

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Inflammatory bowel disease (IBD), which includes Crohn's disease (CD) and ulcerative colitis (UC), are chronic, relapsing inflammatory disorders of the intestinal tract.1 IBD is systemic in nature, and extraintestinal manifestations (EIMs) are also commonly experienced by patients, with a reported incidence of 21–41%.23 However, studies on pediatric EIMs are few, and limited research has shown that from one-quarter to almost one-half of pediatric patients with IBD experience at least 1 EIM at the time of diagnosis.456
EIMs are known to be more common in CD than UC,3 and usually correlate with disease activity, except for some exceptions.7 The pathogenesis of EIMs is poorly understood, and it has been speculated that several immune mechanisms are involved.8 The underlying immune dysregulation of IBD may target the entire body and not only the gastrointestinal (GI) tract. Although it is known that EIMs commonly occur in patients with pediatric-onset IBD, and it is presumed that the pathogenesis is closely related to the same mechanisms involved with the GI tract, few researchers have examined EIM rates and relationships to other disease-related factors in the clinical setting. Recently, the incidence and prevalence of pediatric IBD is increasing worldwide, including that of Korea.910 However, limited data exists for EIMs associated with pediatric IBD in Korea.
Therefore, we aimed to investigate the clinical features and factors associated with EIM development in Korean children and adolescents with IBD.
Go to : 
METHODS
Patients and study design
This study was a multicenter, retrospective study conducted from June 2010 to July 2017 at the Department of Pediatrics of four medical centers in the Daegu-Gyeongbuk region of Korea, which are the only tertiary referral centers for pediatric patients with IBD in the region: Kyungpook National University Children's Hospital, Keimyung University Dongsan Medical Center, Yeungnam University Medical Center, and Daegu Catholic University Medical Center. We analyzed the results of follow-up for the patients diagnosed within the study period.
This study included pediatric patients with IBD diagnosed before the age of 18 years. Diagnosis of IBD had been made in accordance with the revised Porto criteria of the European Society for Paediatric Gastroenterology Hepatology and Nutrition.11 Disease phenotype at diagnosis was classified according to the Paris classification.12 Clinicodemographics including sex, diagnosis age, growth indicators at diagnosis, previous history of EIMs, disease activity scores, laboratory test results, and medication were investigated for all the patients with available data at baseline and at EIM development. Physical examination, clinical activity scores, and laboratory tests, including complete blood cell counts with differential counts, chemistry profiles, erythrocyte sedimentation rate (ESR) and C-reactive protein levels, had been conducted at baseline and every regular visit, which had occurred in intervals of 1 week to 3 months or was an emergency visit. For the clinical activity scores at diagnosis and during follow-up, Pediatric Crohn's Disease Activity Index (PCDAI) had been checked in patients with CD,1314 and Pediatric Ulcerative Colitis Activity Index (PUCAI) in patients with UC.15
EIMs investigated for this study included ankylosing spondylitis, chronic active hepatitis, pancreatitis, nephritis/nephrotic syndrome, aphthous stomatitis, primary sclerosing cholangitis, arthralgia, arthritis, erythema nodosum, pyoderma gangrenosum, and iritis/uveitis. We also investigated EIMs involving the vascular, pulmonary, cardiac, and neurological systems. We did not include other potential EIMs related to nutrient deficiencies from malabsorption, such as osteopenia and osteoporosis; we also excluded fever of unknown origin and iatrogenic EIMs, such as drug-induced bone marrow suppression and corticosteroid-associated myopathy. We examined the EIM rates and the associations between EIMs and variables, and the possible association between a specific medical therapy and EIM development.
Statistical analysis
Student's t-test and Wilcoxon's rank-sum test were used for statistical comparison of continuous variables between groups and the χ2 test or Fisher's exact test was used for comparison of categorical variables. Comparative data for continuous variables are expressed as medians with interquartile range (IQR) or means with standard deviation. Univariate and multivariate logistic regression analyses were performed to examine the association of the development of EIMs with variables. Univariate logistic regression analysis was performed to investigate the crude odds ratio (OR) for each variable, and those with a P value of < 0.1 in the univariate analysis were included in the multivariate analysis. The results are expressed as adjusted ORs with 95% confidence intervals (CIs). Statistical significance was defined as a P value of < 0.05. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital and all other participating centers, and informed consent was waived due to the retrospective nature of this study (IRB No. 2018-03-023).
Go to :
RESULTS
Baseline characteristics of the patients
A total 172 patients were included in this study of whom 137 (79.7%) were CD, and 35 (20.3%) were UC patients, respectively. A total of 116 (67.4%) were male, whereas 56 (32.6%) were female patients. The mean age at diagnosis was 13.9 (IQR, 12.1–15.1) years.
Development of EIMs in the patients
EIMs developed in 42 patients among the total 172 patients (24.4%). EIMs developed in 34 patients among 137 diagnosed with CD (24.8%), and in 8 patients among 35 diagnosed with UC (22.9%) (P = 0.984). All patients with EIMs had developed only one EIM, and there were no patients that developed more than one EIM. The median follow-up duration was 3.2 (IQR, 1.9–5.4) years for patients with CD and 3.0 (1.0–4.0) years for patients with UC (P = 0.073). Arthritis or arthralgia was most commonly observed (n = 15, 35.7%), followed by stomatitis or oral ulcer (n = 10, 23.8%), hepatitis (n = 5, 11.9%), nephritis (n = 4, 9.5%), pancreatitis (n = 2, 4.8%), erythema nodosum (n = 2, 4.8%), pyoderma gangrenosum (n = 1, 2.4%), primary sclerosing cholangitis (n = 1, 2.4%), uveitis (n = 1, 2.4%), and ankylosing spondylitis (n = 1, 2.4%) (Table 1).
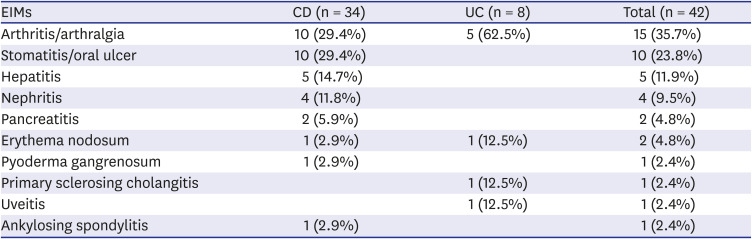
Table 1
Extraintestinal manifestations according to disease
![]()
Arthritis, which was defined as pain and tenderness, swelling, redness and heat on physical examination with radiologic signs of inflammation in one or more joints, were noted in 5 (12.5%) patients at diagnosis and during follow-up. Among hepatitis, one patient was confirmed as autoimmune hepatitis and the others as non-specific hepatitis with hypertransaminasemia. The autoimmune hepatitis had developed in a patient with CD during treatment with mesalazine, which resolved after treatment with azathioprine. Among the EIMs with kidney involvement, two were confirmed as immunoglobulin A nephropathy with kidney biopsy, and both developed in patients with CD during treatment with infliximab. Pancreatitis was observed at diagnosis in two patients with CD, which resolved after treatment with exclusive enteral nutrition.
Comparisons between the EIM-positive and -negative groups
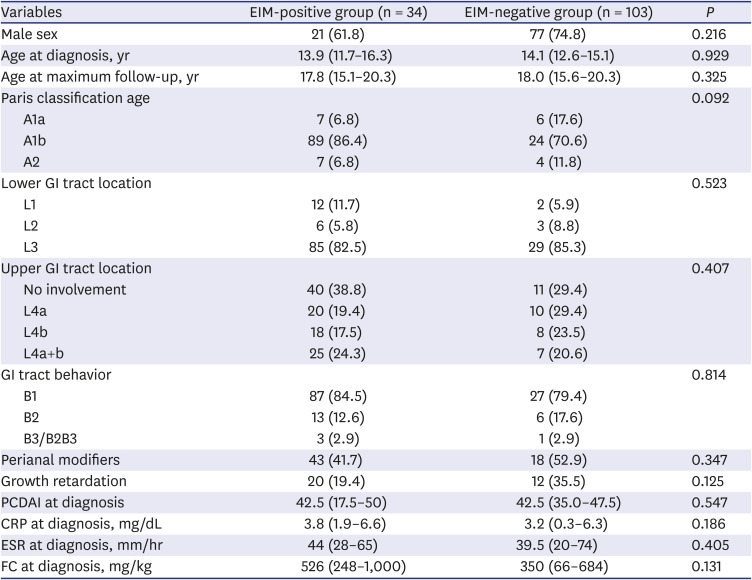
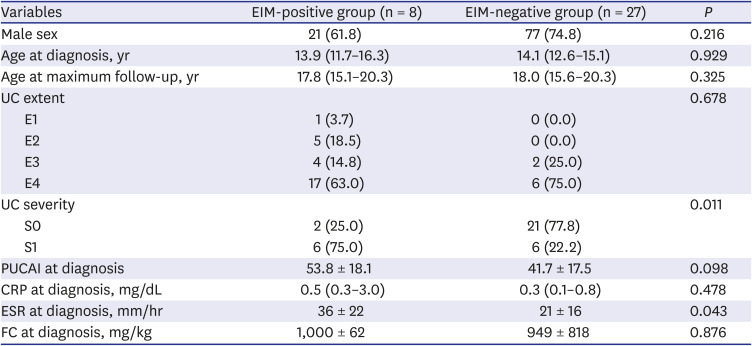
Comparisons of the variables between the EIM-positive and -negative groups in patients with CD were not statistically significant (Table 2). However, comparisons of the variables between the EIM-positive and -negative groups in patients with UC revealed a significant difference in disease severity based on the Paris classification and ESR levels at diagnosis. Patients with S1 disease severity based on the Paris classification were more likely to develop EIMs than those with S0 disease severity (P = 0.011), and higher ESR at diagnosis was significantly associated with the development of EIMs (P = 0.043) (Table 3). Meanwhile, PUCAI score at diagnosis was not significantly different between the EIM-positive and -negative groups in the patients with UC (Fig. 1A), despite the differences in PUCAI score between patients with S0 and S1 disease activity (Fig. 1B).
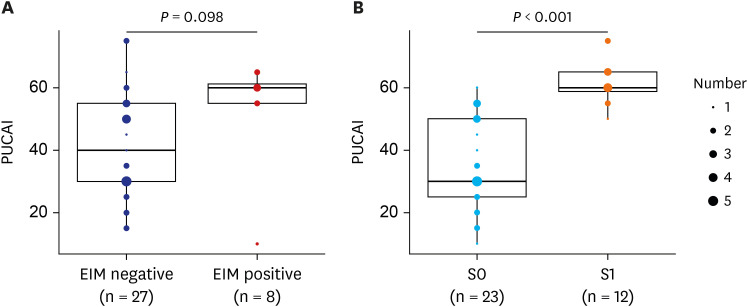 | Fig. 1PUCAI scores in patients with UC. (A) Comparison between EIM-negative and -positive group. (B) Comparison between patients with S0 and S1 disease activity based on the Paris classification.PUCAI = Pediatric Ulcerative Colitis Activity Index, UC = ulcerative colitis, EIM = extraintestinal manifestation, S0 = never severe (PUCAI < 65), S1 = ever severe (PUCAI ≥ 65).
|
Table 2
Comparison between the EIM-positive and -negative groups in CD patients
Data are expressed as median (interquartile range) for continuous variables that did not show normal distribution, unless otherwise indicated.
EIM = extraintestinal manifestation, CD = Crohn's disease, GI = gastrointestinal, A1a = 0–9 years, A1b = 10–16 years, A2 = ≤ 17 years, L1 = distal 1/3 ileum ± limited cecal disease, L2 = colonic disease, L3 = ileocolonic disease, L4a = upper disease proximal to ligament of Treitz, L4b = upper disease distal to the ligament of Treitz and proximal to the distal 1/3 ileum, L4ab = upper disease involvement in both L4a and L4b, B1 = nonstricturing nonpenetrating behavior, B2 = stricturing behavior, B3 = penetrating behavior, B2B3 = both B2 and B3, PCDAI = Pediatric Crohn's Disease Activity Index, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, FC = fecal calprotectin.
![]()
Table 3
Comparison between the EIM-positive and -negative groups in UC patients
Data are expressed as means ± standard deviation for continuous variables that showed normal distribution, and median (interquartile range) for continuous variables that did not show normal distribution, unless otherwise indicated.
EIM = extraintestinal manifestation, UC = ulcerative colitis, E1 = ulcerative proctitis, E2 = left-sided UC (distal to splenic flexure), E3 = extensive (hepatic flexure distally), E4 = pancolitis (proximal to hepatic flexure), S0 = never severe (PUCAI < 65), S1 = ever severe (PUCAI ≥ 65), PUCAI = Pediatric Ulcerative Colitis Activity Index, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, FC = fecal calprotectin.
![]()
Factors associated with EIM development in patients with UC
According to univariate logistic regression analysis, S1 disease severity based on the Paris classification was significantly associated with EIM development (Table 4). S1 disease severity and ESR at diagnosis (P < 0.1) were included in the multivariate logistic regression analysis, which revealed that S1 disease severity based on the Paris classification was the only factor that was significantly associated with EIM development (OR, 16.57; 95% CI, 2.18–287.39; P = 0.017) (Table 4).
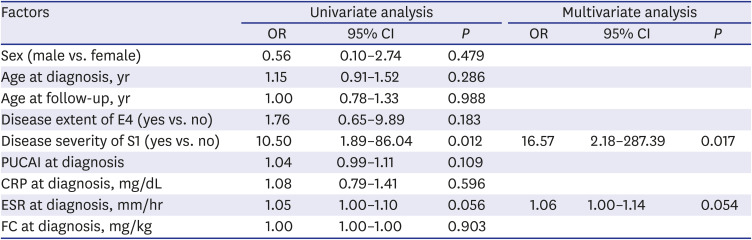
Table 4
Logistic regression analyses of factors associated with EIM development in patients with UC
EIM = extraintestinal manifestation, UC = ulcerative colitis, E4 = pancolitis (proximal to hepatic flexure), S1 = ever severe (PUCAI ≥ 65), PUCAI = Pediatric Ulcerative Colitis Activity Index, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, FC = fecal calprotectin, OR = odds ratio, CI = confidence interval.
![]()
Go to :
DISCUSSION
This is the first multicenter study to investigate the EIMs associated with pediatric IBD in Korea. We have revealed a novel finding that the disease severity of UC based on the Paris classification was significantly associated with EIM development. Close disease activity monitoring and treatment adjustment may minimize the occurrence of EIMs in Korean children and adolescents with UC. Moreover, the finding that PUCAI scores at diagnosis were not significantly different between the EIM-positive and -negative groups in the patients with UC indicates the importance of close monitoring of EIMs in addition to the assessment of PUCAI scores, which are used in everyday clinical practice.
Several studies show that the disease severity at diagnosis is related to EIM development in pediatric patients with IBD.1617 In the study of Dotson et al,16 increased disease severity was associated with the occurrence of EIMs. Their study used the Physician Global Assessment, PCDAI, modified PCDAI, PUCAI, and ESR to assess disease severity; they found that the related EIMs were arthralgia (P = 0.024), aphthous stomatitis (P = 0.001), and erythema nodosum (P = 0.009). These authors also found that aphthous stomatitis, erythema nodosum, and sclerosing cholangitis showed significantly different rates between CD and UC. Similarly, in our study the occurrence of EIMs was related with only the disease severity of UC based on the Paris classification (P = 0.012), and EIMs were significantly more frequent in CD than in UC. However, we were unable to identify significant differences between EIM types due to the small number of EIM occurrences and could not find any association between PCDAI or PUCAI scores at diagnosis with EIM development.
Intestinal inflammation in IBD is not stable but can change dynamically according to environmental factors, such as diet or medication, and consequently can change the host's immunological balance. Additionally, PCDAI or PUCAI scores represent the patient's disease activity at a single time point. Similarly, the Paris classification for CD patients is assessed at diagnosis. Thus, these factors represent cross-sectional disease activity rather than longitudinal disease activity. Meanwhile, the disease severity checked in the Paris classification for UC assesses continuous disease activity from diagnosis to assessment. This longitudinal characteristic of the disease severity checked in the Paris classification may have been why only it was associated with the EIM development in this study.
Another recent study reported that disease severity at diagnosis was associated with future outcomes in children with UC. Assa et al.18 have demonstrated that the severity of UC at diagnosis, but not disease extent, was associated with the risk of colectomy, hospitalization, flares, and biological therapy. These authors found that the EIMs were related to colonic involvement in patients with CD; however, they did not find any associations between disease severity at diagnosis and EIMs in both CD and UC.
More recently, Jansson et al.19 reported that EIMs are associated with future disease severity in pediatric IBD, finding that EIMs in UC increased the risk of biological treatment and surgery, and EIMs in CD increased the relapse rate. These results support those in studies done with French and Swiss pediatric IBD patients.2021 Other studies have reported that the presence of EIMs and a higher PUCAI score at diagnosis were related with extent progression over time since the diagnosis of pediatric UC,22 suggesting that EIMs in UC are closely related to intestinal disease activity progression, which could be an index of suspicion indicating the need for more investigation of progression.
The current study has some limitations. First, the study's retrospective nature may have resulted in selection and observational bias and may have limited accurate data collection. Second, although ours was a multicenter study in one Korean province, the total number of patients was not large enough to reflect the various EIMs that can develop during the disease course. This may be why associations between EIMs and disease severity were not observed in patients with CD in this study. Moreover, it is always intriguing to define the range of EIMs because it is not always clear what an EIM is and what a medication side-effect is. We tried to define the range of EIMs as strictly as possible; however, some data could be missing because of the retrospective nature of the study. This may be the reason why all the patients in this study had only one EIM. A short follow-up period may have also influenced this finding.
Third, the follow-up period of patients in this study was rather short for observation of EIMs that occur during the natural disease course of IBD. Due to the nature of inflammatory bowel disease, which requires continuous monitoring after diagnosis, a sufficient follow-up period from diagnosis to the onset of EIM is required to ensure the validity of the study results. Fourth, we did not investigate the timing of EIM occurrence or the association between EIM and the current medication at the time of EIM development. Hence, we were unable to investigate factors associated with the time-to-EIM development. A prospective population-based study is needed to examine the precise incidence and natural course of EIMs in Korean pediatric patients with IBD. Furthermore, considering the difference of IBD phenotype between ethnicities,23 a multinational study should better reveal the potential differences of EIM occurrence and type between different descent.
In conclusion, severe disease activity based on the Paris classification in pediatric patients with UC was significantly associated with the EIM development. As disease severity in the Paris classification is a dynamic parameter, close disease activity monitoring and treatment adjustment may minimize the occurrence of EIMs in Korean children and adolescents with UC.
Go to :
 XML Download
XML Download