

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) became a pandemic in a short time and caused serious issues for health services around the world.1 Pregnant women are also at risk of severe COVID-19 disease with the possible risk of developing serious illness and need of intensive care treatment. Although mortality among COVID-19 infected pregnant woman was reported lower than the general population,2 recent studies report an increase of unexpected maternal mortality and severe morbidity.3 COVID-19 leads to rapid onset of critical complications and may be fatal in pregnant women.45 Physiological changes in cardiopulmonary and immune systems during pregnancy predispose women to infections with respiratory viruses.6 During the H1N1 pandemic that emerged in 2009, pregnant women made up 1% of patients infected with influenza virus, however, they accounted for 5% of all H1N1 related deaths.78 Thus, the probability of developing serious disease due to COVID-19 is higher than the non-pregnant population.7
There are currently limited reports about treatment and clinical outcomes of critically ill obstetric patients infected with COVID-19 virus. The main principles of treatment for pregnant women with COVID-19 and the status of the fetus remain unclear. The aim of this study was to describe the short-term clinical/laboratory outcomes, treatment methods and mortality/morbidity status of pregnant or puerperium women diagnosed with COVID-19 followed in the intensive care unit (ICU). The secondary aim was to assess the neonatal outcomes of these patients. The outcomes include severity of pulmonary and renal disease, severity of inflammation, levels of hematologic markers, mortality rate, loss of pregnancy, fetal well-being and vertical transmission.
METHODS
This is a single-center retrospective observational study that was carried out at the ICUs of Sakarya University Hospital, Sakarya, Turkey. The medical records of pregnant and puerperal women with COVID-19 disease diagnosed by reverse transcription polymerase chain reaction that were followed up in the ICU between March 2020 and August 2021 were reviewed.
We separated the clinical data each focusing on pulmonary, laboratory and neonatal outcomes; and therapeutic interventions. Assessed pulmonary manifestations were dyspnea, tachypnea, severe cough, symptoms of respiratory disorder (oxygen saturation < 92% in room air), and necessity of invasive mechanical ventilation. Laboratory outcomes were blood leukocyte, lymphocyte, thrombocyte counts, serum D-dimer, procalcitonin, ferritin, C-reactive protein (CRP) and creatinine levels. Overall mortality rate, pregnancy-loss, delivery method (vaginal/cesarean section), delivery time, fetal birth scores, neonatal death and vertical transmission of the virus were also investigated. The findings were compared between patients that were discharged from ICU and patients who have died in ICU for the purpose of determining effectual factors that contribute to mortality.
Statistical analyses
Data were recorded in Excel (Windows) files. Statistical analyses were performed using SPSS 20.0 statistical software (IBM Corp., Armonk, NY, USA). Descriptive analysis of the variables were expressed as mean ± standard deviation in normal distribution, and parameters with abnormal distribution were expressed as median of the 25th–75th percentile (interquartile range). Categorical data are expressed as proportions. The χ2 and the Student's t-test were used for categorical and continuous variables, respectively. Fisher's exact test was applied in analyzing small samples. For continuous variables, differences between the two groups were evaluated using the Student's t-test when data were normally distributed and the Mann–Whitney U test was applied when the assumption of normality was not met. P value less than 0.05 was considered statistically significant.
RESULTS
Nineteen pregnant/puerperal women who were followed up in ICU were found eligible and included in the study. The total number of pregnant women that gave birth in our hospital was 9,656 in the study period. The number of pregnant women that were admitted to our hospital and diagnosed with COVID-19 during the study was 622. The rate of pregnant/puerperal women who required ICU care among all pregnant women with COVID-19 was found as 4.1%. The numbers have been stated in Supplementary Fig. 1 given as distributed to months.
Preeclampsia was seen in one patient, and insulin dependent diabetes was seen in two patients. The mean age of patients was 27.0 ± 3.3 years and mean body mass indexes (BMI) was 29.2 ± 3.63 in the exitus group. In the patients that were discharged from ICU, mean age was 26.18 ± 4.5 and mean BMI was 27.4 ± 3.81. There were no significant differences between the exitus and discharged patients regarding demographic values (Table 1). Mean ICU stay was 15.85 ± 13.77 days in the exitus group and 5.22 ± 2.22 days in the discharged patients. Mean ICU stay was significantly longer in the patients that have died in the ICU (P = 0.037) (Table 1).
Table 1
Data of demographic and patient characteristics at the time of admission to ICU
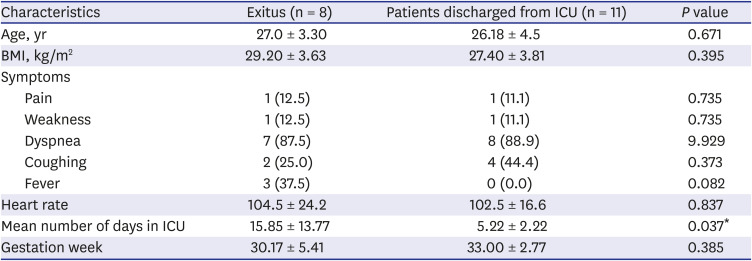
The main clinical symptom on admission to the intensive care unit was dyspnea and coughing which was present in 15 of 19 patients (78%). All patients were under supplemental oxygen therapy (8–10 L/min with reservoir O2 mask) at the time of admission to the ICU. The main indication was respiratory disorder for admission to intensive care. No significant difference was found between the exitus and discharged patients regarding the clinical symptoms (Table 1).
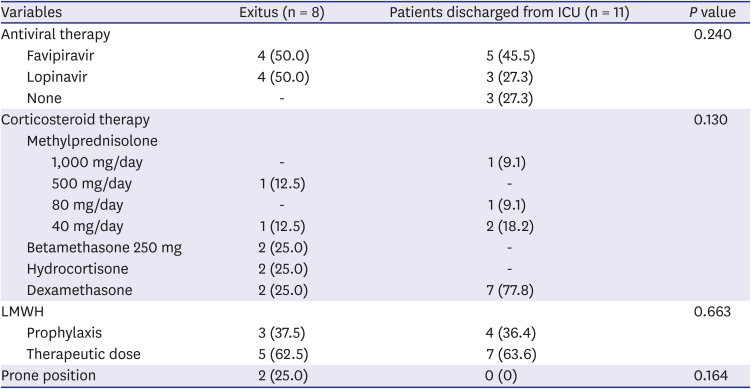
Favipiravir was administered in nine patients and lopinavir/ritonavir combination was used in seven patients. Antiviral therapy was not given to three patients. All patients used low molecular weight heparin, twelve of them received a therapeutic dose and seven of them received a prophylactic dose. Additional acetylsalicylic acid was given to two patients. All patients received corticosteroid therapy in the prenatal or postnatal period. Hemodiafiltration with cytokine filter was applied to one patient and five sessions of plasmapheresis treatment was applied. No significant difference was found regarding the administration of medical therapy between the exitus and discharged patients (Table 2).
Table 2
Data of administered medicine and therapeutic interventions
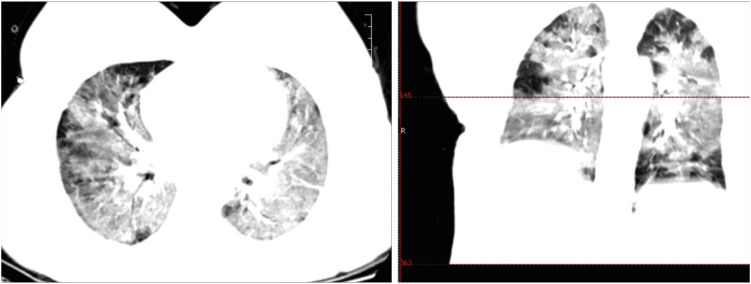
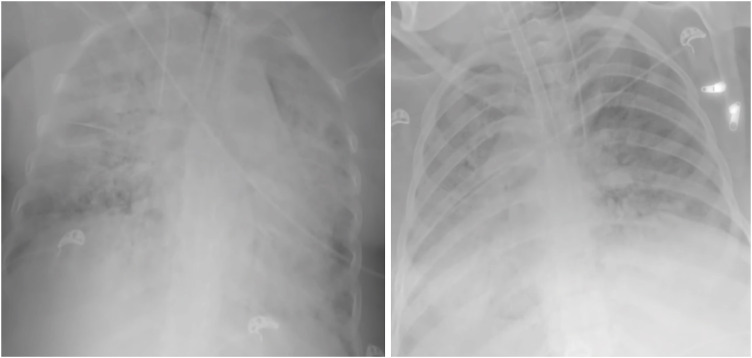
Common radiologic findings were bilateral diffuse ground glass-like infiltrations and pneumonic consolidation areas in the computerized tomography (CT) images (Fig. 1). One patient had pleural effusion in both hemi-thoraces in thoracic CT images. The x-ray images showed a diffuse bilateral infiltration and increased opacity (Fig. 2).
The main laboratory changes were increased levels of CRP which was seen in all patients (100%), increased levels of D-dimer values seen in 15 patients (78.9%), and increased levels of interleukin-6 (IL-6) seen in 16 patients (84.2%). Ferritin levels were found increased in 5 patients (26.3%) and pro-calcitonin levels increased in 5 patients (26.3%). The creatinine values were above the normal limits in 2 patients (10.5%). Lymphocyte levels decreased in 4 patients (21%). No significant difference was detected between the exitus and discharged patients in terms of mean laboratory values (Table 3).
Table 3
Data of laboratory findings
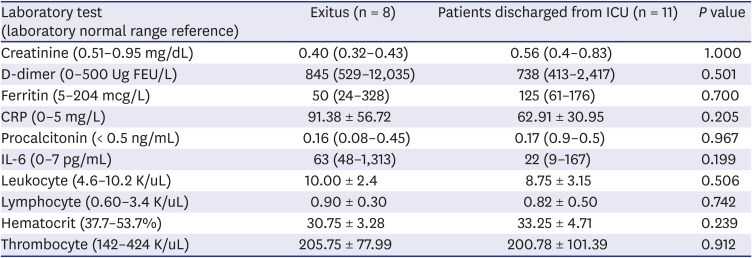
Hematologic markers of the patients also showed abnormal levels. Hematocrit levels were under normal limits in all patients. Leukocyte levels increased in 10 patients (52.6%). Lymphocyte counts were under normal limits in 5 patients (26.3%). Thrombocyte counts were under normal limits in 5 patients (26.3%). The normal limits are defined according to the limits of our institutional laboratory tests which were expressed in Table 3. The exitus and the discharged patients did not differ regarding the hematologic values.
All patients showed symptoms of pulmonary deficiency and received oxygen therapy in our cohort. Eight of the patients had severe respiratory distress who needed non-invasive positive pressure ventilation in the early course. They were intubated and mechanically ventilated in the later course of ICU stay. The rate of invasive mechanical ventilation was significantly higher among the patients that have died in the ICU (P < 0.01) (Table 4).
Table 4
Data of pulmonary outcome

One patient's fetus was not born yet during the study thus, 18 neonates were evaluated. Early delivery was seen in 11 patients (57.8%) and 7 term deliveries (42.1%) occurred without significant difference between the exitus and discharged patients. Sixteen of the patients (84.2%) underwent cesarean-section (C/S) operation with maternal indications during their follow-up between the gestational weeks 25 and 39. No difference was found between the exitus and discharged patients regarding the delivery method. One patient had an emergency bedside C/S operation in 26 weeks 3 days gestational week due to cardiac arrest during intensive care. This patient was tracheal intubated and mechanically ventilated during the cardiopulmonary resuscitation (CPR). The CPR continued for 6 minutes and 24 hours of target controlled therapeutic hypothermia was initiated immediately after the CPR. The patient was extubated after 16 days and received non-invasive ventilatory support for 5 days. On 21st day of admission the patient was intubated again and underwent percutaneous tracheostomy three days later. Unfortunately, the patient died on the 45th day of ICU admission due to ICU complications. The neonate was intubated and resuscitated after birth and admitted to the neonatal ICU without respiratory support in the following days. Eleven patients were discharged from the ICU and eight patients have died due to complications of COVID-19 in our ICU showing an overall mortality rate of 42.1%.
One neonatal death was observed who was born at 25th week with 985 grams birth weight.
Mean delivery week was 30.50 ± 5.01 in exitus group and 35.00 ± 2.64 in discharged patients. Mean birth week was significantly lower in the patients that have died in ICU (P = 0.024). Apgar score in 1st minute was also significantly lower in in the patients that have died in ICU (P = 0.042). No vertical transmission of COVID-19 was detected among neonates of our patients (Table 5).
Table 5
Data of neonatal outcome
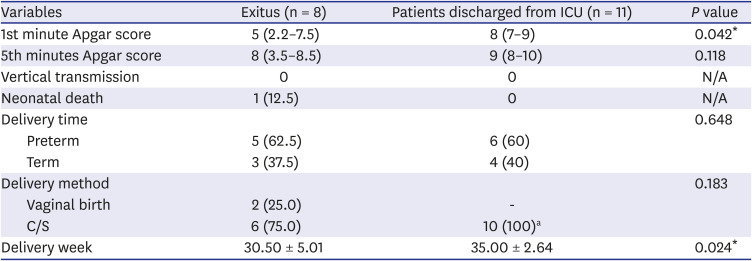
The values are expressed as number, median (interquartile range 25th–75th percentile) and percentage within group.
N/A = not applicable, C/S = cesarean-section, ICU = intensive care unit.
aSince one patient was followed up and discharged from the intensive care unit before delivery, the number of patients is 10 according to the delivery method.
*P < 0.05.
DISCUSSION
In the earlier phase of the COVID-19 pandemic, it was reported that pregnancy did not cause a significant increase in mortality and intensive care admission rates.6910 However, opposite results were reported in later studies showing an increase in the severity of the disease among pregnant and puerperal patients.31112 Recent studies have reported that pregnancy is an independent risk factor for symptomatic or severe COVID-19 disease.13 The pregnant and puerperal patients presented in this report were clustered between November 2020 and August 2021 (Supplementary Fig. 1). This time interval is consistent with the UK report showing a recent increase in ICU admission and severity of disease in pregnant COVID-19 patients.14 As the risk of household transmission in pregnancy is found ten times higher than normal population, the increase of COVID-19 disease among pregnant and puerperal patients in our institution may be attributed to household transmission.15
In many studies, it has been stated that viral diseases may lead to a cytokine storm and in some cases, cytokine storm may accompany sepsis and cause serious end-organ damage.16 Increased IL-6 levels were observed in all of our cases and it is regarded as one of the key actors of cytokine storm.16 Additionally, COVID-19 may have an impact on the cytokine profile of pregnant women varying according to pregnancy trimesters and cytokine levels seem to be correlated with disease severity.17 High production of IL-6 may be associated with adverse pregnancy outcomes such as preterm delivery.17 Significantly high IL-6 levels and high early delivery rates were found for the study group in the present study which is consistent with the present reports.
We used corticosteroids in all our patients to decrease the severity of respiratory immune response and also to increase fetal lung-maturity.18 The use of immune therapy in COVID-19 disease is still inconsistent regarding the use of corticosteroids and the use of immune-stimulating and immune-modulator drugs.19 We administered intravenous immunoglobulin (IVIG) for three post-natal patients who all died. IVIG therapy did not decrease mortality in our patients. Use of corticosteroids did not have a significant effect on mortality in our patients.
Despite all efforts around the world, antiviral or any other group of drugs that provide complete recovery in patients diagnosed with COVID-19 has not yet been identified. The antiviral and anticoagulation treatments of the patients were planned according to the National guidelines that were published and revised frequently in the pandemic period by the Turkish Ministry of Health. Lopinavir/ritonavir was used as antiviral in our pregnant patients and favipiravir was used after delivery. The use of lopinavir/ritonavir combination in pregnant human immune deficiency virus positive patients has been safely used thus, it can be used in pregnant patients diagnosed with COVID-19. Favipiravir is not recommended for use in pregnant women due to its possible teratogenic effects. Unfortunately, both recommended antiviral drugs have limited efficacy in COVID-19 patients.202122
The importance of anticoagulant use in the general population diagnosed with COVID-19 is clearly emphasized in a recently published study.23 Considering the hypercoagulation status in pregnant patients and predisposition of microthrombus formation in COVID-19 disease, it is recommended that all obstetric patients in intensive care unit with the diagnosis of COVID-19 should be given venous thromboembolism prophylaxis.24 Standard heparin or low molecular weight heparin can be used. Measurement of CRP or D-dimer can also be used as a guide to therapeutic anticoagulation treatment. The benefit of early and full dose anticoagulant use in these patients has been stated.24 Considering the national guidelines of the Ministry of Health we used low molecular weight heparin (LMWH) at therapeutic doses when there was no thrombocytopenia or bleeding. We cannot present a controlled study of the effect of anticoagulant therapy to mortality rate due to our small sample size.
Various oxygen therapy methods have been used in our patients including reservoir oxygen mask, high-flow nasal cannula, noninvasive positive-pressure ventilation and endotracheal intubation. Prone position was found technically challenging in late pregnancy, however it was used even in the third trimester with appropriate support for the gravid abdomen.25 In a recently published study, it was reported that the prone position can temporarily improve hypoxemia but does not change the course of the disease and intubation rates in patients who are spontaneously breathing and not yet have been intubated.26 In our cohort group, intermittent prone position was applied to two patients, two of whom were intubated and one of whom was spontaneously breathing with high-flow nasal cannula support. Although the sample size is not insufficient for evaluating the application of the prone position, our clinical experience indicate that the prone position does not decrease the need of intubation and mechanical ventilation.
One puerperal patient died due to end organ failure attributed to cytokine storm and sepsis. Six patients (one was puerperal and the other was pregnant) died due to severe respiratory distress syndrome. The last patient's death was attributed to ICU complications that raised after a cardiac arrest and severe sepsis. The main indicator of mortality for our patients was the need of invasive mechanical ventilation support and higher number of days hospitalized in the ICU. Limitations of our study include the limited sample size and heterogeneity of the clinical symptoms and laboratory findings.
Delivery weeks in the exitus patients were lower than the patients that have discharged from ICU. Although 1st minute Apgar scores of the neonates were lower in the exitus pregnant women, 17 of 18 neonates survived with Apgar scores of minimum 3 and maximum 10. One neonate which was born in the 26th week needed invasive mechanical ventilator support after delivery and was treated with nasal non-invasive mechanical ventilator support during the following days in the neonatal ICU. The overall incidence of cesarean delivery was high without a difference between the exitus and the discharged patients. There were no signs of vertical transmission in our cohort.
In conclusion, the authors have detected an increase in the severity of COVID-19 disease in pregnant and puerperal patients consistent with the global experience. Severe respiratory distress at the time of admission to intensive care unit was common and the need for invasive mechanical ventilation was high in the cohort. Invasive mechanical ventilation and high number of days stayed in ICU may be an indicator of mortality in pregnant and puerperal patients. Rate of cesarean section operations was high and the delivery weeks were low however, no pregnancy-loss occurred and incidence of neonatal death was low. Vertical transmission was not reported. Although there are common findings of the COVID-19 disease such as radiologic images of bilateral diffuse ground glass-like infiltrations and increased levels of inflammatory markers, our cohort showed heterogeneity regarding the laboratory test results. Thus, each pregnant/puerperal patient must be considered individually in aspect of treatment and morbidity/mortality predictors.
 XML Download
XML Download