

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although patients cared for in an intensive care unit (ICU) exhibit a steep rise in their nutritional needs due to hypermetabolism and protein catabolism, there are several difficulties in achieving these requirements. A low nutritional supply to patients in the ICU is known to cause malnutrition, an increase in infectious complications, an increase in the number of days of mechanical ventilation and hospitalization, and an increase in medical expense [1].
For patients in the ICU with normal gastrointestinal (GI) function, the first choice of nutritional support is enteral nutrition (EN) [2]. However, the delay or cessation of EN support often results in various EN complications, making it difficult for these patients to reach nutritional goals [13]. One of the most common complication types during EN administration is GI complication, including vomiting, abdominal distension, loss of bowel sounds, GI bleeding, high gastric residual volume (GRV), and diarrhea.
Diarrhea is one of the most common GI complications, occurring in 2%–95% of patients receiving EN [4]. A possible cause of diarrhea in EN is high osmotic pressure due to the presence of fermentable short-chain saccharides [5]. However, there are few studies on this subject [6]. Fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) are fermentable short-chain saccharides that include fructose (monosaccharide), lactose (disaccharide), fructans, galactans (oligosaccharides), and polyols. They are present in regular food, and their absorption rate in the small intestine is low. Therefore, FODMAPs can cause gas production in the colon, along with abdominal distension [7]. This can be mainly observed in patients with irritable bowel syndrome (IBS), and there is a report that lowering the level of FODMAPs in the diet is effective for reducing GI symptoms in IBS patients [8]. In 2013, when a low-FODMAP diet was supplied to 90 patients with IBS for 15.7 months, there was a significant improvement in abdominal pain, bloating, flatulence, and diarrhea symptoms [9]. In 2014, Halmos et al. [10] conducted a controlled, cross-over study on patients with and without IBS. As a result of alternating a typical Australian diet and a low-FODMAP diet, patients with IBS showed a significant improvement in composite scores reflecting bloating, abdominal pain, and dissatisfaction with stool consistency.
When included in an EN formula, FODMAPs are in the form of inulin, fructo-oligosaccharides, fructans, and galacto-oligosaccharides. They are known to affect intraluminal osmotic pressure [11], the transport of water to the colon, and gas production by bacterial fermentation [12]. They also cause abdominal distension and discomfort under overdose conditions [1112]. An analysis of the causes of diarrhea in 160 hospitalized patients in Australia showed that a low FODMAPs content in an EN formula was significantly correlated with decreased diarrhea [13]; a similar result was reported in another study [14].
There are few studies on GI complications according to the FODMAPs content [15], and even fewer such studies in the ICU. Therefore, we investigated the differences in GI complications according to the FODMAPs content in an EN formula, targeting patients who received EN for the first time in the ICU.
Go to : 
SUBJECTS AND METHODS
Patients
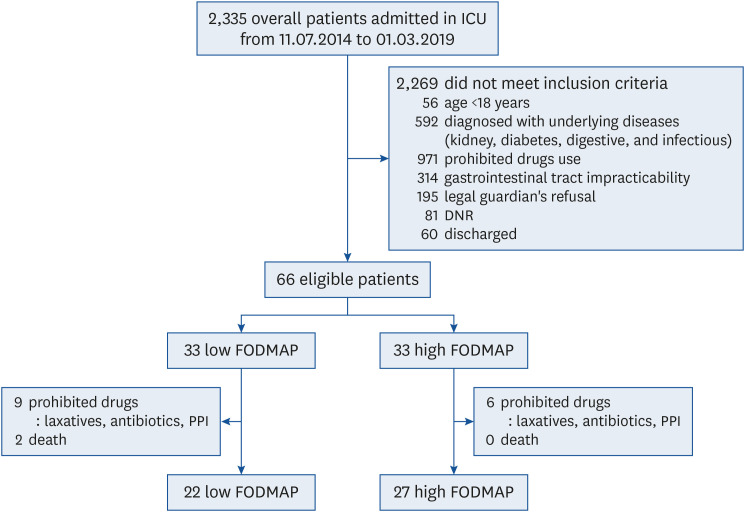
The subjects were patients admitted to the ICU of a medical center in the Republic of Korea, and the research period was approximately 5 years, from July 2014 to July 2019 (Fig. 1). The study was approved by the center's ethical committee (BD2014-085) and was registered as KCT0005660. The subjects were adult patients over 18 years of age who entered the ICU and were initiated on EN support using standard formulations, not special formulations (such as diabetes/kidney/concentration/high protein formulations). Since the subjects were not conscious enough to provide consent for the study, we explained and obtained the consent of their legal guardians. Patients diagnosed with underlying diseases like diabetes, kidney diseases, digestive diseases, and infectious diseases and on medication for the related disease in the last 6 months were excluded. Patients who were being administered proton pump inhibitors (PPIs), antibiotics (except β-lactam antibiotics), antifungal agents, and laxatives were excluded.
Materials
A total of 66 patients who were placed on EN support after entering the ICU were divided into 2 groups of 33 patients as case or control groups (Fig. 1). They were alternately assigned in series order to 1 of the 2 experimental groups, i.e., case or control group. Accordingly, separate formulations (Greenbia Gut-Solution and Greenbia TF; Dr. Chung's Food Inc., Cheongju, Korea) were used in the case and control groups, respectively. The 2 formulations differed in their carbohydrate, protein, and fat ratios, but their macronutrient ratios were formulated to follow and be within the guideline of Korean dietary reference intakes. In other words, the case group was supplied a low level of FODMAPs (approximately 1.6 g/L), and the control group was supplied a high level of FODMAPs (approximately 5.79 g/L) (Table 1). The study was conducted for 7 days after initiating EN, and the same protocol was applied to the case and control groups for those 7 days.
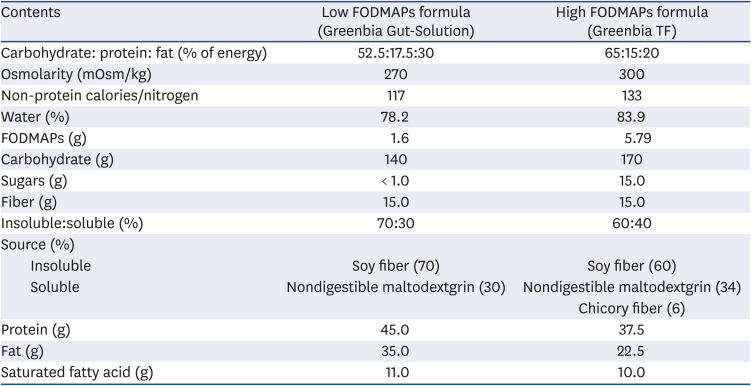
Table 1
Comparison of the 2 formulae used in the study (1,000 kcal/1,000 mL)
![]()
The nutritional requirements of the subjects were calculated using a general formula to provide 25–30 kcal/kg body weight, and the protein requirements were aimed at supplying 1.2–1.5 g/kg [16]. The method of supply and the rate of increase of the EN supply was as follows: on the first day of the implementation, treatment started at 600 kcal/600 mL and was injected by gravity at an amount of 70–150 cc per hour. In the absence of GI complications, a daily increase of 200 kcal/200 mL was achieved until the final requirement demand was reached. All EN administration was performed using a nasogastric tube.
Data collection
The following data were collected. Information related to a patient's general characteristics and conditions included age, sex, height, weight, body mass index (BMI; kg/m2), appropriateness of ICU placement (ICU Simplified Acute Physiology Score 3; SAPS 3 score), and diagnostic category. The status of nothing by mouth (NPO) and the usage of antibiotics were assessed the day before the study began (Table 2). Items related to assessing the infusion of EN were total energy kilocalories per kilogram and total protein grams per kilograms for study days 1 and 7 (Table 3). For GI system evaluation, 6 items were investigated: diarrhea, vomiting, GRV before the first EN treatment in the morning, abnormal bowel sounds, abdominal distension, and lack of defecation days (Table 4). Evaluations of bowel sounds and abdominal softness were conducted by medical staff. After listening for about 30 seconds in the 4 quadrants of the abdomen, bowel sounds were divided into 4 categories (normal, advanced, reduced, and none) [17]. Abdominal softness was checked by palpating the abdomen for the presence of abdominal distension [17]. King's Stool Chart was used to define diarrhea; bowel movements were divided into 12 categories according to the concentration and amount of fecal material, and then scored by category. If the total daily sum of the scores was 15 or more, diarrhea was diagnosed [18].
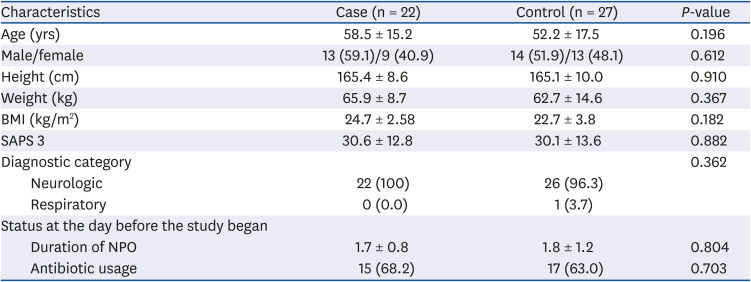

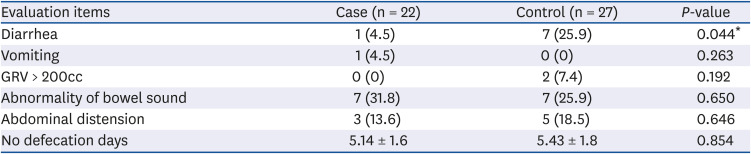
Table 2
General characteristics of the study groups
Data are shown as mean ± SD or number (%).
BMI, body mass index; SAPS 3, simplified acute physiology score 3; NPO, nothing by mouth.
![]()
Table 3
Comparison of daily nutritional intake in the study groups
![]()
Table 4
Gastrointestinal evaluation of outcomes of the study groups
Data are shown as mean ± SD or number (%).
GRV, gastric residual volume.
*P < 0.05 was considered statistically significant.
![]()
Statistical analysis
Statistical analysis was conducted using SPSS 25.0 for Windows (SPSS Inc., Chicago, IL, USA); differences between the 2 groups were determined to be significant if the P-value of an independent t-test was < 0.05. The t-test was used because the data for continuous variables were normally distributed (Shapiro-Wilk). The nominal scale variables were analyzed by applying the chi-squared test, and the survival rate for diarrhea for 7 days was conducted by undertaking Kaplan-Meier survival analysis.
Go to :
RESULTS
Baseline characteristics of the study patients
The general characteristics and conditions of the 2 groups are summarized in Table 2. The average ages were 58.5 and 52.2 years in the case and control groups, respectively, and the proportions of men were 59.1% and 51.9% in the case and control group, respectively; there were no statistical differences between the ages and sex compositions of the 2 groups. In addition, there were no significant differences in the heights, weights, BMIs, SAPS 3 scores, and diagnostic categories between the 2 groups. Before the study began, the average durations of NPO status were 1.7 days and 1.8 days in the case and control groups, respectively, and were not significantly different (P = 0.804). The day before the study began, usage of antibiotics was 68.2% and 63.0% in the case and control groups, respectively (P = 0.703).
Comparison between the 2 groups according to nutrition and GI evaluation
The nutritional targets of the case and control groups were 24.7 kcal/kg and 25.3 kcal/kg, respectively, and the proportions of those reaching their requirement through EN treatment during the 7-day study period were 68% and 70% in the case and control groups, respectively. The nutritional intake states of both groups are summarized in Table 3. The energy supply was not significantly different between the case and control groups on the 1st and 7th day of the study (P =0.136 and P = 0.918, respectively). Moreover, the level of protein supply was not significantly different between the case and control groups on the 1st and the 7th day (P = 0.092 and P = 0.130, respectively).
The results of the GI evaluation and associated outcomes are described in Table 4. Among the 6 items evaluated, there was a statistically significant difference between the 2 groups only in diarrhea difference (P = 0.044); diarrhea was observed only in 1 patient (4.5%) in the case group, whereas in the control group, it was observed in 7 patients (25.9%). In addition, the incidences of diarrhea in the 2 groups over the 7-day study period underwent Kaplan-Meier survival analysis. As shown in Fig. 2, the incidence of diarrhea in the case group was significantly lower than that in the control group (P = 0.048, Fig. 2). In the rest of the GI items, there were no statistical differences, and pressure ulcers did not occur in either group.
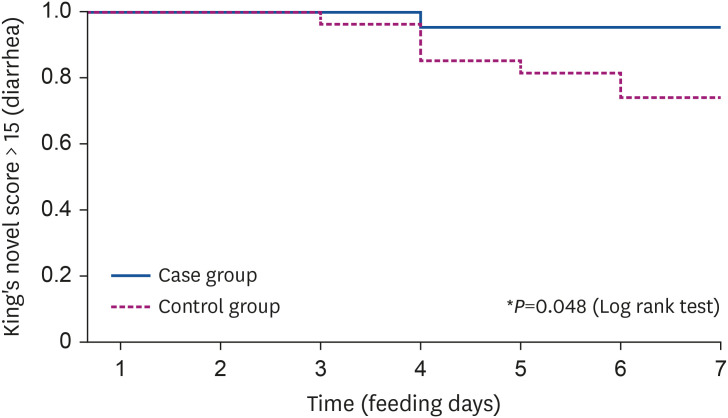 | Fig. 2Kaplan-Meier plot for diarrhea occurrence during the study period.The incidence of diarrhea during the 7-day study period underwent Kaplan-Meier survival analysis. The incidence of diarrhea in the case group was significantly lower than that in the control group. In addition, diarrhea first occurred on the 3rd day in the control group and on the 4th day in the case group.
*P < 0.05 was considered statistically significant.
|
Factors associated with medications
The medications used during the study period in both groups are described in Table 5. The rates of prokinetic use during the study period were 13.6% and 14.8% in the case and control groups, respectively, and there was no statistical difference between the 2 groups (P = 0.907). Comparison of the use of antibiotics (only β-lactam antibiotics) revealed no significant difference between the 2 groups (P = 0.678); 95.5% and 92.6% antibiotic usage in the case and control groups, respectively. The duration of prokinetic usage was 1.3 days and 2.0 days in the case and control groups, respectively, and the difference was not significant (P = 0.484). The starting day of prokinetic usage was 3.3 days and 5.0 days in the case and control groups, respectively, and there was no significant difference (P = 0.445). The duration of antibiotic usage was 6.4 days and 6.6 days in the case and control groups, respectively, and the difference was not significant (P = 0.601). The starting day of antibiotic usage was 1.4 days and 1.0 days in the case and control groups, respectively, and there was no significant difference (P = 0.186). The results of the analysis by antibiotic regimen type showed that the highest proportions of antibiotics administered were for patients only receiving cephalosporin type antibiotics at 81.0% and 76.0% in the case and control groups, respectively. The percentage administered only the piperacillin/tazobactam type was notably lower; 9.5% and 0.0% in the case and control groups, respectively. The percentage of patients administered both cephalosporin and piperacillin/tazobactam types was also low; 9.5% and 24.0% in the case and control groups, respectively, and there was no significant difference between the 2 groups (P = 0.150).
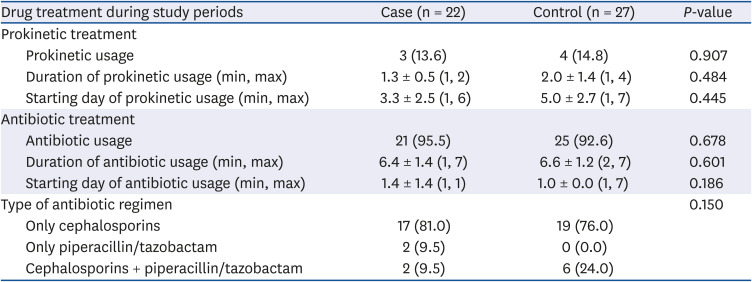
Table 5
Drug treatments administered in the study groups
![]()
There were 11 and 6 dropouts in the case and control groups, respectively (Table 6). On average, dropout occurred after 4.0 days and 2.8 days in the case and control groups, respectively, and that difference was not significant (P = 0.088). The most common reason for dropout was the use of prohibited drugs-antibiotics, which occurred in 5 cases (45.5%) and 4 cases (66.7%) in the case and the control group, respectively. Of the 6 dropouts in the case group, 2 were the result of death, 1 for constipation, 2 for vomiting, and 1 for GI bleeding. In the 2 patients whose cause of dropout was vomiting, the vomitus volume was more than 150 cc and enemas were administered. In the control group, 2 cases dropped out due to constipation. Among the reasons for dropout, diarrhea was not the cause in either group. Moreover, there was no significant difference in dropout percentage between the 2 groups (P = 0.361).
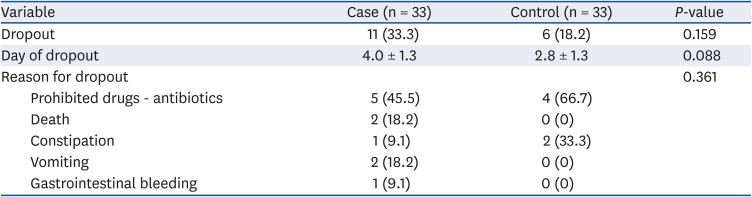
Table 6
Reasons for case dropout
![]()
Go to :
DISCUSSION
Intolerance to EN is a common feature among patients in the ICU [19], and this intolerance is related to GI function failure, indigestion, decreased absorption capacity, and drug side effects. About 50% of patients in the ICU who receive EN are reported to display intolerance symptoms such as high GRV, decreased bowel function, vomiting, and diarrhea [2021]. Diarrhea can be defined as 3 to 5 bowel movements a day with a stool amount of 200–300 g/day [22]; in this study, a total sum score of 15 points or more, obtained by using the King's Stool Chart, was used to define diarrhea. The causes of diarrhea are diverse, but mainly include administration of various drugs, infections, bacterial contamination, and diseases [14]. If diarrhea occurs due to EN intolerance, malnutrition, infection, dehydration, or other conditions may occur and may result from associated factors such as fasting [23].
The 2 EN formulae used in this study had different carbohydrate, protein, and fat content levels (Table 1). Differences in the nutritional design of the 2 formulae resulted in differences in carbohydrate content, which, during the manufacturing process, can result in differences in the FODMAPs components. In the manufacturing process, the amounts of dextrin and sucrose used in the low FODMAPs formula were less than in the high FODMAPs formula, which results in differences in carbohydrate and sugar contents, and those changes are designed to limit the FODMAPs from the raw materials. The protein and fat content in the case group was higher because the calorie levels in the 2 formulae were adjusted to be equal (Table 1). However, the nutritional designs of the 2 formulae reflect typical formulae, and as the differences were not significant, it could not have affected the occurrence of diarrhea. The 2 formulae used in this study were within the normal osmotic pressure range of below 300 mOsm/kg [24], and the osmotic pressures in the 2 study groups were similar; 270 and 300 mOsm/kg in the case and control group, respectively. Typically, in terms of GI tract adaptation of patients receiving EN, the iso-osmolarity of the EN formula is deemed more important than the osmotic pressure [25]. Therefore, the osmotic pressure difference in the 2 groups did not affect the occurrence of diarrhea. The fiber content of both the case and control formulations consisted of insoluble and soluble fibers. There was a small difference between the case and control groups in the insoluble vs. soluble ratio (70:30 and 60:40, respectively). The source of insoluble fiber was soy fiber, which is composed of hemicellulose and cellulose. Nondigestible maltodextrin is commonly used as soluble fiber as it is a low viscosity, water-soluble, and indigestible dextrin produced by heat and enzymatic treatments of cornstarch. Soluble fibers delay gastric emptying and increase transit time through the intestine. In contrast, insoluble fibers decrease intestinal transit time and increase fecal bulk. Insoluble fiber absorbs water and increases stool volume while preventing diarrhea, and it stimulates the intestine, activating bowel movements. Soluble fiber is viscous and becomes a gel-like soft and sticky form that passes through the intestine [26]. The control formulation contained 6% chicory fiber as soluble fiber. Although many reports have suggested that soluble fiber is effective in reducing diarrhea [2728], our results showed a high incidence of diarrhea in the control group administered a formulation with a high soluble fiber ratio. This is thought to be due to the predominant influence of the FODMAPs in that formulation. Although there are nutritional design differences between the 2 formulae, nutritional contents were not significantly associated with diarrhea, except for the FODMAPs content.
The usefulness of a low-FODMAP diet was reported for patients who received EN. In 2010, Halmos et al. [13] retrospectively analyzed 160 patients receiving EN, of which 61% had diarrhea. According to their report, diarrhea was significantly reduced in patients with a length of hospital stay of over 21 days, an EN duration of over 11 days, and who were administered a formula with low content of FODMAPs. In a recent randomized controlled trial, 84 patients receiving EN were divided into 3 groups: low-FODMAP (0.320 g/200 mL), moderate-FODMAP (0.753 g/200 mL), and high-FODMAP (1.222 g/200 mL). Diarrhea was significantly lower in the low-FODMAP group than in the other groups [29]. In our study, the subjects were divided into low-FODMAP and high-FODMAP groups, and the GI complications were compared between the groups. Diarrhea occurred in 1 case (4.5%) and 7 cases (25.9%) in the low-FODMAP and the high-FODMAP group, respectively, and this difference was statistically significant (P = 0.044; Table 4). In addition, a Kaplan-Meier survival analysis showed that the case group had a significantly lower diarrhea incidence (P = 0.048) than that in the control group (Fig. 2). Although the observation is not statistically meaningful, diarrhea occurred for the first time on the 4th day in the case group, and on the 3rd day in the control group; therefore, diarrhea occurred relatively late in the case group.
The types of drugs that cause diarrhea in patients being treated in an ICU are diverse. These include laxatives, prokinetics, antibiotics, hyperosmolar oral liquid medications, and sorbitol-containing agents [3031]. We conducted this study with a strict prohibition of laxatives, antifungals, PPI, and antibiotics (except of β-lactam antibiotics). The use of acceptable medications such as prokinetics and β-lactam antibiotics was not significantly different between the 2 groups (Table 5). The use of prokinetic agents is common in the ICU due to feeding intolerance and delayed gastric emptying [32]. As our study focused on critically ill patients, the use of prokinetic agents was acceptable. However, they were not used from the beginning of the study. The starting day for prokinetic use was not significantly different between the 2 groups (3.3 days in the case group and 5.0 days in the control group; P = 0.445). Moreover, the duration of prokinetic usage was not significantly different between the groups (1.3 days in the case group and 2.0 days in the control group; P = 0.484) (Table 5). Antibiotics are reported to increase the incidence of diarrhea during EN administration [33], and antibiotics of the aminoglycoside, piperacillin-tazobactam, and clindamycin/metronidazole families have been significantly associated with a high incidence of diarrhea [31]. The β-lactam antibiotics used in this study included piperacillin-tazobactam. β-lactam antibiotics are widely prescribed for managing infections in critical care units [34]; however, β-lactam antibiotics have been associated with the highest frequencies of antibiotic-associated diarrhea [35]. In this study, β-lactam antibiotics were excluded from the list of prohibited drugs, in order to increase the number of enrolled subjects. A preliminary assessment showed that the number of subjects that would be enrolled in the study was too small when β-lactam antibiotics were excluded; therefore, if they were excluded, it would have been impossible to proceed with the study. The usage rate, duration of antibiotic usage, starting day of antibiotic usage, and regimen type were compared in the 2 groups (Table 5), and no significant differences between the 2 groups were detected (P = 0.678, P = 0.601, P = 0.186, and P = 0.150, respectively). The number of subjects administered with only piperacillin/tazobactam in the case and control group were 2 and 0, respectively. The number of subjects administered both cephalosporins and piperacillin/tazobactam in the case and control group were 2 and 6, respectively, and the proportions in the 2 groups were no significantly different (P = 0.150). In a previous study, piperacillin-tazobactam has been associated with diarrhea in 3.8%–34.3% of cases [36]. In the present study, of the total 10 subjects administered piperacillin/tazobactam, diarrhea occurred in only 2 patients in the control group (data not shown).
There are several limitations in this study. First, the number of subjects was too small. β-lactamase antibiotic use was not excluded from the study as it was not easy to select other subjects because drug use had to be strictly limited while receiving treatment in the ICU for more than 7 days (Table 6). Therefore, even though it took a long time to enroll subjects, the number of subjects was not large. The study has a small sample size and was conducted so as to avoid prohibited drugs; therefore, based on those limitations, the relationships between FODMAPs and GI problems, especially diarrhea, are not considered conclusive. Second, the study period was as short as 7 days, because the average admission period in the ICU in our hospital was 7 days; therefore, it was impossible to observe patients for more than 7 days. In 2015, in a study by Yoon et al. [29] that was conducted for 2 weeks, subjects receiving EN were divided into low-FODMAP, moderate-FODMAP, and high-FODMAP groups without drug restrictions, and results similar to ours were reported; that is, the low-FODMAP group reported reduced diarrhea symptoms and improved nutritional status. We restricted drug usage and had a short study period (7 days); regardless, we obtained results similar to those of the 14-day study. In the future, if this type of study is extended to include patients in general wards, the study period could be expanded beyond the 7-day limit. Through such studies, we could better identify the relationship between FODMAPs and GI complications other than diarrhea.
Our results suggest that a low-FODMAP EN formula may provide a practical therapeutic approach for patients receiving EN and suffering from GI complications, particularly diarrhea. The incidence of diarrhea was significantly lower in the low-FODMAP EN formula group than in the high-FODMAP EN formula group. As the number of enrolled subjects was small and the study period short, further studies with more enrolled subjects and more extended study periods are needed to determine the effects of FODMAPs on diarrhea and other GI complications.
Go to :
 XML Download
XML Download