

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cancer incidence and mortality rates are increasing rapidly worldwide [1]. The World Health Organization (WHO) reported that 1 in 6 people, a total of 9.6 million, died due to cancer in 2018, and that cancer is the second leading cause of death worldwide [2]. Among cancers, lung cancer (1.76 million deaths), colorectal cancer (862,000 deaths), stomach cancer (783,000 deaths), liver cancer (782,000 deaths), and breast cancer (627,000 deaths) caused the most deaths in 2018 [2]. It has been reported that one-third of cancer deaths are associated with dietary risks and behaviors, such as a high body mass index, a low fruit and vegetable intake, a lack of physical activity, tobacco use, and alcohol use [2]. These results indicate that dietary habits are critical to cancer prevention.
Garlic (Allium sativum L.) is a perennial plant belonging to the Liliaceae, and has been widely cultivated and used as traditional medicine and seasoning and food for thousands of years [3]. Garlic contains more than 33 organic sulfur compounds, in addition to amino acids, vitamins, and micronutrients [4]. The major allyl sulfur content in freshly crushed or chopped garlic is allicin, which is unstable and breaks down rapidly to produce odorous oil-soluble diallyl sulfide (DAS), diallyl disulfide (DADS), diallyl trisulfide (DATS), and ajoene. The major allyl sulfur constituents in processed garlic, S-allylcysteine (SAC) and S-allylmercaptocysteine, are water soluble and formed by the process of natural aging bioconversion [5].
Garlic and its bioactive constituents have been shown to have many properties in in vitro or in vivo studies: anticancer, antithrombotic, antioxidant, anti-inflammatory, antibacterial, antifungal, immunomodulatory, cardiovascular protective, hepatoprotective, digestive system protective, antidiabetic, antiobesity, neuroprotective, and renal protective [67]. Particularly, anticancer effects of garlic may affect cancer cells by modulation of many pathways including alteration in carcinogen-metabolizing enzymes, cell cycle arrest, and induction of apoptotic cell death and suppression of oncogenic signal transduction pathways [8910]. Although the beneficial effects of garlic intake against cancer have been reported in animal studies, benefits in human studies still remain controversial [11].
The Continuous Update Project (CUP) is the largest source of scientific evidence on cancer prevention of diet, weight, and exercise. The results from this CUP (2018) showed no conclusion was drawn due to very limited evidence supported a relation between garlic intake and risk of colorectal cancer [12]. Although there were a few systematic reviews conducted to investigate the effects of garlic intake on cancer, the researchers used a less reliable, and less valid assessment tool instead of the most commonly recommend tool, such as the Cochrane risk of bias tool for RCTs [48]. One meta-analysis of the epidemiological data on the association between garlic intake and cancer prevention did not include information on critical appraisal of study quality [13]. Another meta-analysis included only prospective cohort studies, but not RCTs [14]. Therefore, we aimed to conduct a systematic review to evaluate whether there is a causal relationship between garlic intake and cancer, following the rigorous methods outlined in the Cochrane handbook for systematic reviews including both RCTs and observational studies [15].
SUBJECTS AND METHODS
Data sources and searches
The searches for randomized controlled trials (RCTs) and observational studies, such as prospective cohort studies, related to cancer (surrogate and clinical outcome, including cancer-specific mortality) were performed in 3 databases: MEDLINE (from inception to July 1st week, 2018; search on July 17th, 2018), Embase (from inception to September 5th, 2018; search on September 5th, 2018), and Web of Science (from inception to September 5th, 2018; search on September 5th, 2018). No language restriction was added. The complete search strategy is presented in Supplementary Table 1. Moreover, other articles were identified from the previously published systematic reviews and added to our study [161718].
Study eligibility criteria
We included human intervention trials with a minimum duration of 4 weeks, as well as prospective observational studies (i.e., prospective cohort studies, nested case-control studies, and case-cohort studies). To be included, studies must have provided quantitative information on oral garlic intake from foods or dietary supplements. Studies not containing this quantitative information of garlic intake must have compared different doses of garlic intake (e.g., higher vs. lower doses) or compared the effect of garlic alone with that of a placebo or another active comparator. Finally, studies must have reported outcomes related to cancer, including all types of cancer incidence and mortality (i.e., a specific type of cancer, cancer-specific mortality, or surrogate of cancer risk).
Study selection process
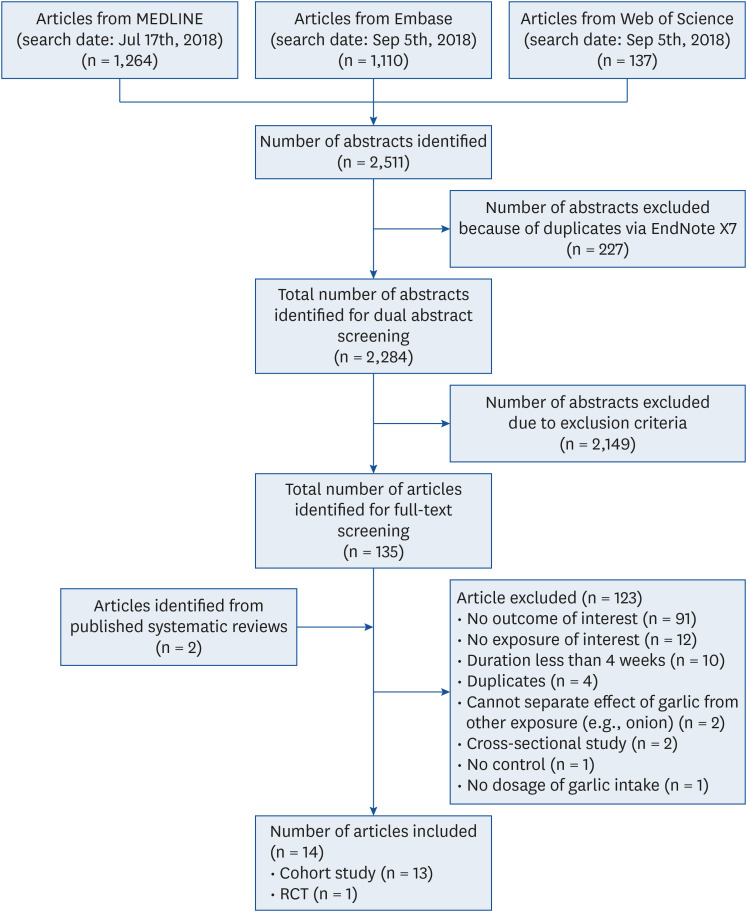
The abstract and titles of all citations were independently screened by 2 investigators according to the established criteria. The abstract screening was performed in the open-source, online software Abstrackr by 2 investigators separately [19]. The full-text screening was performed independently according to the eligibility criteria by 2 investigators. Conflicts were resolved by group consensus. The study selection process is summarized in Fig. 1. Although no language restrictions were applied during the literature search, this systematic review did not identify any foreign language studies.
Data extraction and study quality assessment
Two investigators independently extracted data (e.g., study characteristics, risk ratio) from each included study by using standardized data extraction forms. Discrepancies were resolved by discussion between the two investigators or further group discussion. To assess the risk of bias (RoB) for each included study, we used validated tools—the Newcastle-Ottawa Scale (NOS) for prospective cohort studies [20] and the Cochrane RoB tool for randomized controlled trials [21]. For this study, we modified the study quality assessment tool of the NOS taking out ‘Demonstration That Outcome of Interest Was Not Present at Start of Study’ and ‘Was Follow-Up Long Enough for Outcomes to Occur’ from the original NOS because all included prospective studies were rated `low risk’ for these two questions. Instead, we added ‘adequate sample size and power’ and ‘selective outcome reporting’ questions. Therefore, the modified NOS finally consisted of 8 evaluation items (Supplementary Table 2): (1) representativeness of the exposed cohort; (2) selection of the nonexposed cohort, (3) ascertainment of nutrient exposure, (4) control for important confounders, (5) adequate sample size and power, (6) outcome assessment, (7) completeness of cohort follow-up, and (8) selective outcome reporting. The Cochrane RoB tool consisted of 5 domains: (1) bias arising from the randomization process, (2) bias due to deviations from the intended intervention, (3) bias due to missing outcome data, (4) bias in the measurement of the outcome, and (5) bias in the selection of the reported result. Two investigators rated the RoB with 1 of 3 options: high, low, or unclear risk. Discrepancies were resolved by discussion between the 2 investigators.
Qualitative synthesis and data reporting
Due to large clinical heterogeneity, particularly the different types of garlic intake and various doses of garlic intake reported in the included studies, we performed a narrative synthesis instead of a meta-analysis. We reported our systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline [22]. We assessed the strength of evidence (SoE) for all outcomes by utilizing an evidence grading system employed by the American Diabetes Association (Supplementary Table 3) [23].
RESULTS
The initial search yielded 2,511 citations. Of these, we identified 2,284 unduplicated abstracts for dual abstract screening. Then, we screened 135 possibly relevant articles for full-text screening. Finally, we selected 14 articles (1 RCT and 13 cohort studies). Fig. 1 shows the flow chart of the study selection process. Tables 1 and 2 present the characteristics of the included RCTs and prospective observational studies (i.e., cohort and case-cohort studies), respectively. We present the results by the research questions, specifically the effects of garlic intake on colorectal cancer and other types of cancer. We summarized the findings of this RCT first, followed by the results of the prospective observational studies.


Table 1
Characteristics of the included RCT
| Author, Year [Reference] | Country | Male sex at enrollment (%) | Baseline age (yrs), mean ± SD | Baseline health status | Design/duration | Garlic group | Comparison group | Outcome | Adverse events | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size | Intervention | Sample size | Intervention | ||||||||
| Tanaka, 2006 [24] | Japan | 72.97% | High-AGE, 57.6 ± 1.3; Low-AGE, 61.3 ± 2.0 | Colorectal adenomas | 12 mon | 19 | 2.4 mL per capsule *3 capsules *2 times per day | 18 | 0.16 mL per capsule *3 capsules *2 times per day | Incidence of adenomas, number of adenomas and total size of adenomas | 1 had itchy back in high-AGE and 3 had eczema on the upper limbs, epigastric pain, and glossitis in low-AGE |
![]()
Table 2
Risk of bias assessment for the included RCTs
| Author, Year [Reference] | Bias arising from the randomization process | Bias due to deviations from the intended interventions | Bias due to missing outcome data | Bias in the measurement of the outcome | Bias in the selection of the reported results | Overall bias |
|---|---|---|---|---|---|---|
| Tanaka, 2006 [24] | Some concerns | Low | Low | Low | Low | Moderate (= some concerns) |
![]()
Garlic intake and colorectal cancer
RCTs
Only one RCT [24] met our inclusion criteria (Table 1). Participants (n = 51) with colorectal adenomas (i.e., precancerous lesions of the large bowel) were randomized to either high-dose aged garlic extract (AGE) (2.4 mL/day) or low-dose AGE (0.16 mL/day) for 12 mon. The number and size of colorectal adenomas were assessed via colonoscopy. Of the 51 participants, 37 patients completed the study (19 in the high-dose AGE group vs. 18 in the low-dose AGE group). The results of this RCT showed that high-dose AGE significantly suppressed both the number and total size of colorectal adenomas compared to low-dose AGE after 12 months of intervention (P < 0.05). The overall RoB of this RCT was graded as moderate because of some concerns regarding bias arising from the randomization process (Table 2).
Prospective observational studies
We included 7 prospective observational studies (6 cohort studies and 1 case-cohort study) [25262728293031] in the analysis of garlic intake and risk of colorectal cancer (Table 3). These studies included 3 studies [293031] of total colorectal cancer, 4 studies [25262728] of colon cancer, and 1 study each of rectal cancer [2728293031], proximal colon cancer [2631], and distal colon cancer [2631]. The majority of the included studies (6 of 7 studies) were prospective cohort studies conducted in the U.S., and only one case-cohort study was conducted in the Netherlands. The follow-up duration of the included studies ranged from 3.3 to 24 yrs. The types of garlic exposure were only garlic intake from food sources for 3 studies, only garlic supplements for 2 studies, and garlic from both food and supplements for 2 studies. Only male participants were included for 4 of the 7 studies. The number of participants ranged from 35,210 to 173,229 participants across the 6 prospective cohort studies. The overall RoB was graded as moderate for all 7 studies, specifically due to use of insufficient methods to estimate accurate and usual dietary intake (e.g., food frequency questionnaire or only a single 24 h) to ascertain garlic exposure and inadequate information for statistical power (Table 4).
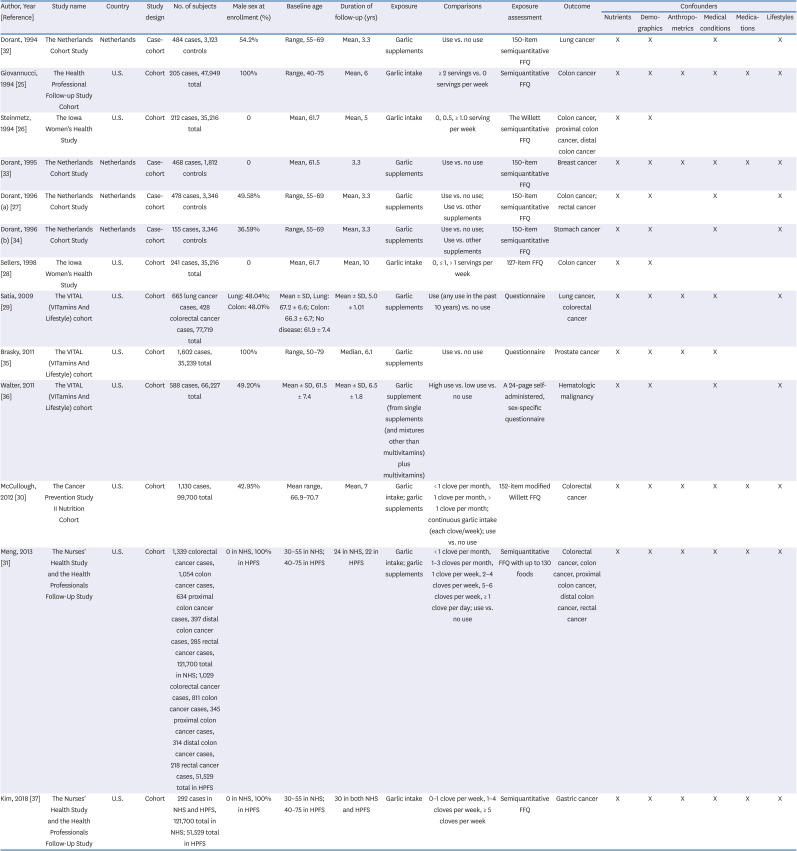
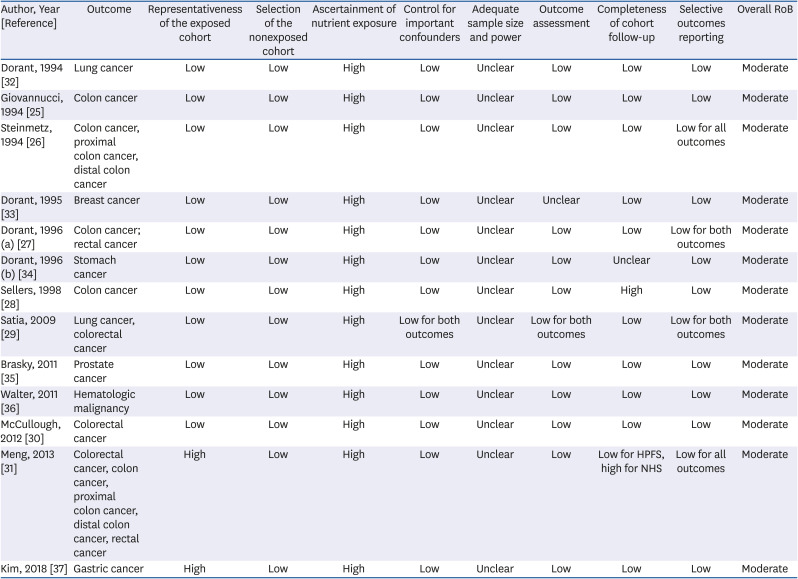
Table 3
Characteristics of the included cohort studies (n = 13)
| Author, Year [Reference] | Study name | Country | Study design | No. of subjects | Male sex at enrollment (%) | Baseline age | Duration of follow-up (yrs) | Exposure | Comparisons | Exposure assessment | Outcome | Confounders | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nutrients | Demographics | Anthropometrics | Medical conditions | Medications | Lifestyles | ||||||||||||
| Dorant, 1994 [32] | The Netherlands Cohort Study | Netherlands | Case-cohort | 484 cases, 3,123 controls | 54.2% | Range, 55–69 | Mean, 3.3 | Garlic supplements | Use vs. no use | 150-item semiquantitative FFQ | Lung cancer | X | X | X | X | ||
| Giovannucci, 1994 [25] | The Health Professional Follow-up Study Cohort | U.S. | Cohort | 205 cases, 47,949 total | 100% | Range, 40–75 | Mean, 6 | Garlic intake | ≥ 2 servings vs. 0 servings per week | Semiquantitative FFQ | Colon cancer | X | X | X | X | X | X |
| Steinmetz, 1994 [26] | The Iowa Women's Health Study | U.S. | Cohort | 212 cases, 35,216 total | 0 | Mean, 61.7 | Mean, 5 | Garlic intake | 0, 0.5, ≥ 1.0 serving per week | The Willett semiquantitative FFQ | Colon cancer, proximal colon cancer, distal colon cancer | X | X | ||||
| Dorant, 1995 [33] | The Netherlands Cohort Study | Netherlands | Case-cohort | 468 cases, 1,812 controls | 0 | Mean, 61.5 | 3.3 | Garlic supplements | Use vs. no use | 150-item semiquantitative FFQ | Breast cancer | X | X | X | X | X | X |
| Dorant, 1996 (a) [27] | The Netherlands Cohort Study | Netherlands | Case-cohort | 478 cases, 3,346 controls | 49.58% | Range, 55–69 | Mean, 3.3 | Garlic supplements | Use vs. no use; | 150-item semiquantitative FFQ | Colon cancer; rectal cancer | X | X | X | X | ||
| Use vs. other supplements | |||||||||||||||||
| Dorant, 1996 (b) [34] | The Netherlands Cohort Study | Netherlands | Case-cohort | 155 cases, 3,346 controls | 36.59% | Range, 55–69 | Mean, 3.3 | Garlic supplements | Use vs. no use; | 150-item semiquantitative FFQ | Stomach cancer | X | X | X | X | ||
| Use vs. other supplements | |||||||||||||||||
| Sellers, 1998 [28] | The Iowa Women's Health Study | U.S. | Cohort | 241 cases, 35,216 total | 0 | Mean, 61.7 | Mean, 10 | Garlic intake | 0, ≤ 1, > 1 servings per week | 127-item FFQ | Colon cancer | X | X | ||||
| Satia, 2009 [29] | The VITAL (VITamins And Lifestyle) cohort | U.S. | Cohort | 665 lung cancer cases, 428 colorectal cancer cases, 77,719 total | Lung: 48.04%; | Mean ± SD, Lung: 67.2 ± 6.6; Colon: 66.3 ± 6.7; No disease: 61.9 ± 7.4 | Mean ± SD, 5.0 ± 1.01 | Garlic supplements | Use (any use in the past 10 years) vs. no use | Questionnaire | Lung cancer, colorectal cancer | X | X | X | X | X | |
| Colon: 48.01% | |||||||||||||||||
| Brasky, 2011 [35] | The VITAL (VITamins And Lifestyle) cohort | U.S. | Cohort | 1,602 cases, 35,239 total | 100% | Range, 50–79 | Median, 6.1 | Garlic supplements | Use vs. no use | Questionnaire | Prostate cancer | X | X | X | X | ||
| Walter, 2011 [36] | The VITAL (VITamins And Lifestyle) cohort | U.S. | Cohort | 588 cases, 66,227 total | 49.20% | Mean ± SD, 61.5 ± 7.4 | Mean ± SD, 6.5 ± 1.8 | Garlic supplement (from single supplements (and mixtures other than multivitamins) plus multivitamins) | High use vs. low use vs. no use | A 24-page self-administered, sex-specific questionnaire | Hematologic malignancy | X | X | X | X | ||
| McCullough, 2012 [30] | The Cancer Prevention Study II Nutrition Cohort | U.S. | Cohort | 1,130 cases, 99,700 total | 42.95% | Mean range, 66.9–70.7 | Mean, 7 | Garlic intake; garlic supplements | < 1 clove per month, 1 clove per month, > 1 clove per month; continuous garlic intake (each clove/week); use vs. no use | 152-item modified Willett FFQ | Colorectal cancer | X | X | X | X | X | X |
| Meng, 2013 [31] | The Nurses' Health Study and the Health Professionals Follow-Up Study | U.S. | Cohort | 1,339 colorectal cancer cases, 1,054 colon cancer cases, 634 proximal colon cancer cases, 397 distal colon cancer cases, 285 rectal cancer cases, 121,700 total in NHS; 1,029 colorectal cancer cases, 811 colon cancer cases, 345 proximal colon cancer cases, 314 distal colon cancer cases, 218 rectal cancer cases, 51,529 total in HPFS | 0 in NHS, 100% in HPFS | 30–55 in NHS; 40–75 in HPFS | 24 in NHS, 22 in HPFS | Garlic intake; garlic supplements | < 1 clove per month, 1–3 cloves per month, 1 clove per week, 2–4 cloves per week, 5–6 cloves per week, ≥ 1 clove per day; use vs. no use | Semiquantitative FFQ with up to 130 foods | Colorectal cancer, colon cancer, proximal colon cancer, distal colon cancer, rectal cancer | X | X | X | X | X | X |
| Kim, 2018 [37] | The Nurses' Health Study and the Health Professionals Follow-Up Study | U.S. | Cohort | 292 cases in NHS and HPFS, 121,700 total in NHS; 51,529 total in HPFS | 0 in NHS, 100% in HPFS | 30–55 in NHS; 40–75 in HPFS | 30 in both NHS and HPFS | Garlic intake | 0–1 clove per week, 1–4 cloves per week, ≥ 5 cloves per week | Semiquantitative FFQ | Gastric cancer | X | X | X | X | X | X |
FFQ, food frequency questionnaire; NHS, Nurses' Health Study; HPFS, Health Professionals Follow-up Study.
![]()
Table 4
Risk of bias assessment for the included cohort studies (n = 13)
| Author, Year [Reference] | Outcome | Representativeness of the exposed cohort | Selection of the nonexposed cohort | Ascertainment of nutrient exposure | Control for important confounders | Adequate sample size and power | Outcome assessment | Completeness of cohort follow-up | Selective outcomes reporting | Overall RoB |
|---|---|---|---|---|---|---|---|---|---|---|
| Dorant, 1994 [32] | Lung cancer | Low | Low | High | Low | Unclear | Low | Low | Low | Moderate |
| Giovannucci, 1994 [25] | Colon cancer | Low | Low | High | Low | Unclear | Low | Low | Low | Moderate |
| Steinmetz, 1994 [26] | Colon cancer, proximal colon cancer, distal colon cancer | Low | Low | High | Low | Unclear | Low | Low | Low for all outcomes | Moderate |
| Dorant, 1995 [33] | Breast cancer | Low | Low | High | Low | Unclear | Unclear | Low | Low | Moderate |
| Dorant, 1996 (a) [27] | Colon cancer; rectal cancer | Low | Low | High | Low | Unclear | Low | Low | Low for both outcomes | Moderate |
| Dorant, 1996 (b) [34] | Stomach cancer | Low | Low | High | Low | Unclear | Low | Unclear | Low | Moderate |
| Sellers, 1998 [28] | Colon cancer | Low | Low | High | Low | Unclear | Low | High | Low | Moderate |
| Satia, 2009 [29] | Lung cancer, colorectal cancer | Low | Low | High | Low for both outcomes | Unclear | Low for both outcomes | Low | Low for both outcomes | Moderate |
| Brasky, 2011 [35] | Prostate cancer | Low | Low | High | Low | Unclear | Low | Low | Low | Moderate |
| Walter, 2011 [36] | Hematologic malignancy | Low | Low | High | Low | Unclear | Low | Low | Low | Moderate |
| McCullough, 2012 [30] | Colorectal cancer | Low | Low | High | Low | Unclear | Low | Low | Low | Moderate |
| Meng, 2013 [31] | Colorectal cancer, colon cancer, proximal colon cancer, distal colon cancer, rectal cancer | High | Low | High | Low | Unclear | Low | Low for HPFS, high for NHS | Low for all outcomes | Moderate |
| Kim, 2018 [37] | Gastric cancer | High | Low | High | Low | Unclear | Low | Low | Low | Moderate |
![]()
Colorectal cancer
Three cohort studies reported associations between garlic intake and colorectal cancer risk (Table 5) [293031]. Three studies investigated garlic intake from different sources: 1 study each investigated garlic intake from food sources [31]; garlic supplements [29], and garlic intake from both food source and supplements [30]. Two studies reporting garlic intake from garlic supplements showed consistent results. One study reported that any garlic supplement use in the past 10 years significantly increased the risk of colorectal cancer compared with that of nonusers of garlic supplements (relative risk [RR] = 1.35, 95% confidence interval [CI] = 1.01, 1.81) [29]. The other study showed that past use of garlic supplements had a significant effect on total colorectal cancer risk compared with that in the never-user group (RR = 1.45, 95% CI = 1.02, 2.07) [30]. Two studies reporting garlic intake from food sources showed no significant associations between garlic intake and the risk for developing colorectal cancer [3031].
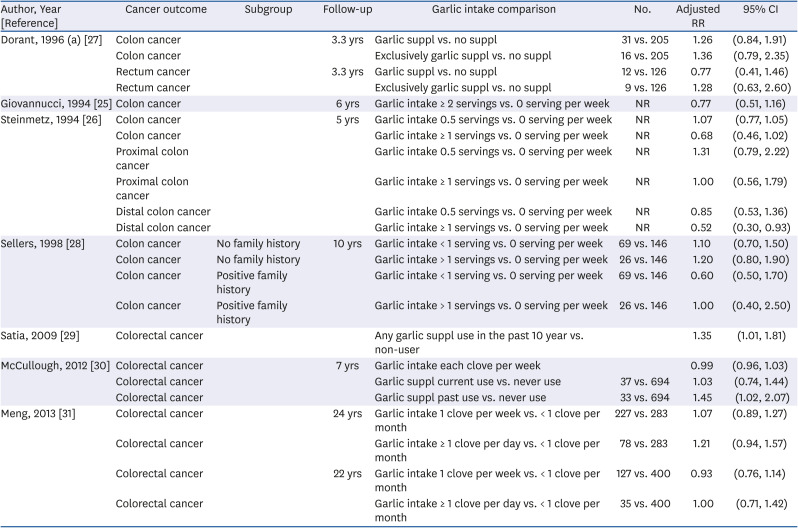
Table 5
Colorectal cancer risk stratified by garlic intake
| Author, Year [Reference] | Cancer outcome | Subgroup | Follow-up | Garlic intake comparison | No. | Adjusted RR | 95% CI |
|---|---|---|---|---|---|---|---|
| Dorant, 1996 (a) [27] | Colon cancer | 3.3 yrs | Garlic suppl vs. no suppl | 31 vs. 205 | 1.26 | (0.84, 1.91) | |
| Colon cancer | Exclusively garlic suppl vs. no suppl | 16 vs. 205 | 1.36 | (0.79, 2.35) | |||
| Rectum cancer | 3.3 yrs | Garlic suppl vs. no suppl | 12 vs. 126 | 0.77 | (0.41, 1.46) | ||
| Rectum cancer | Exclusively garlic suppl vs. no suppl | 9 vs. 126 | 1.28 | (0.63, 2.60) | |||
| Giovannucci, 1994 [25] | Colon cancer | 6 yrs | Garlic intake ≥ 2 servings vs. 0 serving per week | NR | 0.77 | (0.51, 1.16) | |
| Steinmetz, 1994 [26] | Colon cancer | 5 yrs | Garlic intake 0.5 servings vs. 0 serving per week | NR | 1.07 | (0.77, 1.05) | |
| Colon cancer | Garlic intake ≥ 1 servings vs. 0 serving per week | NR | 0.68 | (0.46, 1.02) | |||
| Proximal colon cancer | Garlic intake 0.5 servings vs. 0 serving per week | NR | 1.31 | (0.79, 2.22) | |||
| Proximal colon cancer | Garlic intake ≥ 1 servings vs. 0 serving per week | NR | 1.00 | (0.56, 1.79) | |||
| Distal colon cancer | Garlic intake 0.5 servings vs. 0 serving per week | NR | 0.85 | (0.53, 1.36) | |||
| Distal colon cancer | Garlic intake ≥ 1 servings vs. 0 serving per week | NR | 0.52 | (0.30, 0.93) | |||
| Sellers, 1998 [28] | Colon cancer | No family history | 10 yrs | Garlic intake < 1 serving vs. 0 serving per week | 69 vs. 146 | 1.10 | (0.70, 1.50) |
| Colon cancer | No family history | Garlic intake > 1 servings vs. 0 serving per week | 26 vs. 146 | 1.20 | (0.80, 1.90) | ||
| Colon cancer | Positive family history | Garlic intake < 1 serving vs. 0 serving per week | 69 vs. 146 | 0.60 | (0.50, 1.70) | ||
| Colon cancer | Positive family history | Garlic intake > 1 servings vs. 0 serving per week | 26 vs. 146 | 1.00 | (0.40, 2.50) | ||
| Satia, 2009 [29] | Colorectal cancer | Any garlic suppl use in the past 10 year vs. non-user | 1.35 | (1.01, 1.81) | |||
| McCullough, 2012 [30] | Colorectal cancer | 7 yrs | Garlic intake each clove per week | 0.99 | (0.96, 1.03) | ||
| Colorectal cancer | Garlic suppl current use vs. never use | 37 vs. 694 | 1.03 | (0.74, 1.44) | |||
| Colorectal cancer | Garlic suppl past use vs. never use | 33 vs. 694 | 1.45 | (1.02, 2.07) | |||
| Meng, 2013 [31] | Colorectal cancer | 24 yrs | Garlic intake 1 clove per week vs. < 1 clove per month | 227 vs. 283 | 1.07 | (0.89, 1.27) | |
| Colorectal cancer | Garlic intake ≥ 1 clove per day vs. < 1 clove per month | 78 vs. 283 | 1.21 | (0.94, 1.57) | |||
| Colorectal cancer | 22 yrs | Garlic intake 1 clove per week vs. < 1 clove per month | 127 vs. 400 | 0.93 | (0.76, 1.14) | ||
| Colorectal cancer | Garlic intake ≥ 1 clove per day vs. < 1 clove per month | 35 vs. 400 | 1.00 | (0.71, 1.42) |
![]()
Colon cancer
Three cohort studies and one case-cohort study [25262728] examined associations between garlic intake and colon cancer (Table 5). The three cohort studies examined garlic intake from food sources, and the case-cohort study investigated garlic supplements. All 3 cohort studies examining garlic intake from food sources reported no significant associations between garlic intake and colorectal cancer [252628]. One case-cohort study reported that garlic supplement users had a significantly increased risk of developing colon cancer compared with nonusers (RR = 1.45, 95% CI = 1.02, 2.07) [27].
Other cancers (lung cancer, stomach cancer, prostate cancer, breast cancer, and hematologic malignancy)
Prospective observational studies
Three cohort and 3 case-cohort studies [29323334353637] investigated the associations between garlic intake and other types of cancer (Table 6). There were 2 studies each of lung cancer and stomach cancer. Additionally, there was only 1 study each of prostate cancer, breast cancer, and hematologic malignancy.
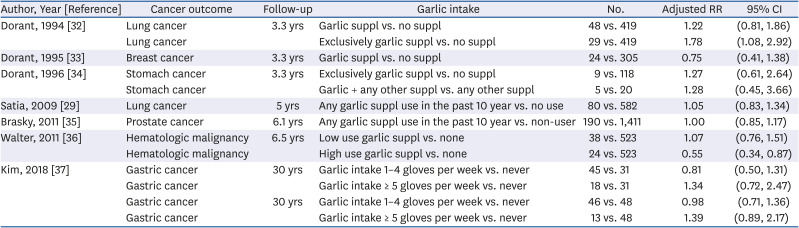
Table 6
Other types of cancer risk stratified by garlic intake
| Author, Year [Reference] | Cancer outcome | Follow-up | Garlic intake | No. | Adjusted RR | 95% CI |
|---|---|---|---|---|---|---|
| Dorant, 1994 [32] | Lung cancer | 3.3 yrs | Garlic suppl vs. no suppl | 48 vs. 419 | 1.22 | (0.81, 1.86) |
| Lung cancer | Exclusively garlic suppl vs. no suppl | 29 vs. 419 | 1.78 | (1.08, 2.92) | ||
| Dorant, 1995 [33] | Breast cancer | 3.3 yrs | Garlic suppl vs. no suppl | 24 vs. 305 | 0.75 | (0.41, 1.38) |
| Dorant, 1996 [34] | Stomach cancer | 3.3 yrs | Exclusively garlic suppl vs. no suppl | 9 vs. 118 | 1.27 | (0.61, 2.64) |
| Stomach cancer | Garlic + any other suppl vs. any other suppl | 5 vs. 20 | 1.28 | (0.45, 3.66) | ||
| Satia, 2009 [29] | Lung cancer | 5 yrs | Any garlic suppl use in the past 10 year vs. no use | 80 vs. 582 | 1.05 | (0.83, 1.34) |
| Brasky, 2011 [35] | Prostate cancer | 6.1 yrs | Any garlic suppl use in the past 10 year vs. non-user | 190 vs. 1,411 | 1.00 | (0.85, 1.17) |
| Walter, 2011 [36] | Hematologic malignancy | 6.5 yrs | Low use garlic suppl vs. none | 38 vs. 523 | 1.07 | (0.76, 1.51) |
| Hematologic malignancy | High use garlic suppl vs. none | 24 vs. 523 | 0.55 | (0.34, 0.87) | ||
| Kim, 2018 [37] | Gastric cancer | 30 yrs | Garlic intake 1–4 gloves per week vs. never | 45 vs. 31 | 0.81 | (0.50, 1.31) |
| Gastric cancer | Garlic intake ≥ 5 gloves per week vs. never | 18 vs. 31 | 1.34 | (0.72, 2.47) | ||
| Gastric cancer | 30 yrs | Garlic intake 1–4 gloves per week vs. never | 46 vs. 48 | 0.98 | (0.71, 1.36) | |
| Gastric cancer | Garlic intake ≥ 5 gloves per week vs. never | 13 vs. 48 | 1.39 | (0.89, 2.17) |
![]()
Lung cancer
One cohort and one case-cohort studies examining the relationship between garlic intake and lung cancer showed inconsistent results (Table 6) [2932]. One study showed that the exclusive use of garlic supplements significantly increased the risk of lung cancer [32]. The other study reported a nonsignificant relationship between garlic supplement intake and lung cancer [29].
Hematologic malignancy, breast cancer, and prostate cancer
One cohort study asserted that high use of garlic supplements (≥ 4 days per week) significantly decreased the risk of hematologic malignancy compared with that of nonusers (hazard ratio = 0.55; 95% CI = −0.34, 0.87) (Table 6) [36]. Additionally, a few studies found nonsignificant relationships between garlic supplement intake and the risk of breast cancer [33] and prostate cancer [35].
Overall SoE
We graded the overall SoE, and it was inadequate for the causal effects of garlic intake on colorectal cancer, lung cancer, and stomach cancer (Table 7).
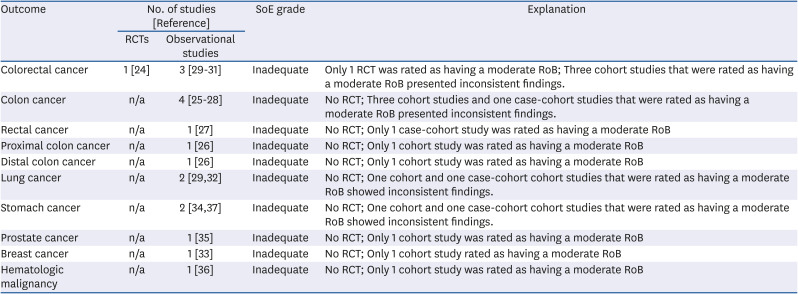
Table 7
SoE grading: garlic intake by outcome1)
| Outcome | No. of studies [Reference] | SoE grade | Explanation | |
|---|---|---|---|---|
| RCTs | Observational studies | |||
| Colorectal cancer | 1 [24] | 3 [293031] | Inadequate | Only 1 RCT was rated as having a moderate RoB; Three cohort studies that were rated as having a moderate RoB presented inconsistent findings. |
| Colon cancer | n/a | 4 [25262728] | Inadequate | No RCT; Three cohort studies and one case-cohort studies that were rated as having a moderate RoB presented inconsistent findings. |
| Rectal cancer | n/a | 1 [27] | Inadequate | No RCT; Only 1 case-cohort study was rated as having a moderate RoB |
| Proximal colon cancer | n/a | 1 [26] | Inadequate | No RCT; Only 1 cohort study was rated as having a moderate RoB |
| Distal colon cancer | n/a | 1 [26] | Inadequate | No RCT; Only 1 cohort study was rated as having a moderate RoB |
| Lung cancer | n/a | 2 [2932] | Inadequate | No RCT; One cohort and one case-cohort cohort studies that were rated as having a moderate RoB showed inconsistent findings. |
| Stomach cancer | n/a | 2 [3437] | Inadequate | No RCT; One cohort and one case-cohort cohort studies that were rated as having a moderate RoB showed inconsistent findings. |
| Prostate cancer | n/a | 1 [35] | Inadequate | No RCT; Only 1 cohort study was rated as having a moderate RoB |
| Breast cancer | n/a | 1 [33] | Inadequate | No RCT; Only 1 cohort study rated as having a moderate RoB |
| Hematologic malignancy | n/a | 1 [36] | Inadequate | No RCT; Only 1 cohort study was rated as having a moderate RoB |
SoE, strength of evidence; RCT, randomized controlled trial; RoB, risk of bias; n/a, not applicable.
1)The SoE grading scheme is presented in Supplementary Table 2.
![]()
Adverse events
The one included RCT of garlic supplements [24] identified adverse events. One participant in the high-dose AGE group had itching on the back, and three participants in the low-dose AGE group reported eczema on the upper limbs, glossitis, and epigastric pain.
DISCUSSION
This systematic review identified insufficient evidence to draw conclusions for the causal relationship between garlic intake and cancer. Only one small RCT was identified, and the included cohort studies presented large methodological heterogeneity (i.e., follow-up duration, types of garlic intake: supplements, food, or both, assessment tool of garlic exposure, and various comparison groups) hindering the comparability of the results.
Up to now, garlic has been reported that has favorable effects against cancer in vitro and in animal studies. Their major compounds were well known as allicin, ajoene, DAS, DADS, and DATS. Among them, DAS is the major ingredient of cooked garlic which comprise about 60% of garlic oil [38]. The mechanism of anticancer effects of garlic ingredients has been revealed through the animal and human cancer cell line experiments. Previous research have reported that DAS can decrease testosterone and N-methyl-N-nitrosourea (MNU) induced carcinogenesis in the prostate gland of rats [39], and dwindle the incidence of tumor formation in MNU-induced carcinogenesis in mammary glands through inhibition of DNA alkylation as well as formation of two nitrosamine-related DNA adducts; O(6)-methylguanine and N(7)-methylguanine [40]. DADS reduced benzo[a]pyrene-induced carcinogenesis in human hepatoma cells through inhibition of the cytochrome P450 activity [41]. Several studies have revealed that the antiproliferative property of DADS in cultured human colon tumor cells (HCT-15) relative to its ability to decrease the proportion of cells in the G1 phase and increase the proportion of cells in the G2/M phase. All of these results suggested that the DADS compound can exert antiproliferative effects through cell cycle arresting in mitosis, which leads to apoptosis [42]. Additionally, DADS increases reactive oxygen species and oxidative stress that can induce apoptosis in many types of mammalian tumor cells [43]. The mechanisms by which DAD, DADS, the major components of garlic, elicit anti-cancer activity include histone acetylation, endoplasmic reticulum stress, and the Fas-mediated cell death pathway [44]. In this systematic review, we could not provide clear scientific conclusions regarding the effects of garlic on cancer because analytical and process information of garlic supplement or garlic intake were not reported in the included studies. The amount of individual garlic component (e.g., allicin) could be affected by various factors such as types of garlic, cooking, smashing, storage, and method of preservation.
We must concede that despite the many studies that have done, the conclusions of this present review do not differ greatly from that of a previous done almost two decades ago. Fleischauer and Arab [45] reported in 2001 the relationship between garlic intake and cancer incidence in 19 case-control or cohort studies. This report stated that only a few retrospective case-control studies showed inverse association of garlic intake with stomach and colorectal cancer, but the included cohort studies did not show any significant relationship for stomach and colorectal cancers. Similar to what we found in this systematic review, the authors pointed out a limited number of studies, inappropriate adjustment for potential confounding factors, and inaccurate measure of garlic intake would make it hard to come to a reliable conclusion.
In prospective observational studies, we found contradictory results on the relationship between the cancer outcomes and various types of garlic intake (i.e., food and supplement). As for colorectal cancer, 2 studies [2930] showed that the intake of garlic supplements increased the risk of colorectal cancer, while 2 studies [3031] did not show significant associations between garlic intake from food sources and the risk of colorectal cancer. In the case of colon cancer, one study showed that the intake of garlic supplementation increased the risk of colon cancer [27], while 3 studies revealed that there was no significant relationship between the garlic intake from food sources and the risk of colon cancer [252628]. Additionally, rectal cancer was not significantly related with the intake of garlic supplement [27]. However, garlic intake from food sources significantly decreased the risk of distal colon cancer [26]. Therefore, we found the varying relationship between garlic intake and colon cancer may vary depending on how garlic is consumed and where colorectal cancer occurs. In the case of lung cancer, one study [32] showed that garlic supplementation increased the risk of lung cancer, while another study [29] revealed no significant association between garlic supplementation and the risk of lung cancer. From the results of this study, it is speculated that it is best to consume an appropriate amount of garlic in the form of food, not supplements. Generally, our body would absorb and metabolize nutrients from complex mixtures in foods. Thus, if the nutrients are consumed in a purified or concentrated supplements form, they can easily interfere with the absorption of other nutrients from foods consumed at the same time [46]. Therefore, it is safe and recommended to eat garlic as a food at a daily table.
The strength of this systematic review is that we have used robust study eligibility criteria for the study designs. However, this systematic review has a few limitations. All included observational studies have a high risk of bias in ascertainment of nutrient exposure. The included observational studies employed either food frequency questionnaire to assess dietary intake of garlic or specific questionnaire to measure consumption of garlic supplements. FFQs have inherent measurement errors in cohort studies [47], while multiple 24-hour dietary recalls or diet diaries are considered as a more accurate instrument [48]. In addition, the included studies did not provide information on how the garlic dosages were prepared. The concentration of allicin intake from garlic supplements and garlic foods consumption depends on a set of variables, including moisture content, temperature conservation, type of garlic used, storage conditions [49]. When clinical studies do not determine allicin bioavailability from the garlic samples used [50], it is difficult to correctly judge the final composition of garlic samples. Taken into consideration of the limitations in this systematic review, we suggest future studies to employ a more objective measurement of garlic consumption, to overcome the limitations of using FFQs. There are several promising biomarkers for garlic consumption such as S-allyl-mercapturic acid, allyl methyl sulfide, allyl methyl sulfoxide, allyl methyl sulfone, and SAC [51]. Using biomarkers to quantify dietary intake will enable future systematic reviews to correctly capture and compare the effect of garlic intake in all included studies.
In conclusion, one RCT showed that the aged garlic extract significantly decreased the size and number of colorectal adenomas, while several cohort studies indicated inconsistent relationships between garlic intake and colorectal cancer. We determined that the SoE was inadequate for the effects of garlic intake on cancers due to insufficient number of good-quality RCTs. We recommend that more prospective cohort studies, from the countries to have population with higher intake of garlic, such as Italia and South Korea, are needed to be included for the future systematic reviews.
 XML Download
XML Download