving exercise rehabilitation; dCancer sites were categorised using the Korean standard. “Other” rehabilitation includes occupational therapy, swallowing therapy for dysphagia, complex decongestive therapy for lymphedema, and biofeedback therapy for pelvic floor dysfunction.
The types of medical care institution initially visited did not differ significantly between rehabilitation nonusers and users. However, among patients who received therapeutic exercise, those who visited a tertiary hospital initially were more likely to receive special therapy than patients who visited another type of hospital (3,550 [18.2%] vs. 427 [14.3%]).
The most prevalent diseases were gastrointestinal (40.7%), thyroid (17.7%), respiratory (10.9%), and breast (8.7%) cancers (Table 1). Patients with CNS cancer were most likely to receive therapeutic exercise (1,509 [28.4%]), especially special therapy (1,135 [75.2%]). Patients taking analgesics were more likely to receive all types of rehabilitation therapy than patients not taking them. Patients with a CCI ≥ 6 were more likely to receive therapeutic exercise than patients with a CCI < 2 (13,096 [7.3%] vs. 12,520 [4.7%]); the difference was more pronounced for special therapy (3,178 [24.3%] vs. 1,100 [8.8%]).
Utilisation of therapeutic exercises according to cancer stage and type
Fig. 3 shows the utilisation of therapeutic exercises of cancer patients stratified by SEER stage. The rate of therapeutic exercise was higher in distant cancer patients than in localised or regional cancer patients (8.7% vs. 5.3% vs. 5.5%). In addition, the proportion of patients receiving special therapy was higher among those with metastases than localised or regional cancer (1.47% vs. 0.69% vs. 0.56%).
Fig. 3
Prevalence of the utilisation of rehabilitation (simple, moderate, or special) by cancer patients according to the SEER stage.
SEER = Surveillance, Epidemiology, and End Results.

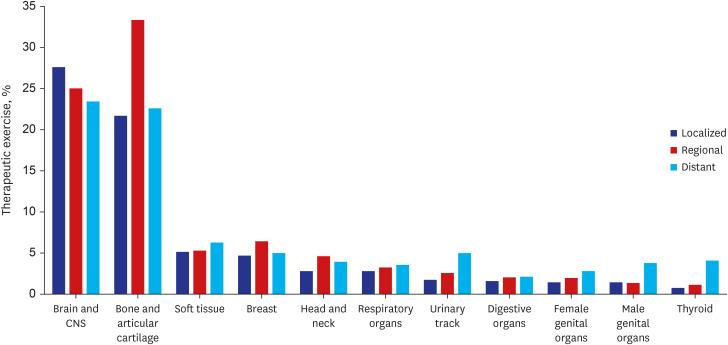
When comparing the prevalence of therapeutic exercise by the primary cancer type and SEER stage, simple therapeutic exercise (MM101) was excluded because it is only 10 minutes in duration, which is too short for rehabilitation purposes (although it is widely used by primary healthcare services to treat musculoskeletal problems).
Among patients with localised cancers, those with primary tumours in the CNS (27.5%) and bone (21.7%) were more likely to receive therapeutic exercise (Fig. 4). Fewer than 5% of patients with other types of cancer engaged in therapeutic exercise. A similar pattern was evident among those with distant metastasis. Patients with primary tumours in the CNS (23.5%) and bone (22.7%) were more likely to receive therapeutic exercise. However, even though patients with other types of primary cancer might be severely disabled by distant metastasis, the therapeutic exercise rate was below 6%. Patients with advanced primary digestive organ tumours were the least likely to be treated (2.1%). Therapeutic exercise was more common in patients with metastatic than localised cancers of the thyroid (4.1% vs. 0.7%), urinary track (5.1% vs. 1.7%), and male genital organs (3.8% vs. 1.4%).
DISCUSSION
In this large Korean population-based study, only 6.4% of the cancer patients received physical rehabilitation. Although patients with distant metastasis used more intensive rehabilitation than early cancer patients, rehabilitation therapy was unevenly distributed among the cancer types. Patients with bone or brain cancer, who were previously eligible for special therapy, were more likely to receive rehabilitation therapy.
The utilisation rate of rehabilitation therapy was far below those reported elsewhere. Podnos et al.15 investigated the referral rates for rehabilitation among patients with newly diagnosed lung cancer, and found that 31% of the referrals were for pulmonary rehabilitation, while 19% were for PT or OT. In Denmark, among 13,059 persons diagnosed with cancer, 2,523 (19%) were referred for rehabilitation within 2.5 years of diagnosis.16 Although cancer rehabilitation services are cheaper in Korea than other countries,17 uptake remains low. Cheville et al.4 reported that 92% of metastatic breast cancer patients had at least one physical impairment. Of 530 identified impairments, 484 (92%) required physical rehabilitation and 469 (88%) PT or OT, although only 30% of impairments requiring rehabilitation and 21% of those requiring PT/OT were actually treated. Large rehabilitation departments have emphasised cancer over the last decade, and reimbursement for rehabilitation services has declined.18 Among patients with diseases such as stroke, cerebral palsy,19 and Parkinson's disease,4 as well as cardiac problems, the rate of utilisation of rehabilitation is even lower in Korea. Of patients with Parkinson's disease, 35–40% claimed for PT and 16–19% for OT.4 Among children with cerebral palsy, 28.6% and 81.3% underwent inpatient and outpatient PT, respectively.
There was no remarkable change in the rate of rehabilitation utilization during this period, however, increased none the less, which suggests the evidence-based practice increasing in Korea and more therapy being available. In addition, providers and health care systems are preparing of the shift from a fee-for-service reimbursement models to a value-based reimbursement methodology slowly. If value-based reimbursement models are implemented in rehabilitation service, patient-centered rehabilitation will be facilitated.
Barriers to referral for, and utilisation of, rehabilitation in Korea include poor understanding of the effectiveness of rehabilitation services among cancer patients and the lack of a cooperative referral system.11 We found that factors associated with the insurance system itself can promote underutilisation. While the numbers of physiatrists and physical therapists relative to the population in Korea are close to those in other countries, there is an uneven distribution of resources. Comprehensive insurance coverage can encourage healthcare providers to increase access to services. The medical costs of rehabilitation are not high, at less than 10% of all medical costs. The lower price per visit compared to other countries is a barrier to healthcare providers.
In our study, rehabilitation treatment was unevenly distributed among cancer types. Patients with bone or brain cancer were more likely to receive rehabilitation. This may not be attributable only to the fact that patients with bone and brain cancer have severe disability. In an Australian population-based cohort study, Joshy et al.20 found that the outcomes varied by cancer type, being worst for multiple myeloma, lung cancer, and non-Hodgkin's lymphoma. Disability in association with certain cancers may be attributable to a lower cure rate (e.g., lung cancer), higher treatment toxicity, and higher prevalence of comorbid disease.20 Compared to Australia, the variation in rehabilitation utilisation across cancer types in Korea can be explained by the characteristics of the insurance claims system itself. Patients with bone or CNS lesion experience disability in specific domains, such as mobility, and interventions for ambulation are covered by the Korean insurance system. In addition, pulmonary rehabilitation for lung cancer patients has been covered by insurance since 2016 by which the trend could be changed in future studies. The insurance reimbursement criteria for complicated, specialised therapies are based on the disease code, not the level of impairment. The diagnosis of cancer itself is not a criterion for reimbursement. The variable patterns of insurance use suggest that care is managed poorly.21
Specific rehabilitation therapies for lymphedema, dysphagia, and pelvic floor dysfunction have their own claims codes in our insurance system. Upper limb dysfunction is reported in 30–40% of breast cancer patients and lymphedema in 10–40%, with the rates varying according to the assessment method.2223 In our study, the rehabilitation utilisation rate by patients with breast cancer was 11.6%, which is substantially lower than the rate of complications after breast cancer treatment.24 Accessibility is an important factor related to the underutilisation of rehabilitation therapy. Lack of recognition of the important factors; other important factors include limited training of physiatrists25 and problems with service delivery.112627
In South Korea, the healthcare system is based on universal coverage; maximum coverage is sought in the context of limited resources. Important questions about health care can often be answered by studying health care utilisation.21 Rates of utilisation can reveal differences in the needs of specific subgroups. Resources are allocated based on cost-effectiveness, rather than absolute values, where effectiveness is determined by outcomes. For cancer rehabilitation, “pay per value” is the appropriate outcome measure for an insurance system, not “pay per activity” or “pay per time”. Patients with cancer are a heterogeneous group in terms of functional level; their physical impairments differ by type and stage of cancer.
Rehabilitation utilisation was higher among patients with distant-stage cancer than those among those with localised or regional cancer. Living with incurable/metastatic cancer increases the patient burden. Treatment toxicity, which is more likely in metastatic cancer patients with reduced functional status, limits the efficacy of treatment.2829 In our study, the greater proportion of special rehabilitation among distant-stage patients illustrated the severe disability associated with such cancer, compared with localised or regional disease. More complicated impairment in the case of distant-stage cancer requires special and intensive rehabilitation therapy that considers the safety and efficacy of appropriate and personalised therapy. Medical costs associated with emergency room visits and hospitalisation, as well as the caregiver burden, were higher in metastatic cancer patients; these costs could be reduced by such rehabilitation therapy. Compared to our previous study30 which reported that 29.9% of advanced cancer patients have a disability, the proportion of rehabilitation utilisation rate (8.7%) in patients with metastasis is far lower. Although those with primary tumours of the CNS and bone used rehabilitation therapy even in advanced stages of disease, fewer than 6% of the others (who might be severely disabled by distant metastasis) used this therapy. In addition, patients with advanced primary tumours of the pancreas, gastrointestinal tract, or respiratory organs (such as the lungs) rarely used rehabilitation therapy. The main cause of disability in such patients is not neuro-musculoskeletal in nature; rather, it is symptom clusters (pain, fatigue, and cachexia). Rehabilitation of cachexia is not covered by the Korean insurance system which could explain the discrepancy between the severity of impairment and less prevalent usage of rehabilitation for the advanced cancer patients with the primary cancer type of gastrointestinal tract. More evidence of the effectiveness of rehabilitation is required and the insurance system must be improved. Moreover, rehabilitation of cachexia and symptom clusters is required for advanced cancer patients.
Our study had several strengths. It was the first to analyse high-quality, population-based Korean cancer registry data, allowing rehabilitation utilisation to be understood according to the characteristics of a nationally representative population of cancer patients. Furthermore, the cancer type and stage were defined based on the KCCR data, rather than through analysis of medical claim records. One limitation of this study was that we could not determine the demand for rehabilitation by cancer patients, because these data were lacking. However, based on previous studies, the disability level could be estimated according to cancer type and stage. Secondly, there may have been some mismatches among procedures, benefits, and claim records. Further studies should examine patients' experience with, and the demand for, cancer rehabilitation. Movsas et al.26 reported that 87% of patients admitted to an oncology unit required rehabilitation. Further studies should determine the rate of unmet rehabilitation need among cancer patients.
In conclusion, only a small proportion of the cancer patients in this study received rehabilitation therapy. Cancer patients other than those with brain or bone tumours, which were previously covered by the insurance system, are less likely to utilise rehabilitation services. To overcome the underutilisation of cancer rehabilitation therapy in Korea, insurance coverage should be changed from a disease-oriented model to one based on internationally recognised classifications of functioning, disability, and health. Further efforts to improve the rate of rehabilitation treatment will be important for improving the outcomes of cancer patients.
 XML Download
XML Download