

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic diseases have been shown to be caused by a variety of factors including genetics, lifestyle behaviors, and social determinants of health [1]. While the contributors of chronic disease are expansive, medical nutrition therapy (MNT) by registered dietitian nutritionists (RDNs) has been shown to be effective at preventing, delaying, and managing chronic diseases [23]. This includes chronic diseases such as diabetes, hypertension, lipid metabolism disorders, and chronic kidney disease [4]. MNT is an intensive, focused, and comprehensive nutrition therapy service involving in-depth individualized nutrition assessment [5]. Personalized goals, lifestyle changes, and interventions are established relative to each individual's nutrition challenges and medical condition(s) or disease(s) [5]. Ongoing behavior change is supported through reinforcement from follow-up [5]. MNT can address chronic disease through lifestyle modification as well as the impacts of social determinants of health on the individual's disease state [6].
RDNs can help facilitate lifestyle behavior changes by involving the patient in shared decision making, a unique and individualized approach to care. Some strategies using MNT include goal setting, assessing visual and social cues, stress management and more [789]. Specific dietary behavior lifestyle modifications are shown to improve as a result of nutrition counseling (e.g., increased fruit and vegetable intake [10], weight loss [11], reduced waist circumference (WC) [11], improved blood pressure). Physical activity is another lifestyle modification that RDNs play a key role in addressing. Physical activity related lifestyle modification facilitated by RDNs is shown to prevent weight and body fat regain following loss [12].
In addition to facilitating lifestyle behaviors for the management of chronic disease, understanding patients' social determinants of health also contribute to an improved health status. Food insecurity and poor food access are linked with higher levels of chronic disease [1314]. Additionally, poor disease self-management [1516], increased hospitalization [16], and a higher probability of mental health issues [17] are linked with food insecurity. Food insecurity is defined as “a household-level economic and social condition of limited or uncertain access to adequate food” [18]. The Academy of Nutrition and Dietetics has highlighted the important role that RDNs play in addressing food insecurity [19]. RDNs who assess social determinants of health during visits can help identify concerns, like food insecurity, and work to help patients with resources and referrals needed to improve health outcomes. While the effectiveness of MNT by RDNs on chronic disease through lifestyle modification is clear, little research exists to explore the effects of MNT by RDNs on food security.
MNT is an evidence-based solution for preventing and managing chronic disease. A large body of research exists demonstrating the effectiveness of RDNs in the primary care setting [20]. One less frequently studied setting is the patient’s home. The home environment has been identified as an area for skill-building and education interventions for availability and accessibility of food [2122]. The home environment has been studied in relation to children and obesity [23]. However, less studied is the home environment's impact on the adult population where the same intervention benefits may be observed [242526]. The home environment offers a unique setting to provide MNT, as the RDN is provided with a broader representation of contributing factors related to potential health disparities. Therefore, the purpose of this secondary data analysis was to assess the impact of individualized MNT by RDNs in the home setting on dietary factors, physical activity, and food security. We hypothesized that RDNs have positive impacts on dietary factors, physical activity, and food security status.
SUBJECTS AND MATERIALS
Study design
This secondary data analysis used baseline and follow up data from a nutrition consulting company in Philadelphia, Pennsylvania. This data was collected within the regional area of Philadelphia.
Participants
Eligible participants (n = 1,007) were selected based on a convenience sample of individuals referred by healthcare professionals or self-referred. Additionally, participants had an MNT benefit covered by their health insurance plan. Participants partook in one-on-one nutritional counseling with a RDN in the participant's home. Total individual visits ranged from one or more, depending on participant's wants, between January 1, 2019 and December 31, 2019.
The original intention for data collection was not research, thus participants did not complete an informed consent. De-identified data was provided to the research team for analysis. The University of North Florida Institutional Review Board deemed this research not human subjects research (UNF IRB: 1437719).
Procedures
Nutrition assessment and intervention were completed during a home visit by a trained Registered Dietitian Nutritionist. Each nutrition intervention approach was individualized based on the wants and needs of each participant. RDNs used personalized MNT to enhance the participants nutritional status. Other counseling strategies employed included motivational interviewing and SMART goal setting.
Measurements
Each participant provided baseline demographics (age, sex, insurance company). Anthropometric data (e.g., height, weight) were self-reported, body mass index (BMI) was then calculated. Participants provided self-reported dietary intake using Food Patterns Equivalents Database standard questions of servings per day of each group (whole grains, fruit, vegetables, dairy, fish, and water) [27]. Physical activity status (e.g., days per week, minutes per day) was self-reported. The 2-item food security screener questionnaire, based on the United States Department of Agriculture (USDA) Food Security Survey, was asked verbally by RDNs during home visits [28].
Data analysis
Summary and statistical analyses were performed on all data using SAS® software version 9.4 (SAS Institute, Cary, NC, USA) [29]. All statistical tests were two-sided, with 5% significance level (P < 0.05 was considered significant). To address the potential data entry errors and exclude unreasonable outliers, the data analysis only included the subjects who are at least 18 years old and with no more than six home visits.
The changes (post value − pre value) of the corresponding categories (weight, BMI, physical activity, and dietary factors) were analyzed by a linear regression model or linear mixed model, depending on the model fit. Age, sex, baseline (pre) value, and number of appointments were included in all models as fixed effect. The RDN was included in the model for weight and BMI change as a random intercept. The correlated residuals among the different types of dietary factors were accounted for by the appropriate covariance structure. Furthermore, for all the response variables, the observations within the 5th to 95th percentile were included for the robustness of the testing.
RESULTS
Participants
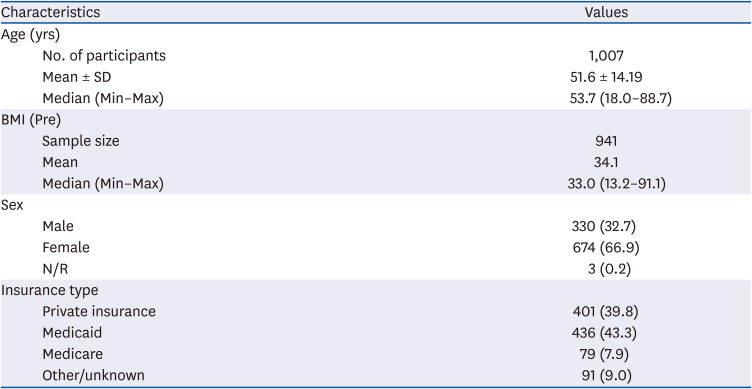
Table 1 summarizes the demographics of the participants. The average age of the participants was 51.6 years old with a mean BMI of 34.1 kg/m2. Participants insurance type varied, with a majority holding Medicaid (43.3%) and then private insurance (39.8%).
Table 1
Demographics of participants
Weight, BMI, and physical activity
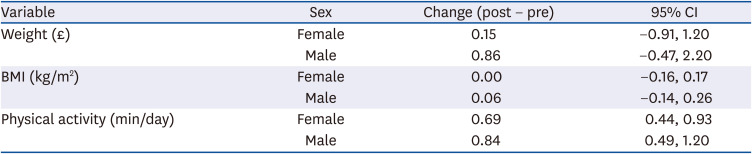
Table 2 summarizes the findings from the analysis of changes in weight, BMI, and physical activities by sex. The baseline value was a significant factor for all changes, while the number of appointments was significant for the changes in weight and BMI. On average, weight increased by 0.15 pounds for female participants and 0.86 pounds for male participants. BMI did not change for female participants and increased by 0.06 for male participants. Weight and BMI change were not significant. For everyone more home visit, weight increased by 0.6 pounds and BMI increased by 0.08 pounds. Regarding time spent on physical activity per day, increases were significant for both female and male participants by 0.69 and 0.84, respectively. This equates to an additional 10.4 and 12.6 minutes per day of physical activity.
Table 2
Least squares-mean estimates of changes in weight, BMI and physical activity
Dietary factors
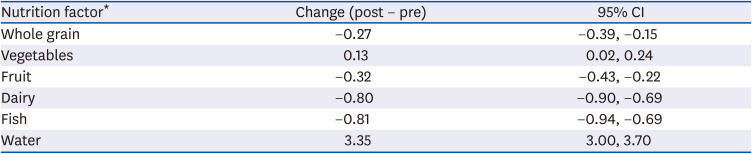
Table 3 summarizes the findings from the analysis for changes in dietary factors. The baseline value and the number of appointments were significant for the changes in dietary factors. For everyone more home visit, there is 0.04 increase in the number of total servings of all dietary changes. However, the disparity was remarkable between different types of dietary factors. For example, the consumption of total servings of vegetables (0.13) and water (3.35) significantly increased, while the consumption of total servings of whole grains (−0.27), fruits (−0.32), dairy (−0.80) and fish (−0.81) significantly decreased.
Food insecurity
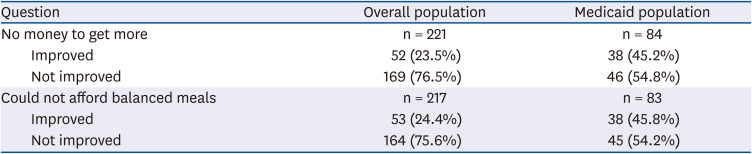
Two validated screening questions [28] regarding food security were asked during home visits using a 4-point scale in which a higher score represents a higher level of food insecurity. Improvement in food security was defined as a lower score at the end compared to the beginning of home visits. The proportions of improvement were examined and reported by the summary statistics. No formal analysis was conducted due to the limited sample size from a large amount of missing data.
In the overall population, 23.5% among the 221 participants showed improvement in answering the first question and 24.4% among the 217 participants showed improvement for the second question. The proportions in the Medicaid population were even higher: 45.2% (out of 84 participants) improved for the first question and 45.8% (out of 83 participants) improved for the second question (Table 4).
DISCUSSION
This secondary data analysis was one of the first in the past several decades to demonstrate the impact of RDNs delivering MNT in the home setting. Advantages of the RDN providing MNT has been demonstrated [20], however, research supporting the use of MNT in home settings has been limited. Therefore, this study sought to build on a much-needed area of RDN MNT research. The importance of the home environment as an ideal setting to provide MNT has been demonstrated in this study. This study found that RDNs in the home were able to impact dietary and lifestyle changes. The home environment MNT setting can be critical for applying individualized behavior change modifications due to understanding the unique characteristics of the participant's physical environment (e.g., housing, transportation, safety, walkability, geography). Moreover, home visits allow for RDNs to provide applicable resources (e.g., food access, resources, education, health access) tailored to an individual person's needs.
In this analysis, RDNs were able to initiate successful changes in self-reported physical activity, vegetable intake, and water intake. Weight remained relatively unchanged, with statistically insignificant increases reported. This is consistent with research showing long-term weight loss and maintenance is difficult, but with the right behavioral strategies and understanding of home characteristics, people can be successful [30]. Thus, it is positive that this analysis observed nonsignificant change. Weight in this context was self-reported and also might not have been the primary reason for seeing an RDN, which may be reasons for limited findings. Additionally, with the increases in vegetable and water intake but decreases in fruits, whole grains, dairy and fish, it should be noted that people tend to under and over-report depending on a variety of factors such as age, BMI, sex, life-stage, etc. [31]. This study asked dietary intake through a typical day of eating, for example, “how many servings of whole grains do you eat per day” which is then assessed across the number of visits per individual. These might fluctuate and not adequately capture dietary intake. Moreover, participants who signed up for home visits may have had different intentions (e.g., weight loss, improved health, fitness, wellness), thus it is difficult to draw single conclusions for the whole group on behavior change.
A particularly noteworthy finding was the reported change in food security with the overall population reporting 23.5% improvement with the first question and 24.4% improvement with the second question. When examining the subset Medicaid population, food security change increased to 45.2% improvement with the first question and 45.8% improvement with the second question. This shows RDNs are positioned to guide vulnerable populations toward solutions related to food insecurity. As outlined by the Academy of Nutrition and Dietetics position statement [19] on food security in the U.S., through home visits, RDNs in this setting can assess and monitor food security through the 2-item screener [28] and then provide referrals and resources during the home visit session based on responses and needs. Conducting visits in the home setting and familiarity with the communities in which participants live, RDNs can appropriately provide locations and hours of operation for the nearest food bank/food pantry, while understanding limitations surrounding food acquisition and transportation [19]. A study by Knoblock-Hahn and colleagues [32] also found improvements in food security with a program specifically geared at empowering parents to make improvements with health behavior decisions. As stated by the Academy of Nutrition and Dietetics practice applications president's page, “as dietitians, we may never know if our patient is food-insecure by looking at them” [33]. With RDNs in the home, as they were in this analysis, they are better situated and can observe the larger home environmental contextual evidence to understand the participant's food security risk. Even more less studied is the impact of home visits with nutrition assessment and monitoring on vulnerable populations, like Medicaid recipients. This analysis extends research in this area and creates groundwork for future research in the home environment with adults and the complexities associated with the Medicaid population.
This secondary analysis of data collected from a city-wide nutrition program provides several strengths including analyzing data conducted from home visits over a period of time. This analysis extends much needed research on adults in the home environment related to weight, BMI, and dietary intake, especially since capturing data on the varied roles and employment options by RDNs is needed. Another strength of the study is the evidence to support improvements in food security through home visits by RDNs, especially in the Medicaid population. This is critical as the U.S. continues to see high food security risk now coupled with the impact of coronavirus disease 2019. While this study has strengths, it is not without limitations including the nature of secondary analysis of data. Participants scheduled appointments for a variety of reasons, ultimately making it difficult to draw cohesive conclusions due to the personalized nature of the data. Data collected was not part of a research study and with that stated, there's methodological weaknesses including self-reported weight, physical activity, and dietary intake. Future work in this area should be structured as part of research study including consenting and enrolling interested participants from the population already participating in the program. A more research sound methodology may lend to more accurate measures of weight (e.g., RDN carrying and conducting weight/height measurements via a portable scale and stadiometer) and use of diet records or 24-h recalls, findings may be strengthened.
Registered Dietitian Nutritionists are uniquely fitted to provide MNT in the home setting. With using the home as the location of care delivery, RDNs can get a full picture of the environment and nearby resources surrounding the individual, thus providing personalized counseling. RDNs can improve dietary behaviors, boost physical activity, and provide resources needed to address food insecurity.
 XML Download
XML Download