

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of pediatric heart transplantation has been steadily increasing, and the survival rate has improved impressively despite diversity in recipient heart disease and limited resources in pediatric heart donation. Improvements in surgical techniques, the use of immunosuppressant agents post-transplantation, and the early detection of graft failure have all significantly contributed to this improvement in pediatric heart transplantation outcome. Considering the severely limited availability of suitable donor hearts, the first step towards achieving the best outcome is reducing the waiting list mortality. Pediatric waiting list mortality rates are reported as 5–32% and also vary among countries, regions, and institutions.123 Significant risk factors while on the list include the use of extracorporeal membrane oxygenation (ECMO) or ventilator support, the presence of congenital heart disease (CHD), a patient body weight < 3 kg, nonwhite race, United Network of Organ Sharing (UNOS) status 1A, and the need for dialysis.14 However, there has been a significant decrease in waiting list mortality due to changes in the donor allocation system and the use of ventricle assist devices (VAD) as a bridge to transplantation.56 In Korea, the first successful pediatric heart transplantation was performed in 1997, and 10–15 cases are added annually according to the Korean Network of Organ Sharing (KONOS).7 Recently, the use of a VAD has been available for pediatric patients, so a much better outcome can be expected in pediatric heart transplantation in Korea. However, no national studies about the waiting list mortality of pediatric heart transplantation patients before the use of VAD in Korea have been conducted; therefore, we collected and analyzed the data from most of the centers. The purposes of this study were to investigate the waiting list mortality rate of pediatric heart transplantation in Korea, the causes of mortality, and the median survival periods as well as any risk factors.
METHODS
Study population
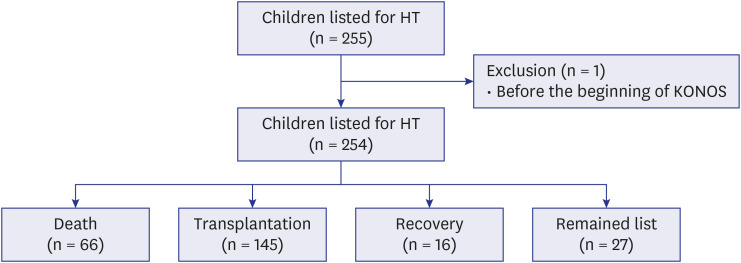
All pediatric patients younger than 18 years old who were listed for heart transplantation at three major hospitals (Samsung Medical Center, Asan Medical Center, and Seoul National University Children’s Hospital) in Korea between January 2000 and January 2020 were identified retrospectively through KONOS. Each hospital provided the total number of patients who were listed for heart transplantation along with the demographic and clinical information on patients who were listed for heart transplantation but died while waiting to determine the waiting list mortality rate. The demographic and clinical variables were defined at the time the patient was listed for heart transplantation. We collected a variety of clinical data from patients who died, including age, sex, body weight, body surface area, blood type, the use of mechanical ventilator, the time between diagnosis of heart failure and listing for heart transplantation, the use of dialysis, initial KONOS level, cardiac diagnosis, cause of death, date of death, and the use of ECMO. The patients who died were followed up from the time they were listed for heart transplantation until their date of death. All patients who were listed for heart transplantation before the advent of KONOS were excluded. Of the 255 pediatric patients who were listed for heart transplantation, 1 patient was excluded because the time of listing preceded the advent of KONOS. The initial KONOS level that was defined at the time of initial listing for heart transplantation was classified into levels 0, 1, 2, and 3 depending on the patients' clinical status and the urgency for heart transplantation. KONOS level 0 was defined as the condition that require applying ECMO, mechanical ventilator due to heart failure, mechanical circulatory device due to ventricular arrhythmias or VAD with significant complications. KONOS level 1 was defined as the condition that require artificial heart, VAD, IABP or continuous administration of intravenous inotropic agents for more than 4 weeks and so on. Of the final 254 pediatric patients listed for heart transplantation, 145 patients received a transplant during the study period, and 16 patients were removed from the waiting list due to recovery of their underlying disease. Twenty-seven patients remained on the waiting list on the last day of observation, and 66 patients had died (Fig. 1). These 66 patients were considered as the patient group. We further investigated this group to confirm the causes of waiting list mortality and the median survival periods depending on variable risk factors
Statistical analysis
The data were analyzed using IBM® SPSS® for Windows software, version 25.0 (IBM Corporation, Armonk, NY, USA). The statistics are presented as the median and number (percent). The survival period on the waiting list was estimated using the Kaplan-Meier method. The univariate relationships between patient characteristics and waiting list mortality were evaluated with the log-rank test. The multivariate analysis was performed using the Cox proportional hazards model. The risk factors associated with mortality were considered statistically significant when the P value was < 0.05.
RESULTS
Characteristics of the patient group
The waiting list mortality rate was 26%. In the patient group, 38 (57.6%) patients were male. The median body weight and body surface area were 9.2 kg and 0.45 m2 respectively. A total of 51 (77.3%) patients were supported by mechanical ventilator care. The interval between the diagnosis of heart failure and listing for transplantation was 68 days. Less than half of the patients who died during waiting for transplantation were needed on dialysis (n = 23, 34.8%). We divided the patient group into four subgroups depending on patient age. Most patients (n = 30; 45.5%) were included in the group < 1 year of age. The progression of heart failure was the leading cause of mortality (n = 24; 36.3%), followed by multi-organ failure in organs other than the heart (n = 18; 27.2%), (Table 1).
Table 1
The characteristics of patients who died while awaiting heart transplantation
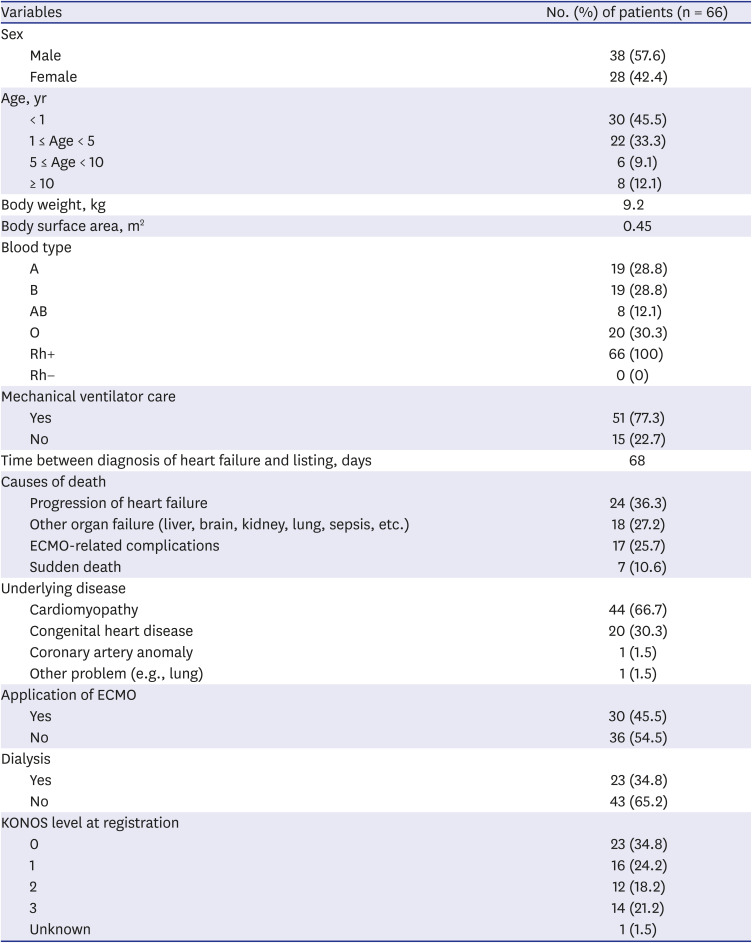
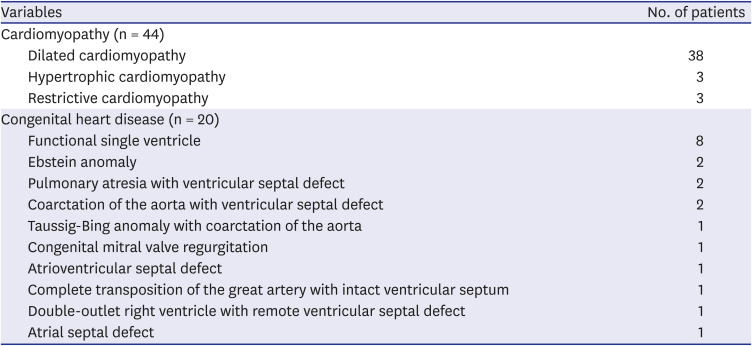
Cardiomyopathy (n = 44; 66.7%) was the leading reason that patients were listed for heart transplantation, and dilated cardiomyopathy (n = 38) also accounted for a majority. The second most common cause of heart transplantation candidate listing was CHD (n = 20; 30.3%). Among the CHD patients, a single functional ventricle (n = 8) was the most common abnormality (Table 2). A little less than half of the patients received ECMO (n = 30; 45.5%). Most patients were included KONOS level 0 (n = 23; 34.8%), and only 1 (1.5%) patient was not classified into any group due to lack of information (Table 1).
Table 2
The detailed classification of the cardiomyopathy and congenital heart disease patients who died while awaiting heart transplantation
A comparison of survival times depending on various risk factors in the patient group
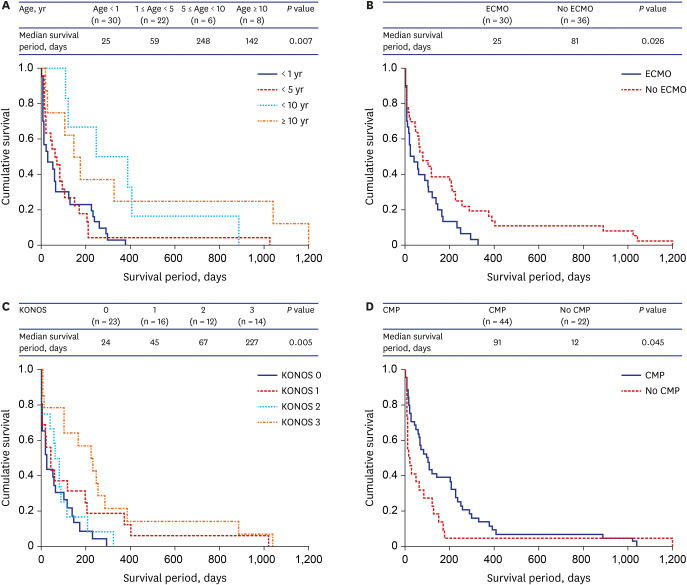
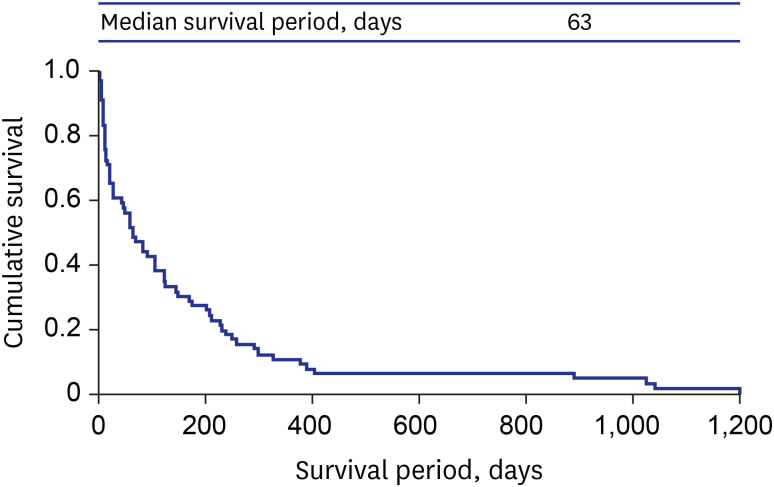
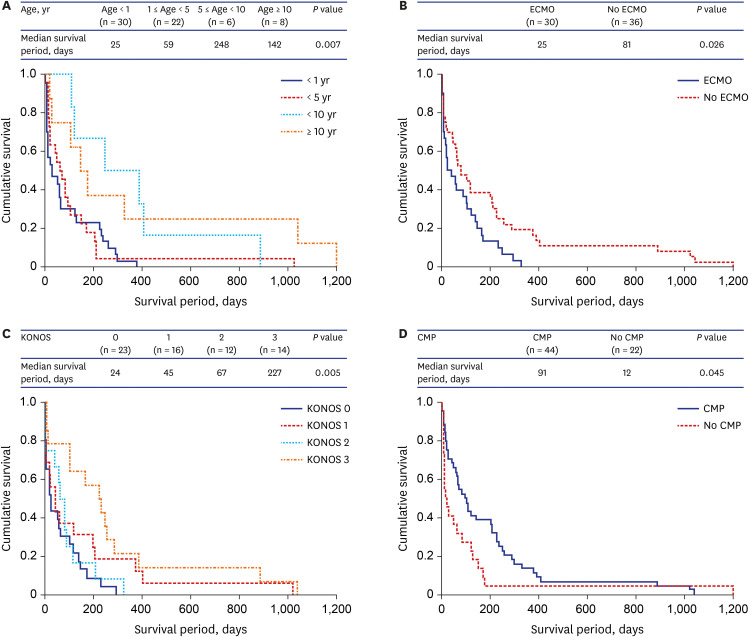
In this study, a 63-day median survival period was shown in the patient group of 66 patients (Fig. 2). Fig. 3A–D contain the Kaplan-Meier cumulative survival curve and the median survival periods according to the various risk factors. The Kaplan-Meier curve indicated worse survival periods for younger patients. In the groups with patients under 1 year old and between 1 year and 5 years of age, the survival periods tended to be shorter compared to the other groups. The shortest median survival times were seen for patients < 1 year old (Fig. 3A). This difference was statistically significant among the different age groups (P = 0.007). The Kaplan-Meier curve showed worse survival periods when the patient was supported by ECMO (P = 0.026; Fig. 3B). Shorter median survival periods were associated with a higher KONOS level, which reflects the serious clinical status of these patients. A median survival period of 24 days was seen when the patient was classified as KONOS level 0 (P = 0.005; Fig. 3C). We compared the Kaplan-Meier survival curves between the cardiomyopathy and non-cardiomyopathy groups. Because CHD was present in almost all patients in the non-cardiomyopathy group, this group was actually considered to be a group of patients that represented CHD. The Kaplan-Meier curve showed markedly worse survival periods when for patients with CHD. Only 12 days of median survival were expected in the non-cardiomyopathy group (P = 0.045; Fig. 3D). The difference was not statistically significant among the different blood type groups (P = 0.614). The Kaplan-Meier curve showed no different survival curve between the patient with and without mechanical ventilator care. (P = 0.079). Finally, we compared the Kaplan-Meier survival curves according to the presence or absence of dialysis support. There was no significant difference of survival curve between them. (P = 0.213).
Risk factors associated with waiting list mortality
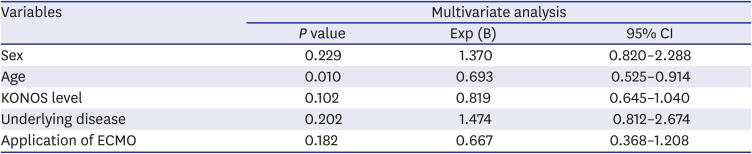
Even though a univariate analysis identified sex, age, initial KONOS level, underlying cardiac disease, and the application of ECMO as risk factors for waiting list mortality, age was the only statistically significant risk factor upon multivariate analysis. The mortality rate tended to decrease as the patient age increased (Table 3).
Table 3
The multivariate analyses of the patient group produced using a Cox proportional analysis
DISCUSSION
In this study, a 26% waiting list mortality rate and a 63-day median survival period without the use of VAD were demonstrated, which were inferior outcomes compared to those reported in the United States (US; 17%).1 Other studies have reported that CHD, bridging with ECMO, a younger age, and a higher KONOS level, ventilator support and dialysis support are risk factors associated with a shorter survival period.189101112 Previous study reported that the blood type is no longer a risk factor of death while awaiting a heart transplant.4 In our study, blood type also was not a significant risk factor associated with mortality. However, a multivariate analysis in this study revealed that only the patient age had a significant association with waiting list mortality. In pediatric heart transplantation, long-term survival has been a main outcome for a long time. However, reducing waiting list mortality and maintaining the recipient's condition until the time of transplantation should also be emphasized. Even with improvements in the organ allocation system in the US, Almond et al.1 reported that pediatric waiting list mortality remained unacceptably high.
In our study, the survival rate during the waiting period for heart transplantation was poor for patients who received mechanical circulatory support (such as ECMO). In addition, pediatric patients who were initially listed as KONOS levels 0 or 1 had poor survival periods than patients at other levels. The median time interval between the diagnosis of heart failure and the day of listing in our study was 68 days. Therefore, the patient's clinical condition at registration as well as any circulatory deterioration during the waiting period might lead to the poorest outcomes. And it is important that the timely transplant registration of high-risk children should be emphasized. The main reasons for death while waiting for heart transplantation were due to complications related to ECMO and combined other multi-organ failures. Therefore, adequate medical support for other organs should be provided to reduce waiting list mortality. Patients who received ECMO ironically had both a higher probability of heart transplantation but also a greater risk of waiting list mortality, which is also true in Korea. Our patients experienced bleeding, thromboembolic complications, or other device-related issues that lead to death before transplantation.
Our study period was equated to Era 1 in the US, which took place from 1999–2004 when there was no pediatric VAD availability. We expect an improvement in the waiting list mortality of Era 2 (pediatric VAD). Zafar et al.6 reported that even with an increase in the number of children listed with a UNOS status 1A, there has been a greater than 50% reduction in waiting list mortality in the VAD era. Another review demonstrated that the 28% waiting list mortality in Era 1 for patients who received ECMO decreased to 13% with the availability of VAD in Era 2.13 However, patients with a low body weight and those with CHD were still at higher risk of waiting list mortality regardless of era.6 Currently, the use of ECMO as a bridge to heart transplantation is minimal; only 4% of all listed patients in the US receive ECMO, and we are aware that the period of VAD support in patients as a bridge to pediatric heart transplantation is not a risk factor for mortality.14
In contrast, the expansion of donor heart criteria and the increased use of limited donor hearts might also have contributed to a reduction in the waiting list mortality rate.15 ABO-incompatible donor heart transplantation has been successfully performed in young infants.16 In adult heart transplantations, donation after circulatory death (DCD) is becoming widely accepted and prevalent in Europe. A case report has also described a child who underwent successful heart transplantation after DCD.17
This study had several limitations. Although it was a multicenter study of three major centers, our study did not include all pediatric patients listed for heart transplantation in Korea. The incidence of pediatric heart transplantation has recently been increasing in Korea. Therefore, our study included only a small number of patients, which might explain why our results were slightly different from those of other large-scale studies. The reasons for mortality in our patients might be quite complicated, and the main cause of mortality was not always easy to define based solely on patient medical records.
In conclusion, although this study was conducted before the use of pediatric VAD, the waiting list mortality rate was high compared to that reported by other studies carried out in other countries. The different survival periods according to age, cardiac diagnosis, the use of ECMO, and the initial KONOS level were proven by univariate analysis; however, age was the only significant factor associated with waiting list mortality in pediatric patients based upon our multivariate analysis. Therefore, we expect that this study's findings may impact our timing of heart transplantation listings and lead to a revision of the organ allocation system, especially in pediatric patients.
 XML Download
XML Download