

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic hepatitis C virus (HCV) infection is a chronic inflammatory disease of the liver caused by HCV, and approximately 180 million individuals worldwide are infected.1 After acute HCV infection, 50–80% of patients transition to chronic hepatitis, which is a major cause of liver-related mortality. In Korea, the anti-HCV antibody positivity rate is 0.6–0.8%, of which 1/2–1/3 are accompanied by viremia.2 Also, HCV infection has been designed as a group 3 nationally notifiable infectious disease, and the number of reported cases is increasing every year.3
Human immunodeficiency virus (HIV) is an RNA virus that affects the immune system by acting on CD4+ T-cells. It is mainly transmitted through sexual intercourse, blood contact, or perinatal infection and progresses to acquired immune deficiency syndrome (CD4+ T-cell level: < 200 u/L) approximately 8–10 years after infection. Approximately 38 million individuals worldwide are infected with HIV and global prevalence is 0.7% in 2019.4 The number of individuals infected is still gradually increasing.5 The number of HIV-infected patients in Korea has increased steadily since it was first reported in 1985.6 However, the incidence of HIV infection in Korea is 2 per 100,000 individuals, the lowest among Organization for Economic Cooperation and Development countries after Japan.7
Both HCV and HIV infections are characterized by the same route of infection, even though there are differences in infectivity or prevalence rates by region. Globally, there are 4–5 million patients with HCV/HIV coinfection. The prevalence of HCV infection in patients with HIV infection varies from 2.5% to 82%, depending on the route of infection. In Korea, the HCV prevalence in HIV infected patients assessed by HCV Ab test was 1.7–5.2%.8 HCV/HIV coinfection progresses more rapidly to advanced liver fibrosis and cirrhosis than does HCV monoinfection, which eventually increases the risk of end-stage liver disease and hepatocellular carcinoma, resulting in higher liver-related mortality.910 It increases the relative risk of end-stage liver disease by 6.14 times and cirrhosis by 2.07 times.11
With the development of new oral direct-acting antivirals (DAAs) for the treatment of chronic HCV infection, the cure rate has been reported to reach almost 100% depending on the drug used. However, data related to the effect of HCV/HIV coinfection are limited. Several studies on the effect and stability of DAAs on HCV/HIV coinfection have been conducted, and it was reported that similar treatment response rates were obtained between HCV/HIV coinfection and HCV monoinfection.12131415 These studies suggested that DAA treatment is also effective in patients with HCV/HIV coinfection. However, there are very few studies on patients with HCV/HIV coinfection in low endemic areas of HIV infection, such as Korea. In Korea, previous studies on HCV/HIV coinfection did not reflect the actual clinical characteristics of patients with HCV/HIV coinfection because they defined HCV infection as positivity for anti-HCV antibody, not positivity of HCV-RNA polymerase chain reaction results.16 In addition, there are no studies on the efficacy of antiviral agents in HCV/HIV-coinfected patients. The aim of this study was to investigate the clinical characteristics of patients with HCV/HIV coinfection in Korea in comparison to those of patients with HCV monoinfection and to analyze the therapeutic effect of antiviral agents. We intended to provide a basis for selecting an appropriate therapeutic agent for HCV/HIV coinfection in Korea.
Go to : 
METHODS
Patient selection
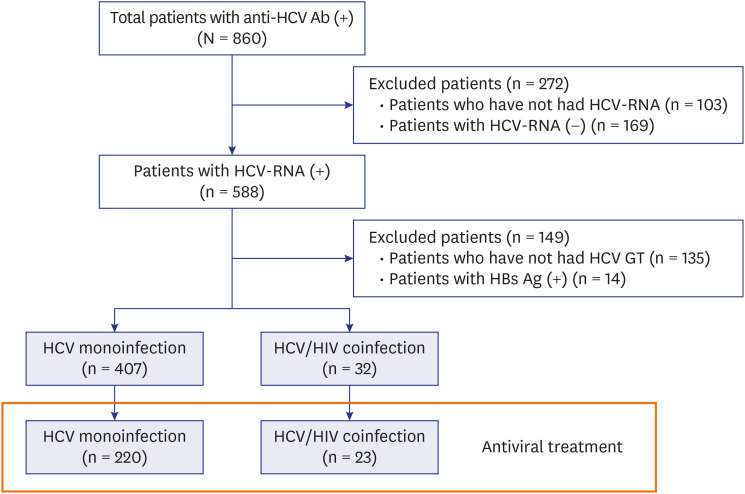
We retrospectively included 860 patients who had a positive result for anti-HCV antibody at the National Medical Center (NMC) in Seoul, Korea between January 2009 and March 2020. NMC is the central infectious diseases hospital in Korea, and in 2019, about 2,000 people with HIV infection were followed up. HCV infection was defined on the basis of a positive result for HCV-RNA polymerase chain reaction and known HIV-infected patients were included, for HIV infection is confirmed by national reference laboratories according to the law in Korea. The exclusion criteria were as follows: 1) age of < 19 years, 2) no HCV-RNA polymerase chain reaction data, 3) negative test result for HCV-RNA polymerase chain reaction, 4) no HCV genotype polymerase chain reaction data, and 5) concomitant infection with other chronic viral hepatitis, such as hepatitis B. Finally, 439 patients were enrolled in the analysis. A total of 243 patients were administered antiviral agents: 220 patients with HCV monoinfection and 23 patients with HCV/HIV coinfection (Fig. 1).
Clinical parameters
We collected the following clinical and laboratory data from electronic medical records: age, sex, nationality, HCV-RNA titer, HCV genotype, platelet count, aspartate transaminase (AST) level, alanine transaminase (ALT) level, history of anti-HCV treatment, type and duration of antiviral therapy, and rate of sustained viral response (SVR). Additionally, CD4+ T-lymphocyte count, HIV-RNA titer and duration of antiretroviral therapy were obtained in patients of HIV infection. The findings of the most recent test within 2 months of starting antiviral treatment were obtained as laboratory data. The HCV genotyping was performed by real-time polymerase chain reaction method. It targets the NS5B region and undergoes nucleic acid amplification and electrophoresis. HIV-RNA suppression defined as HIV-RNA < 40 copies/mm3. In addition, the AST level to platelet ratio index (APRI) and fibrosis-4 index (FIB-4 index) were calculated:
Cirrhosis was defined on the basis of histological or clinical, laboratory, and/or imaging features compatible with cirrhosis. Treatment regimens were selected by the physician according to the guidelines of the Korean Association for the Study of the Liver (KASL).1718 Chronic HCV infection in Korea was mainly treated with interferon-based treatment prior to the launch of daclatasvir and asunaprevir in 2015. Since then, it has mainly been treated with DAA therapy. Treatment efficacy was defined as the achievement of SVR (defined as HCV-RNA level of < 15 IU/mL) at 24 weeks after completion of treatment in patients receiving pegylated interferon-based treatment and 12 weeks after completion of treatment in patients receiving DAA treatment. Treatment failure was defined as the non-achievement of SVR, i.e., detectable serum HCV-RNA 12 weeks after treatment completion for DAA therapy and 24 weeks for pegylated interferon-based therapy. The treatment regimens used were pegylated interferon + ribarivin (PEG-INF + RBV), pegylated interferon + sofosbuvir + ribarivin (PEG-INF + SOF + RBV), daclatasvir + asunaprevir (DCV + ASV), sofosbuvir + ribavirin (SOF + RBV), ledipasvir/sofosbuvir (LDV/SOF), ledipasvir/sofosbuvir + ribavirin (LDV/SOF + RBV), grazoprevir/elbasvir (GZR/EBR), ombitasvir/paritaprevir/ritonavir + dasabuvir (OBV/PTV/r + DSV), sofosbuvir + daclatasvir (SOF + DCV), and glecaprevir/pibrentasvir (GLE/PIB) (Fig. 2). The duration from HCV diagnosis to treatment defined the period from the date of positive HCV-RNA test after first visit to the date of initiation of antiviral treatment. The primary endpoint was the comparison of SVR between HCV monoinfection and HCV/HIV coinfection. The secondary endpoint was the comparison of the clinical characteristics between them.
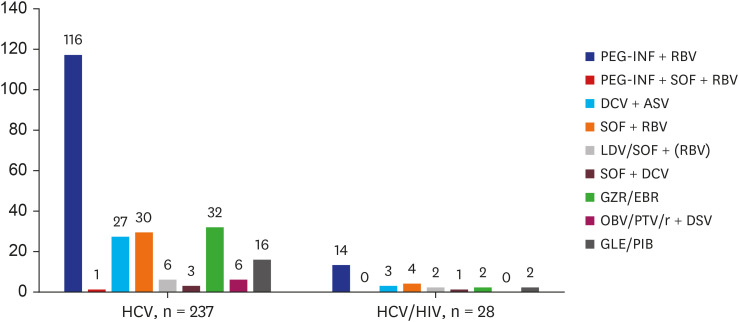 | Fig. 2Antiviral treatment regimens according to the study groups.HCV = hepatitis C virus, HIV = human immunodeficiency virus, PEG-INF = pegylated interferon-α, RBV = ribavirin, DCV = daclatasvir, ASV = asunaprevir, SOF = sofosbuvir, LDV = ledipasvir, GZR/EBR = grazoprevir/elbasvir, OBV/PTV/r = ombitasvir/paritaprevir/ritonavir, DSV = dasabuvir, GLE/PIB = glecaprevir/pibrentasvir.
|
Statistical analysis
The baseline characteristics were compared between HCV monoinfection and HCV/HIV coinfection using the independent t-test or Wilcoxon rank sum test for continuous variables and the Pearson χ2 test or Fisher's exact test for categorical variables. Statistical significance was set at P values of < 0.05. A univariate analysis was used to assess the factors related to SVR. Multivariate logistic regression was performed only for variables with P values of < 0.05 in the univariate analysis. Treatment efficacy was analyzed on an intent-to-treat (ITT) basis and a modified intent-to-treat (mITT) basis. In the ITT analysis, missing SVR measurements were assigned to indicate treatment failure. The mITT analysis included only patients with known SVR status. All statistical analyses were performed using commercially available statistical software (SPSS statistics version 26.0; IBM Corp., Armonk, NY, USA).
Ethics statement
This study was performed in accordance with the ethical guidelines of the Declaration of Helsinki. The present study protocol was reviewed and approved by Institutional Review Board of National Medical Center (NMC-2012-102). Informed consent was waived by the board.
Go to :
RESULTS
Baseline characteristics
Between January 2009 and March 2020, 860 patients were included in the study. Of these, 421 patients were excluded, and 439 patients were finally enrolled in the analysis. A total of 407 patients (92.7%) had HCV monoinfection, and 32 patients (7.3%) had HCV/HIV coinfection. Two hundred seventy-three patients were men (62.2%), and most of them had genotypes 1b (53.8%, n = 236) and 2 (40.3%, n = 177). However, the patients with HCV/HIV coinfection had a higher proportion of men than those with HCV monoinfection (93.8% vs 59.7%, P < 0.001). Also, HCV/HIV-coinfected patients had a higher incidence of genotype 1a, but a lower incidence of genotype 1b (Table 1).
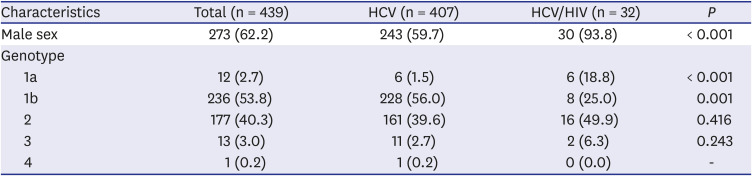
Table 1
Characteristics of the patients with positive HCV-RNA findings
Values are presented as number of patients (%).
HCV = hepatitis C virus, HIV = human immunodeficiency virus.
![]()
The baseline characteristics of the 243 patients who received antiviral treatment are shown in Table 2. Of them, 141 patients were men (58.0%), and the overall mean age was 55.7 ± 12.2 years. Genotype 1b was the most common genotype (50.6%), followed by genotype 2 (42.8%). Patients with cirrhosis were 20.2% and the mean HCV-RNA titer was 3,100,000 ± 5,900,000 IU/mL. In HCV/HIV-infected patients, the median CD4+ T-lymphocyte at the time of HCV antiviral treatment was 502 cell/mm3 (interquartile range, 338–671 cell/mm3) and HIV-RNA suppression was observed in 17 patients. Median duration of antiretroviral therapy was 10.2 months (interquartile range, 1.2–39.8 months). The most common route of infection was men who have sex with men in 8 patients (34.8%), followed by heterosexual transmission in 2 patients (8.7%). The route of infection of 13 patients has not been identified.
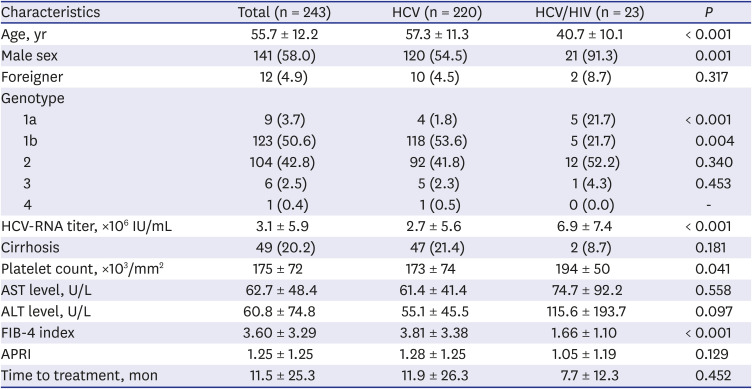
Table 2
Characteristics of the patients receiving antiviral therapy
Values are presented as mean ± standard deviation or number of patients (%).
HCV = hepatitis C virus, HIV = human immunodeficiency virus, AST = aspartate aminotransferase, ALT = alanine aminotransferase, FIB-4 = fibrosis-4, APRI = AST level to platelet ratio index.
![]()
Of the 243 patients, 220 patients with HCV monoinfection and 23 patients with HCV/HIV coinfection were treated with antiviral agents. The patients with HCV/HIV coinfection were significantly younger (40.7 ± 10.1 vs. 57.3 ± 11.3 years, P < 0.001) and more likely to be men (91.3% vs. 54.5%, P = 0.001). In terms of HCV genotype, though genotype 1b and 2 were most common in both HCV monoinfection and HCV/HIV coinfection groups, genotype 1a was more common in the HCV/HIV coinfection group (21.7% vs. 1.8%, P < 0.001); meanwhile, genotype 1b was more common in the HCV monoinfection group (53.6% vs. 21.7%, P = 0.004). The pretreatment HCV viral load was higher in the HCV/HIV coinfection group than in the HCV monoinfection group (6,900,000 ± 7,400,000 IU/mL vs. 2,700,000 ± 5,600,000 IU/mL, P < 0.001). The serum platelet count was higher in the HCV/HIV coinfection group (194 ± 50 vs. 173 ± 74 [×103/mm2], P = 0.041). However, the serum AST and ALT levels were not significantly different between the two groups. The patients with HCV/HIV coinfection had a lower FIB-4 index than those with HCV monoinfection (1.66 ± 1.10 vs. 3.81 ± 3.38, P < 0.001). Meanwhile, the APRI showed no difference between the two groups. The duration from HCV diagnosis to treatment in HCV monoinfection group and HCV/HIV coinfection group were 11.9 ± 26.3 and 7.7 ± 12.3 months, respectively (P = 0.452) (Table 2).
Among the patients receiving antiviral treatment, a total of 12 patients were foreigners. Ten patients had HCV monoinfection and 2 patients had HCV/HIV coinfection. Especially, all patients with genotype 3 (5 patients in HCV monoinfection and 1 patient in HCV/HIV coinfection) were foreigners. Also, in the rest of the foreign patients, 1, 4, and 1 patients had genotype 1a, 1b, and 2, respectively. When comparing the genotypes between Koreans and foreigners, 1b and 2 were more common in Koreans (96.1% [n = 222] vs. 41.7% [n = 5], P < 0.001).
Treatment outcomes
The treatment regimens according to the groups are summarized in Fig. 2. In our center, 22 patients received retreatment after the first antiviral treatment failure. Six patients had treatment experience in other hospitals. Thus, 265 antiviral treatments were administered. The number of patients receiving antiviral agents was similar between pegylated interferon-based treatment (n = 130, 49.1%) and DAA treatment (n = 135, 50.9%). There were 237 treatment-naïve patients and 28 treatment-experienced patients. There were 42 patients (15.8%) who had no confirmed SVR, and there was no significant difference between HCV monoinfection (n = 39, 16.5%) and HCV/HIV coinfection (n = 3, 10.7%) (P = 0.558).
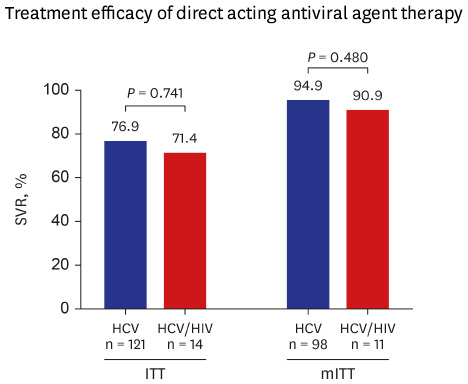
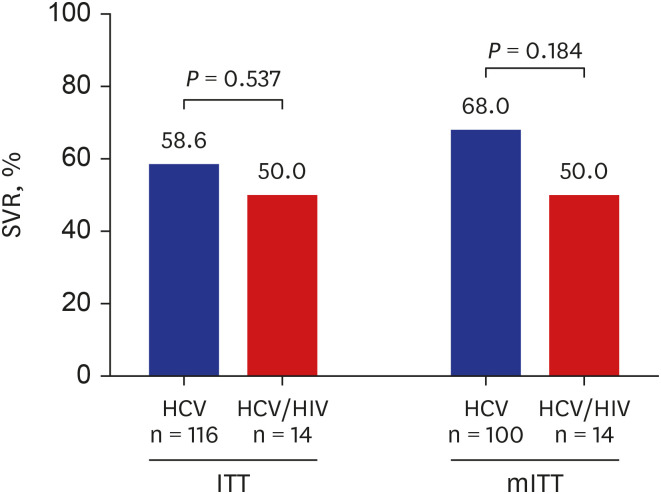
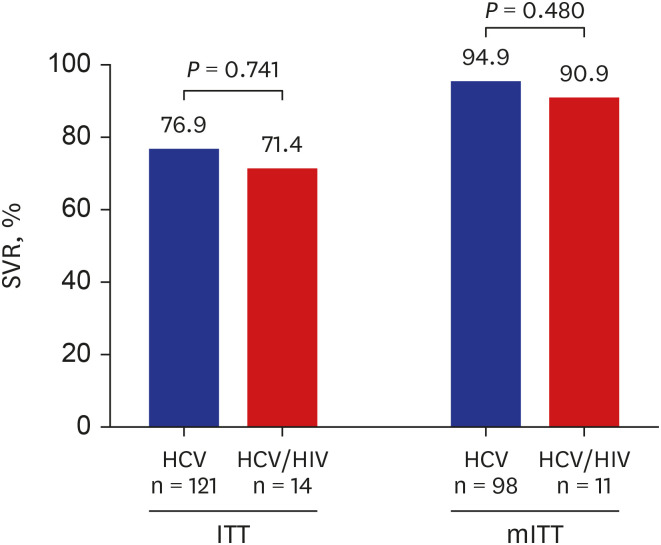
We compared the SVR rates between pegylated interferon-based treatment and DAA treatment. In the ITT analysis of the patients receiving pegylated interferon-based treatment, the SVR rate was 58.6% for HCV monoinfection and 50.0% for HCV/HIV coinfection, which was not significantly different (P = 0.537). In the analysis of the patients receiving DAA treatment, there was also no significant difference in the SVR rate between the two groups (76.9% vs. 71.4%, P = 0.741). In the mITT analysis, the treatment efficacy of pegylated interferon-based therapy for HCV monoinfection tended to be greater than that for HCV/HIV coinfection; however, the difference was not significant (68.0% vs. 50.0%, P = 0.184). In the comparison of the efficacy of DAA treatment in the mITT analysis, the SVR rate for HCV/HIV coinfection (90.9%) was as high as that for HCV monoinfection (94.9%) (Figs. 3 and 4).
Factors influencing the response to antiviral treatment
We evaluated the factors influencing the effectiveness of antiviral treatment, including interferon-based therapy and DAA therapy. In the univariate analysis, the HCV-RNA titer and DAA treatment were found to be associated with SVR. In the multivariate analysis adjusted for age and sex, a lower HCV-RNA titer and DAA treatment were independent factors for achieving SVR (hazard ratio [HR], 0.612; 95% confidence interval [CI], 0.409–0.914; P = 0.016 and HR, 8.806; 95% CI, 3.522–22.019; P < 0.001, respectively) (Table 3). Among 109 patients who received DAA treatment and with confirmed SVR, five patients failed to achieve SVR (one patient with HCV/HIV coinfection and four patients with HCV monoinfection). The characteristics of the patients with failed treatment are summarized in Table 4.
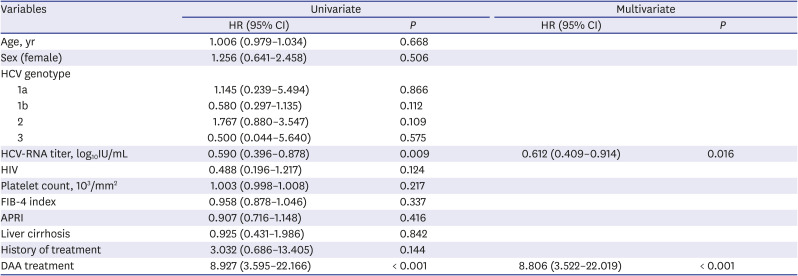

Table 3
Factors influencing SVR in the overall patients with chronic hepatitis C (modified intent-to-treat analysis)
HCV = hepatitis C virus, HIV = human immunodeficiency virus, FIB-4 = fibrosis-4, APRI = AST level to platelet ratio index, DAA = direct-acting antiviral, SVR = sustained viral response, HR = hazard ratio, CI = confidence interval.
![]()
Table 4
Characteristics of the patients treated with DAAs but failed to achieve SVR
HCV = hepatitis C virus, HIV = human immunodeficiency virus, DAA = direct-acting antiviral, LC = liver cirrhosis, SVR = sustained viral response, GT = genotype, DCV = daclatasvir, ASV = asunaprevir, SOF = sofosbuvir, RBV = ribavirin, GLE/PIB = glecaprevir/pibrentasvir, PEG-INF = pegylated interferon.
![]()
Go to :
DISCUSSION
Because of the low incidence of HIV infection in Korea, limited data are available regarding the treatment outcomes of patients with HCV/HIV coinfection. This is the first study to compare the clinical characteristics and treatment efficacy of HCV/HIV-coinfected patients with those of HCV-monoinfected patients in Korea. In this study, the SVR rate of DAA treatment in the HCV/HIV-coinfected patients was comparable to that in the HCV-monoinfected patients. This study showed that DAA treatment yielded therapeutic results in Koreans similar to those in previous study populations.
HCV/HIV coinfection yields more severe liver injury than does HCV monoinfection and is associated with an increased risk of end-stage liver disease or hepatocellular carcinoma.91019 Therefore, HCV eradication is important in patients with HCV/HIV coinfection. In the era of interferon-based treatment, patients with HCV/HIV coinfection achieve a lower therapeutic effect than do patients with HCV monoinfection, with a lower rate of achieving SVR.2021 After the development of DAAs, the paradigm for the treatment of HCV infection has changed. DAAs have been shown to have excellent cure rates for HCV monoinfection. Clinical trials evaluating the treatment efficacy of DAAs in patients with HCV/HIV coinfection showed efficacy similar to that in patients with HCV monoinfection.1314 Similar results were also reported in clinical studies conducted in actual clinical settings.2223 Collins et al.24 performed a retrospective cohort study of HCV-monoinfected and HCV/HIV-coinfected patients regarding treatment uptake and outcome of DAAs. The SVR rate was comparable between the two groups (90.9% vs. 96.7%, P = 0.074). Piekarska et al.25 evaluated the actual-clinical-setting efficacy of DAAs in patients with HCV/HIV coinfection as compared to that in patients with HCV monoinfection. The rates of SVR after 12 weeks did not differ significantly between the two groups (95.9% vs. 97.3% in the coinfection and monoinfection groups, respectively; P > 0.05). In our study, the analysis demonstrated comparable efficacy between the two groups. Both groups achieved SVR at a similar level, and there was no significant difference observed. This result is consistent with those of previous studies.
Genotype 1a was more common in the HCV/HIV-coinfected patients than in the HCV-monoinfected patients. This result is different from the fact that most of the genotypes in Korea are types 1b and 2. In one study in Korea that analyzed the genotype of 21 HCV/HIV-coinfected patients, 68.4% presented genotype 1, and the remaining patients presented genotype 2. They reported only genotypes 1b and 2 were observed in the HCV/HIV-coinfected group.8 Even considering nationality, the proportion of genotype 1a is higher in patients with HCV/HIV coinfection in our study. The reason why the distribution of genotypes is different from that in the other study is unclear. It is speculated that the patients in our study may have been infected through contact with foreigners, such as those from the USA, where genotype 1a is common. However, there is insufficient evidence to support this hypothesis. Additional multicenter studies will be needed to confirm the actual genotype distribution in HCV/HIV-coinfected patients.
Among the patients receiving antiviral therapy, the HCV-RNA titer was significantly higher in the HCV/HIV coinfected group. This indicates that viral replication occurred more actively in the patients with coinfection. There were no significant differences found for cirrhosis between the two groups. In terms of the serum fibrosis markers, the APRI did not show any significant differences. However, it is peculiar that the fibrosis-4 index was lower in the coinfected group. This is presumed to be because the HCV/HIV-coinfected patients were younger than the HCV-monoinfected patients. Further studies are required to determine the effect of coinfection on liver fibrosis. In the logistic regression analysis, the factors affecting SVR were the pretreatment HCV-RNA titer and DAA treatment. In particular, DAA treatment was associated with a nearly 9-fold increased likelihood of SVR. The treatment efficacy analysis showed that DAAs were effective in both groups irrespective of HIV infection.
Our study had several limitations. First, this was a single-center study and was retrospective in nature. Second, because of the small number of patients with HCV/HIV coinfection, we could not demonstrate a significant difference in the SVR rate between those with and without HIV infection. In addition, we could not analyze the predictors of SVR according to the treatment regimen. Third, as the study was conducted only on patients who visited public medical institutions, there was a possibility of selection bias. Further multicenter and nationwide studies are required to confirm this hypothesis.
In conclusion, this study showed that the patients with HCV/HIV coinfection who received antiviral treatment at a single center in Korea were younger, had higher proportion of men and incidence of genotype 1a, and had less advanced fibrosis than those with HCV monoinfection. Since it is conducted in a single center and had retrospective nature, there are limitations in interpretation and generalization. Nevertheless, in actual clinical settings, HCV/HIV-coinfected patients show an excellent treatment response to DAA treatment, similar with HCV-monoinfected patients.
Go to :
 XML Download
XML Download