

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Preterm birth, defined as “birth between 20 and 37 weeks of gestation”, is a major contributor to disease burden for infants and children in the world.1234 One of every 10 newborns were preterm babies in the United States during 2003–2012, i.e., 5,042,982 (12.2%) of 41,206,315 births.1 The share of preterm births increased rapidly from 4.3% to 6.0% in Korea during 2001–2010.2 On a global level, 15 million newborns are preterm babies every year and this is responsible for 965,000 neonatal deaths and 125,000 deaths among children aged 1–5 years. Three quarters of this mortality is estimated to be avoidable with cost-effective interventions.34 Independent suggestions have been made on a positive association between gastroesophageal reflux disease (GERD) and periodontitis and on a positive linkage between periodontitis and preterm birth (PTB).567891011 Likewise, it would be natural to expect a positive relationship between GERD and preterm birth. But little endeavor has been made in this direction.
One previous study adopted machine learning and general hospital data for testing an association among spontaneous preterm labor and birth (SPLB), GERD and periodontitis.12 Data for this study came from 731 obstetric patients in Anam Hospital (Seoul, Korea) during January 5, 1995–August 28, 2018. Random forest variable importance, the contribution of a certain variable for the performance of the random forest, was adopted for finding main predictors of SPLB and testing its associations with GERD and periodontitis. Based on random forest variable importance, main predictors of SPLB were age, education, GERD, Helicobacter pylori, upper gastrointestinal tract symptoms, various types of body mass index (BMI), diabetes and hypertension, parity, pelvic inflammatory disease, and medication such as progesterone, calcium channel blocker. Periodontitis ranked twenty second. It was concluded that SPLB had a stronger association with GERD than with periodontitis and, for preventing SPLB, preventive measures for hypertensive disorder, GERD and diabetes mellitus would be very important together with appropriate BMI management and effective progesterone and calcium-channel-blocker medications.
However, the data in this previous study was relatively small (731 participants). Machine learning analysis with population data is expected to bring more conclusive evidence on the association among the three diseases above. In this context, this study uses machine learning and population data for testing the following hypotheses:
METHODS
Participants
Retrospective cohort data came from Korea National Health Insurance Service claims data for all women in Korea who aged 25–40 years and gave births for the first time as singleton pregnancy during 2015–2017 (405,586 women). The dependent variable was preterm labor and birth during 2015–2017 (birth between 20 weeks and 0 day and 36 weeks and 6 days of gestation). Four types of preterm labor and birth were defined based on International Classification of Diseases, 10th Revision (ICD-10) code: 1) PTB 1: preterm birth with premature rupture of membranes (PROM) only; 2) PTB 2: preterm labor and birth without PROM; 3) PTB 3: PTB 1 or PTB 2; 4) PTB 4: PTB 3 or other indicated preterm birth (Supplementary Table 1). This variable was coded as “no” vs. “yes”. And the following 29 independent variables were included in this study: 1) GERD (coded as no vs. yes) for each of the years 2002–2014, i.e., GERD_2002, …, GERD_2014; 2) periodontitis (coded as no vs. yes) for each of the years 2002–2014, i.e, Periodontitis_2002, …, Periodontitis_2014; 3) age (year) in 2014; 4) socioeconomic status in 2014 measured by an insurance fee with the range of 1 (the highest group) to 20 (the lowest group); and 5) region (city) (coded as no vs. yes) in 2014. GERD (GERD_2002, …, GERD_2014) and periodontitis (Periodontitis_2002, …, Periodontitis_2014) were screened from ICD-10 codes (Supplementary Table 1).
Analysis
Logistic regression, the random forest and the artificial neural network were adopted and compared for predicting preterm birth.1213 Data on 402,092 observations with full information were split into training and validation sets with a 70:30 ratio (281,464 vs. 120,628 observations). Accuracy, a ratio of correct predictions among 120,628 observations, was used as a standard for validating the models. Random forest variable importance, the contribution of a certain variable for the performance of the random forest, was used for finding main predictors of preterm birth and testing its associations with GERD and periodontitis. R-Studio 1.3.959 (R-Studio Inc., Boston, MA, USA) was employed for the analysis during September 2019–May 2020.
RESULTS
Descriptive statistics are shown for participants' preterm birth and its categorical predictors in Table 1. Among 405,586 participants, 21,961 (5.41%), 9,034 (2.23%), 28,054 (6.92%) and 29,167 (7.19%) belonged to PTB 1, 2, 3 and 4, respectively. Among the participants, 376,384 (92.8%) resided in urban areas. Indeed, the average age and socioeconomic status of the participants were 31 and 11, respectively. During 2002–2014, the prevalence of GERD was consistently higher for those with preterm birth than for those without the outcome: 10.54%, 10.33%, 10.50%, 10.47% and 7.90% for PTB 1, PTB 2, PTB 3, PTB 4 and the normal in 2014, respectively; and 0.79%, 0.80%, 0.78%, 0.79% and 0.62% for PTB 1, PTB 2, PTB 3, PTB 4 and the normal in 2002, respectively (Table 2). A similar pattern was found for the prevalence of periodontitis: 0.09%, 0.09%, 0.08%, 0.08% and 0.05% for PTB 1, PTB 2, PTB 3, PTB 4 and the normal in 2014, respectively; and 0.07%, 0.07%, 0.07%, 0.07% and 0.04% for PTB 1, PTB 2, PTB 3, PTB 4 and the normal in 2002, respectively.
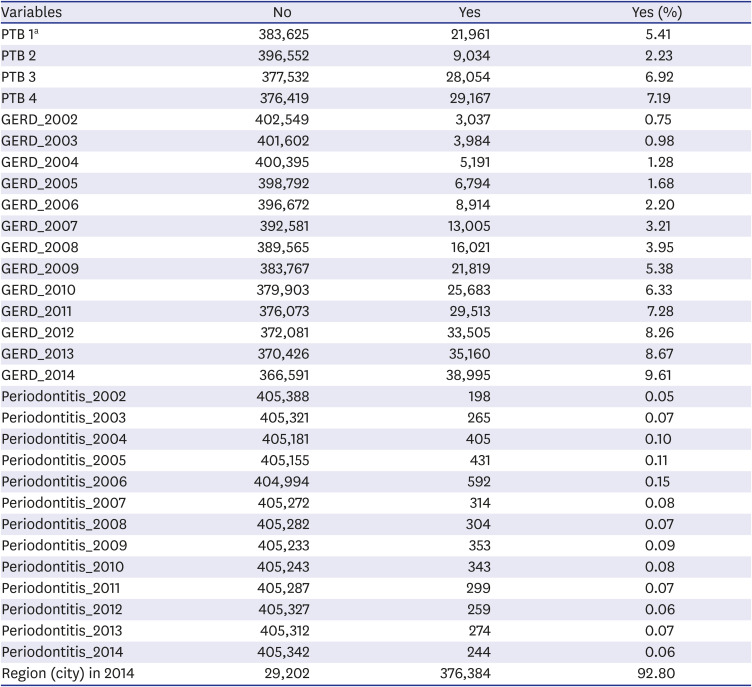
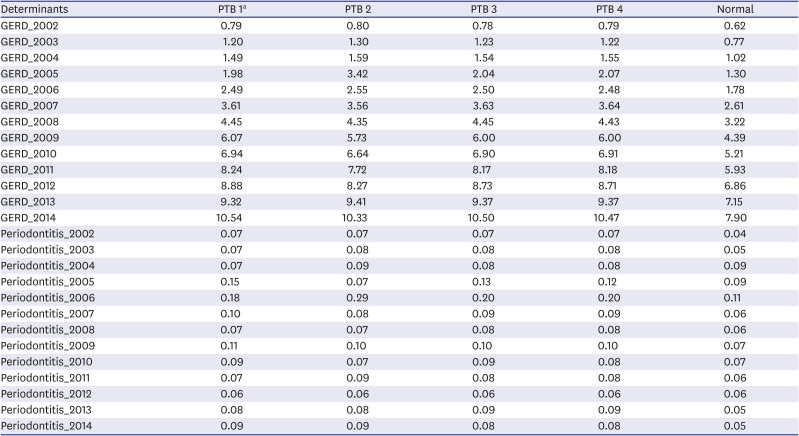
Table 1
Descriptive statistics on PTB and its categorical predictors
![]()
Table 2
Percentages of GERD and periodontitis during 2002–2014
![]()
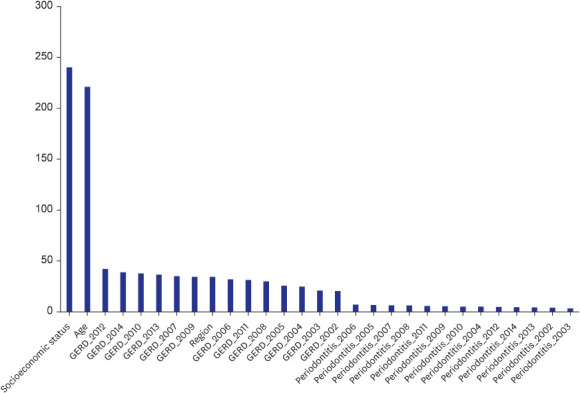
The accuracy of the random forest was similar with those of logistic regression and the artificial neural network (94.56%, 97.79%, 93.07% and 92.80% for PTB 1, PTB 2, PTB 3 and PTB 4 in Table 3, respectively). Based on random forest variable importance in Fig. 1, main predictors of preterm birth during 2015–2017 were socioeconomic status in 2014 (240.28), age in 2014 (221.13), GERD for the years 2012 (42.24), 2014 (38.86), 2010 (37.76), 2013 (36.64), 2007 (35.01) and 2009 (34.39), region in 2014 (34.36) and GERD for the year 2006 (31.98). These values were the average for PTB 1, PTB 2, PTB 3 and PTB 4 (Supplementary Fig. 1 for each of PTB 1, PTB 2, PTB 3 and PTB 4). Top-10 predictors for PTB 2 were socioeconomic status in 2014 (121.02), age in 2014 (112.27), GERD for the years 2012 (21.31), 2010 (19.61), 2011 (19.53), 2014 (19.26) and 2009 (19.22), region in 2014 (16.58) and GERD for the years 2013 (16.35) and 2006 (15.80). Likewise, top-10 predictors for PTB 4 were socioeconomic status in 2014 (306.92), age in 2014 (294.18), GERD for the years 2012 (56.84), 2014 (49.77), 2010 (48.33) and 2013 (47.89), region in 2014 (46.74) and GERD for the years 2007 (46.47), 2008 (42.78) and 2009 (41.78). The importance rankings of periodontitis were relatively low across board.
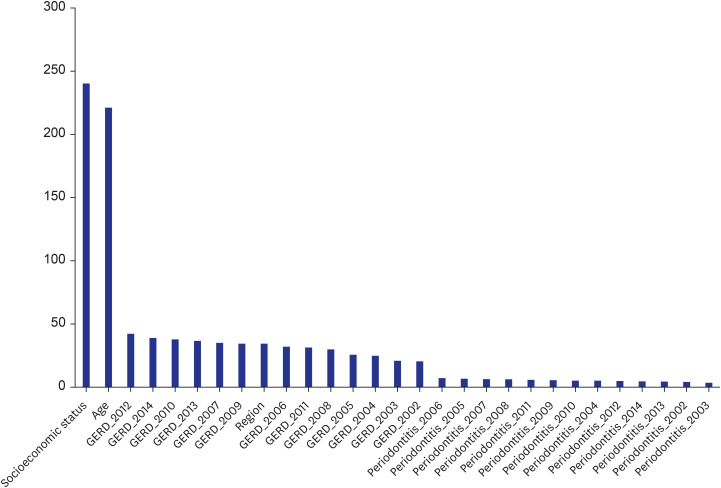

Fig. 1
Variable importance from the random forest: average for PTB 1, PTB 2, PTB 3 and PTB 4.
PTB = preterm birth, GERD = gastroesophageal reflux disease.
![]()
Table 3
Model performance
PTB = preterm birth, AUC = area under the receiver-operating-characteristic curve.
aPTB during 2015–2017.
![]()
The results of logistic regression are shown in Tables 4 and 5. The odds of PTB 2 (or PTB 4) will increase by 6.6% (or 3.1%) if age increases by 1 year. The odds of PTB 4 will go up by 3.2% if socioeconomic status go down by 10 units, e.g., from 1 (the highest group) to 10 (the middle group). The odds of PTB 4 is greater by 8.0% for those with GERD in 2011 than those without it. Likewise, the odds of PTB 4 is higher by 7.9% for those with GERD in 2009 than those without it. Logistic regression requires an unrealistic assumption of ceteris paribus, i.e., “all the other variables staying constant”. In this context, the results of logistic regression would serve as supplementary information to random forest variable importance. According to the findings of this study above, 1) the hypothesis cannot be rejected on a positive association between preterm birth and GERD (hypothesis 1) while 2) the hypothesis can be rejected on a positive association between preterm birth and periodontitis (hypothesis 2).
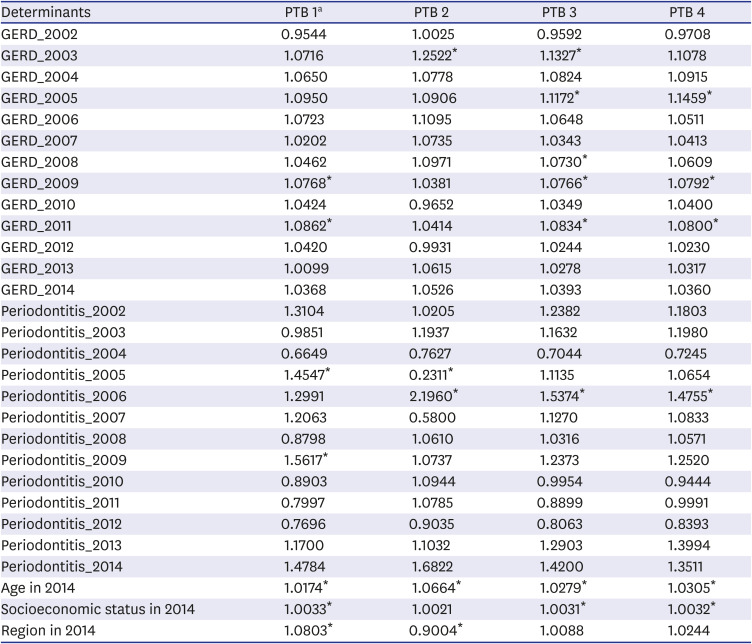
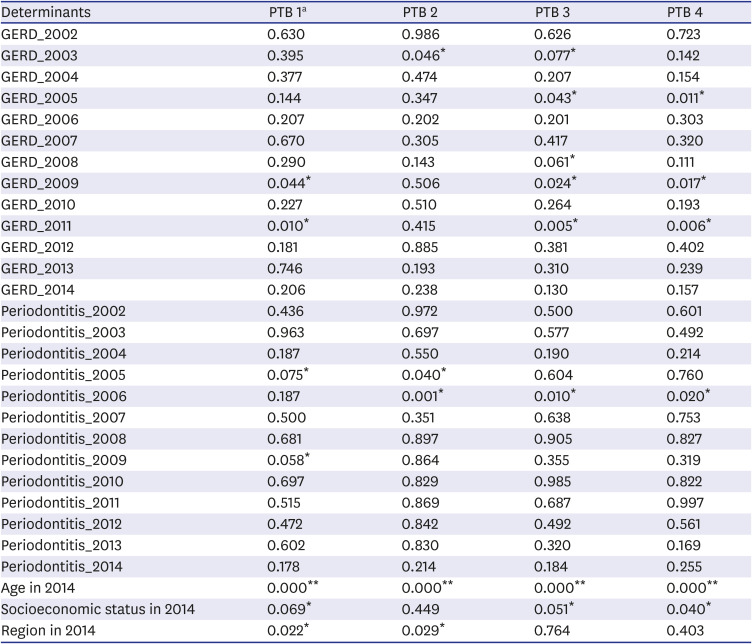
Table 4
Coefficients of predictors from logistic regression for each type of PTB
![]()
Table 5
P values: coefficients of predictors from logistic regression for each type of PTB
PTB = preterm birth, GERD = gastroesophageal reflux disease.
aPTB during 2015–2017.
*P < 0.100; **P < 0.001.
![]()
DISCUSSION
In summary, based on random forest variable importance, main predictors of preterm birth during 2015–2017 were socioeconomic status in 2014, age in 2014, GERD for the years 2012, 2014, 2010, 2013, 2007 and 2009, region (city) in 2014 and GERD for the year 2006. The importance rankings of periodontitis were relatively low.
According to the findings above, this study draws the following clinical implications. Firstly, the results of this study promote active counseling on GERD for effective prenatal care. Independent suggestions have been made on a positive association between GERD and periodontitis1415 and on a positive linkage between periodontitis and preterm birth.6 Likewise, it would be natural to expect a positive relationship between GERD and preterm birth. This study supports this expectation given the high importance rankings of GERD from the random forest in this study: GERD for the years 2012, 2014, 2010, 2013, 2007, 2009 and 2006 ranked within the top ten. GERD is reported to cause cytokine-triggered inflammation,161718 which is expected to cause uterine contraction and preterm birth.19202122 As a matter of fact, GERD symptoms such as nausea and vomiting are quite general but usually ignored among pregnant women. Based on the relatively small data (731 participants), the previous study drew a clinical implication that the promotion of active counseling on GERD is vital for effective prenatal care.12 This study confirms this clinical implication, using the population data (405,586 women). Secondly, the findings of this study highlight the importance of socioeconomic status as a main predictor of preterm birth. A few studies indicate that low socioeconomic status is a risk factor for preterm birth: education below high school graduation for 731 Korean women in a single-center retrospective study (odds ratio, 1.660),12 income below $1,000 for 2,645 Korean women in a multi-center prospective study (odds ratio, 5.1)23 and employment in heavy work for 7,634 Italian women in a multi-center retrospective study (odds ratio, 1.9).24 Socioeconomic status was measured by an insurance fee with the range of 1 (the highest group) to 20 (the lowest group) in this study and lower socioeconomic status was a risk factor for preterm birth (odds ratio, 1.0032: The odds of PTB 4 will go up by 3.2% if socioeconomic status go down by 10 units, e.g., from 1 [the highest group] to 10 [the middle group]). This result is consistent with the existing literature and, it would be needed for preventing preterm birth to promote socioeconomic status for pregnant women.
To our best knowledge, this study is the first attempt to use machine learning and population data for finding main predictors of preterm birth and evaluating its association with GERD and periodontitis. The terms “artificial intelligence” and “machine learning” have garnered great attention on a global scale in the past decades and a vast improvement of computing power has been a main factor for the unprecedented performance and popularity of these cutting-edge approaches. This study will be a good starting point in this direction to find main predictors of preterm birth and draw effective implications for its prevention and management. However, this study still had some limitations. Firstly, this study did not examine possible mediating effects among variables. Secondly, this study adopted the binary category of preterm birth as no vs. yes. But preterm birth can have multiple categories and it will be a good topic for future study to compare different predictors for various categories of preterm birth. Thirdly, it was not the scope of this study to explore and evaluate various pathways between GERD and preterm birth. Little literature is available and more effort is needed in this direction. Fourthly, GERD was screened from ICD-10 codes in this study. Additional validation based on endoscopic finding and motility testing are expected to improve external validity for this line of research. Fifthly, this study excluded education, employment, upper gastrointestinal tract symptoms, Helicobacter pylori, pelvic inflammatory disease, various types of BMI, diabetes and hypertension, parity and medication such as progesterone, calcium channel blocker. Sixthly, the area under the receiver-operating-characteristic curves of this study belonged to the range of 0.51–0.57 and they were not high enough to serve as diagnostic tests. Further improvement is needed and one solution would be to extend this study to consider various information on health status and medication history. Finally, further investigations of single vs. multiple gestation, first vs. recurrent preterm birth, would deliver more insights and more detailed clinical implications.2526
In conclusion, preterm birth has a stronger association with GERD than with periodontitis. For the prevention of preterm birth, preventive measures for GERD would be essential together with the improvement of socioeconomic status for pregnant women. Especially, it would be vital to promote active counseling for general GERD symptoms (neglected by pregnant women).
 XML Download
XML Download