

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Age is an important determining factor for the treatment method in femoral neck fractures.1 In general, surgeons prefer internal fixation for patients aged 60 years or younger and arthroplasty for patients who are older than 65 years.2 Deciding which type of arthroplasty, total hip arthroplasty (THA) versus hemiarthroplasty (HA), to do in elderly femoral neck fracture patients has been a controversial issue.3 Even though an earlier study reported favorable results of HA,4 groin pain and acetabular erosion appeared as concerns after the HA.5
Comparative studies of HA and THA in the 2010s reported superior clinical results and similar mortalities after THA compared to HA in these patient cohorts.156789101112131415 Thus, THA has been favored more than HA and is currently in increasing use.16 Population aged > 65 years has been considered to be elderly. Currently, with an increase in life expectancy, the size of population older than 80 years is growing.17
Because THA is associated with longer operation time and more bleeding than HA,8 THA might lead to higher mortality compared to HA in the older elderly (> 80 years) pateints. However, previous studies addressed the elderly patients as those older than 65 years, and there has been no study involving patients older than 80 years or comparing patients aged < 80 years and those aged > 80 years. Furthermore, several randomized controlled trials (RCTs) could not exclude selection bias due to small sample sizes.1418 In addition, there are gaps in guidelines on how to treat femoral neck fractures between surgeons and institutions.219
Therefore, the nationwide representative claims data used in this study reflected all of the skills and experiences of the surgeons in our country and thus, prevented selection bias. The purpose of this study is to compare the mortality rate, length of hospital stay and transfusion volume between HA and THA due to femoral neck fracture in two age groups: 1) patients aged 65–79 years and 2) those aged 80–99 years.
Go to : 
METHODS
Data source
The Korean National Health Insurance Service (KNHIS) database includes medical information such as demographics, diagnostic codes, and treatment procedure codes from all South Korean institutions.2021 NHIS-Senior cohort (a total of 588,147 participants) was constructed by KNHIS through simple random sampling, 10% of the population of about 5.5 million South Korean enrollees older than 60 years of age in 2002. The KNHIS-Senior cohort represent the elderly population living in South Korea. All individuals except those who emigrated or died were followed until 2015.
Incident femoral neck fracture cohort and all-cause mortality
The eligibility criteria were: 1) a first-time admission to acute care hospitals with the diagnostic code of femoral neck fracture (International Statistical Classification of Disease and Related Health Problems, 10th Revision; ICD-10, S720); 2) at least a 3-year hip fracture-free period before the enrollment to exclude bilateral femoral neck fracture patients; 3) treatment with HA or THA, and 4) age between 65 and 99 at the time of the admission due to the fracture.22 Patients who had a femoral neck fracture in 2015 were excluded to ensure the minimum 1-year follow-up period. The incidence date (index date or time zero) of the femoral neck fracture was defined as the date of admission to the acute care hospital.
In the KNHIS-Senior cohort, each subject's unique de-identified number was linked to mortality information provided by the Korean National Statistical Office.21
The primary outcome was the mortality rate, and the secondary outcomes were the duration of hospitalization and the amount of transfusion.
The elderly cohort was divided in two groups according to the age at the time of admission: 1) younger elderly group (65–79 years) and 2) older elderly group (80–99 years). The outcomes of interest after THA and those after HA were separately compared in the two age groups.
Statistical analysis
The baseline characteristics of the patients were identified at time zero. The survival time used in the survival analyses was defined as the days from the index date to the date of death or December 31, 2015, whichever came first. The denominators for calculation of the incidence rate were defined as the survival time in days divided by 365.25. The cumulative survival probabilities and survival curves were estimated and graphed by a Kaplan-Meier method using the product-limit formula. A generalized estimating equation model with Poisson distribution and logarithmic link function was used to calculate the adjusted risk ratios (aRRs) of death with 95% confidence intervals (CIs) according to the type of surgery.
Potential confounders, including age group, gender, the level of income, Charlson comorbidity score (CCS), type of anesthesia, amount of transfusion, registered disabilities, duration of hospital stay, number of hospital beds, the year of admission due to femoral neck fracture, and past medication history (antidepressants, benzodiazepine, anti-diabetic, anti-hypertensive, non-steroidal anti-inflammatory drugs, lipid-lowering agents, COX-2 inhibitors, steroids, antiplatelet, anti-dementia, anti-Parkinson's, anti-epileptic drugs, anti-mania, and anti-psychotic agents, opioids and warfarin), were adjusted using multivariate-adjusted regression models. Each subject's number of comorbidities was assessed by diagnostic codes during the three years before the index date using Quan's ICD-10 coding algorithm of the CCS.23 The presence of disease-constituting categories in the CCS was defined by at least two outpatient visits or one admission for the primary or first secondary diagnosis. The statistical analyses were conducted using SAS software version 9.4 (SAS Institute, Cary, NC, USA). P values of < 0.05 were considered statistically significant.
Ethics statement
The design and protocol of this retrospective study were approved by the Institutional Review Board of Daejeon Eulji Medical Center (EMC-IRB No. 2019-06-018-003). Written informed consent was waived due to the nature of retrospective study.
Go to :
RESULTS
Between January 1, 2002, and December 31, 2015, a total of 10,515 femoral neck fracture patients were admitted to hospitals in South Korea. Of them, 1,292 patients who had a prior femoral neck fracture before December 31, 2004 or did not meet the enrollment criteria of minimum 3-year hip fracture-free period, were excluded. Additionally, 56 patients who were aged < 65 or > 99 years at the time of admission, 694 patients whose index date was within 1-year prior to December 31, 2015, and 2,251 patients who underwent internal fixation or non-operative treatments, were excluded. Finally, a total of 6,222 patients: 5,913 HA patients (95.03%) and 309 HA patients (4.97%), were enrolled in this study (Table 1). There were 3,228 patients: 3,015 HA patients and 213 THA patients in younger elderly group (65–79 years old), and 2,994 patients: 2,989 HA patients and 96 THA patients in older elderly group (80–99 years old).
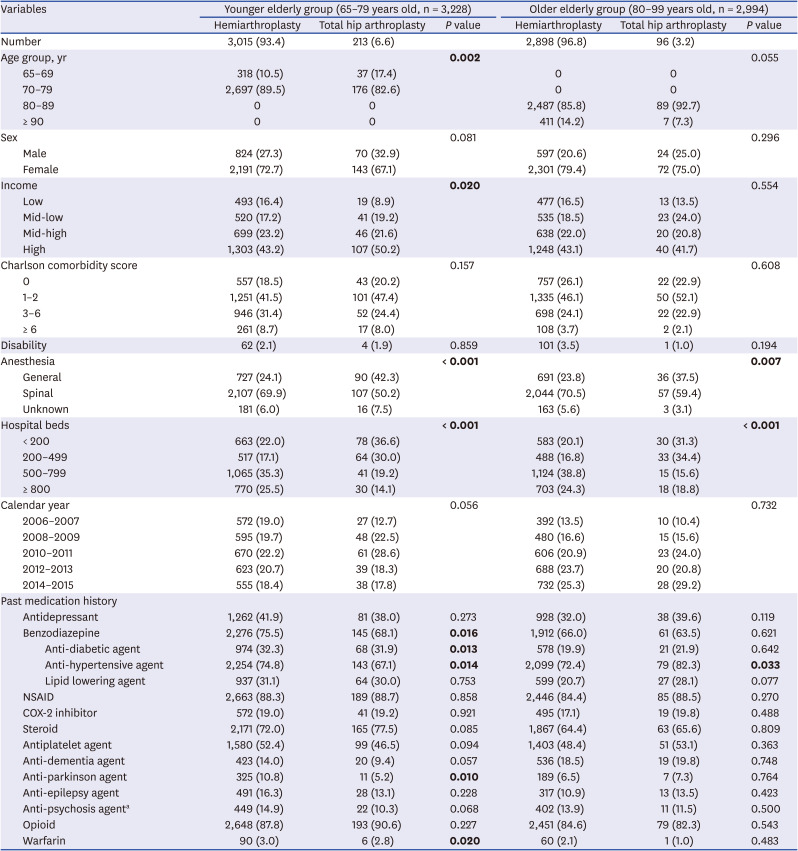
Table 1
Demographics and medication histories according to type of surgery in elderly patients with femoral neck fracture
Values are presented as number of patients (%). Bold-faced P values indicate statistically significance.
NSAIDs = non-steroidal anti-inflammatory drugs.
aTotal number of lithium users was only 6. So, they were included in antipsychotics.
![]()
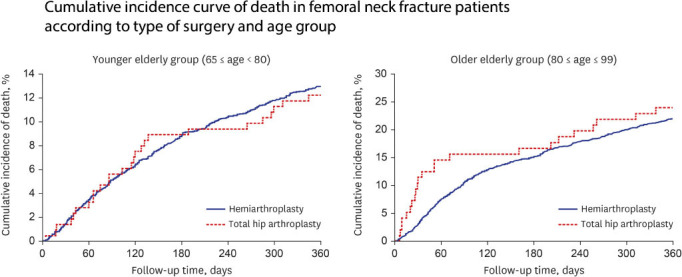
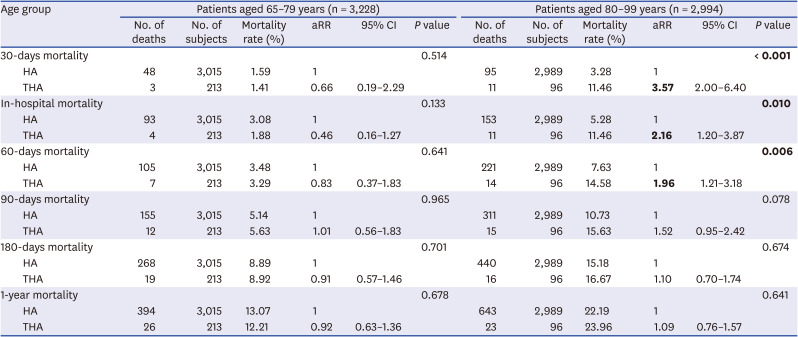
In the younger elderly group, the mortality rate was not different at any period between the THA patients and the HA patients (Table 2, Fig. 1). The mean hospital stay was 35.08 (± 37.72) days in the HA group and 27.19 (± 15.86) days in the THA group (P < 0.001). The transfusion volume was 860 (± 879.5) mL in the HA group and 1,019.7 (± 1,355.6) mL in the THA group (P = 0.092).
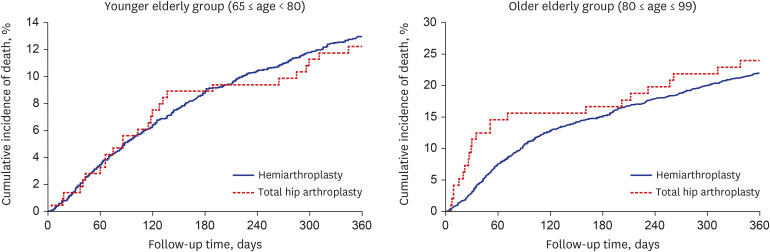 | Fig. 1Kaplan-Meier curve. Comparison of cumulative incidence of death between total hip arthroplasty group and hemiarthroplasty group in younger elderly group and older elderly group. P value for log-rank test was 0.746, 0.544, respectively.
|
Table 2
Effect of surgical type on all-cause mortality of different time frame according to age group
Bold-faced P values indicate statistically significance.
aRR = adjusted risk ratio, CI = confidence interval, HA = hemiarthroplasty, THA = total hip arthroplasty.
![]()
In older elderly group, the mortality rate was higher in the THA patients compared to the HA patients during in-hospital period and within 30- and 60-days (Table 2, Fig. 1). The mean hospital stay was 35.33 (± 36.98) days in the HA patients and 32.24 (± 31.29) days in the THA patients (P = 0.075). The transfusion volume was 978.5 (± 926.7) mL in the HA patients and 1,131.7 (± 1,053.2) mL in the THA patients (P = 0.163).
Go to :
DISCUSSION
The main finding of this study was that THA was associated with a higher mortality rate than HA in femoral neck fracture patients older than 80 years.
Life expectancy is increasing almost linearly and already surpassed the 85th year in most developed countries.17 In accordance with the increase of life expectancy, octo- and nonagenarian population is increasing. These older elderly people (aged > 80 years) have more underlying comorbidities and might have higher mortality rate compared to the younger elderly people (aged between 65–80 years).24 Thus, the safety and functional outcome of hip arthroplasties in older elderly patients should be separately evaluated from overall elderly patients aged more than 65 years. In the older elderly patients, postoperative mortality should be considered first in choosing the type because they have high comorbidities.24
In the literature, many studies compared the results of THA versus HA in elderly femoral neck fracture patients. Most studies used the age criteria of 65 years to define the elderly and did not separately assess the mortality in the older elderly patients. These studies advocated THA because it was superior to HA in terms of functional outcome and risk of reoperation, and no difference was found between THA and HA in the rates of mortality and infection. Maceroli et al.25 compared mortality rates at 30-day and 1-year postoperatively following THA and HA for displaced femoral neck fractures in 45,749 patients older than 60 years using New York's Statewide Planning and Research Cooperative System. In their study, 30-day mortality after HA was higher (8.4% vs. 5.7%; P < 0.001) as was 1-year mortality (25.9% vs. 17.8%; P < 0.001). The authors interpreted that these high mortality rates in the HA group were due to a selection bias that THAs were not performed in unhealthy patients. Bhandari et al.4 conducted a randomized controlled trial on 1,495 femoral neck fracture patients, who were 50 years of age or older and underwent either THA or HA at 80 institutions of 10 countries. The incidence of secondary procedures, functional score, quality of life, and 2-year mortality did not differ between the two treatment groups. In meta-analysis of 17 studies including 1364 patients with femoral neck fractures over 50 years of age (660 THAs and 704 HAs), Lewis et al.14 found no significant differences in the overall all-cause mortality, 30-day mortality, and 1-year mortality between the two groups. In addition, there were no differences in 30-day and 1-year mortalities in both of the < 80 and ≥ 80 age groups. It should be noted that the RCTs, which were included in their analysis, had a risk of selection bias due to small sample sizes.252627
Besides the mortality rate, the operation time, transfusion rate and the length of hospital stay should be considered in the selection of the arthroplasty type in elderly patients. In a study by Woon et al.,28 the mean hospital stay was longer in the THA group was longer (7.7 days vs. 6.7 days) and the blood transfusion rate was higher (30.4% vs. 25.7%) in the THA group than in the HA group. Bhandari et al.29 and Schneppendahl et al.30 also noted that the HA was advantageous in terms of bleeding compared to THA. In our study, the mean hospital stay of HA group was longer than that of THA group in younger elderly group, while it was not different in older elderly group. The transfusion volume was not different in both age groups.
There were limitations to this study. First, it was a retrospective review using health care claim data. Second, inherently, there might be erroneous disease coding, we could not identify specific cause of death, and functional results were not evaluated. Nevertheless, the KNHIS-Senior cohort represents the entire South Korean population over 60 years of age and had a quite low rate of follow-up loss. Femoral neck fracture patients in this study could represent all South Korean hip fracture patients older than 65 years of age. Third, among patients over 80 years of age, the number of patients who underwent THA is small compared to those who underwent HA. Thus, the difference in results depending on the presence or absence of underlying diseases is very large in people over 80 years of age. However, there was no difference in CCS in younger elderly group and older elderly group, respectively. Also, we tried to adjust for underlying disease through past medication history in statistical analysis.
In conclusion, in older elderly patients (aged 80–99 years) with femoral neck fractures, THA was associated with higher risk of in-hospital, and 30-day and 60-day mortality compared to HA. We recommend HA in these patient cohort.
Go to :
 XML Download
XML Download