

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common arrhythmia and is associated with increased risk of thromboembolism and heart failure.12 Since the findings that pulmonary veins (PVs) are the trigger foci for AF, catheter ablation has been recommended for drug refractory symptomatic AF.3 Catheter ablation in patients with heart failure showed significantly better outcome, and almost 70% of these patients showed persistent AF.4 However, the efficacy of catheter ablation for persistent AF remains suboptimal due to electrical atrial remodeling, and more than 40% of patients experienced AF recurrence.56
Surgical approaches such as Cox–Maze operation are options for this issue. However, surgical ablation is invasive and showed better outcome when performed concomitant to other cardiac surgery.789 Thoracoscopic ablation is an alternative, less invasive approach for stand-alone surgery for AF. Current guidelines recommend that thoracoscopic hybrid surgical ablation procedures should be considered in patients with failed percutaneous AF ablation.10
Hybrid AF ablation can enhance the benefits of both surgical ablation and catheter ablation. Surgical ablation targets both PVs, the left atrial (LA) posterior wall, and left atrial appendage (LAA) closure with the ability to visualize the atrium. It also can access the epicardial structures such as ganglionic plexi and ligament of Marshall.11 Catheter ablation allows more detailed electrical mapping and can target gap ablation and ablate sites out of the surgeon's view such as the cavotricuspid isthmus (CTI) or the septal region. The proper hybrid treatment should consist of a planned combination of surgical and catheter ablation. Theoretically combining the epicardial approach with endocardial ablation that includes validation of the ablation lines and modification of the residual AF substrate may increase long-term procedural success rates. A hybrid procedure consisting of the sequential combination of thoracoscopic surgical ablation and endocardial catheter ablation is an attractive alternative that complements the respective limitations of epi- and endocardial approaches. However, these two-stage approaches require longer hospitalization with increased medical costs. The timing and sequence of the hybrid procedure remains a matter of debate. Performing the whole procedure during single session lessens the risk of repeated hospitalization and anesthesia, but prolonged the duration of procedure time. Intervening the procedures more than 2–3 months interval between two stages allows the epicardial lesions to heal and stabilize, which could uncover conduction gaps and warrants the overall efficacy.
In this study, we evaluated the efficacy of the early staged hybrid procedure in hospital stay after totally thoracoscopic ablation.
METHODS
Study population
This study was a single-center, retrospective, observational study. Consecutive patients who underwent totally thoracoscopic ablation procedure from February 2012 to December 2018 were included. Patients with failed PV isolation and who received Cox–Maze surgery or LAA exclusion only were excluded. Patients who were treated with catheter ablation before totally thoracoscopic ablation were excluded. The early staged hybrid approach with an electrophysiology study after surgical thoracoscopic ablation in hospital stay was performed. In stand-alone surgical ablation group, routine electrophysiology study was not performed after totally thoracoscopic ablation and the patients were followed up after discharge. We compared the outcomes of the early staged hybrid group versus the stand-alone surgical ablation group.
Surgical techniques
Totally thoracoscopic ablation procedures were performed under general anesthesia. All procedures were performed using standard techniques as described previously.1213 The bilateral thoracoscopic approach with video-assisted thoracoscopic surgical technique was used. This technique requires only three holes for one 10 mm port and two 5 mm ports. Starting on the right side, a 5mm port was introduced in the fourth intercostal space at the mid-axillary line. After carbon dioxide insufflation to expand the operative field and depress the diaphragm, the remaining two ports were placed in the third intercostal space at the anterior axillary line and the sixth intercostal space at the mid-axillary line, respectively. After pericardial tenting, a lighted dissector (AtriCure Lumitip Dissector, Atricure, Inc., Cincinnati, OH, USA) was used to pass a rubber band under the PV antrum through the oblique sinus. An AtriCure Isolator Transpolar Clamp (Atricure, Inc.) was connected to the rubber band and positioned around the PV antrum. PV antrum isolation was performed by applying bipolar radiofrequency energy 6 times to the clamps around the PV antrum. Additional superior and inferior ablation lines connecting both PV isolation lines were created epicardially using a linear pen device (MLP, Atricure, Inc.). Ganglionated plexi subsequently were ablated with bipolar radiofrequency energy with the aid of high-frequency stimulation. Confirmation of ablation lines was obtained by pacing testing using the AtriCure Cooltip pen (MAX5, Atricure, Inc.). The procedure was repeated on the left side. Before PV and ganglionated plexus ablation, the ligament of Marshall was dissected and ablated. When all ablations were complete and conduction block was confirmed, the LAA was removed with an endoscopic stapling device.
Hybrid approach
A staged electrophysiology study was performed after totally thoracoscopic ablation median 6 days after surgery during hospitalization. The electrophysiological study was performed under sedation, and detailed electroanatomical data were obtained from the CARTO mapping system (Biosense Webster, Diamond Bar, CA, USA). Single or double trans-septal access was performed with an SL1 sheath (St. Jude Medical, St. Paul, MN, USA). The circular mapping catheter and the ablation catheter were introduced into the left atrium. Bidirectional block was confirmed for both PVs with entrance block and exit block. We applied radiofrequency catheter ablation (RFCA) if a residual PV gap was present. Additional CTI ablation was performed after PVI. Other linear lesions were created by discretion of the physician. All patients underwent catheter ablation with an open irrigated catheter (Thermocool, Biosense Webster). RF energy up to 25–35 W was used. Patients were administered anticoagulant during procedures with intravenous heparin. The infusion was adjusted to maintain an activated coagulation time of 300–400 sec.
Outcome
The primary outcome was recurrence of atrial tachyarrhythmia after three months of blanking period. Atrial tachyarrhythmia recurrence was defined as any evidence of sustained atrial tachyarrhythmia for longer than 30 sec in Holter monitoring or clinical documentation of 12-lead electrocardiogram (ECG). The secondary outcome was repeat unplanned electrophysiology study and catheter ablation due to atrial tachyarrhythmia recurrence that was refractory to drug therapy or cardioversion.
Follow-up
All patients were followed up at two weeks, three months, six months, and every six months thereafter. In addition, 24-hour Holter monitoring was performed at three, six, and 12 months and annually thereafter. Additional monitoring was performed when patients experienced tachyarrhythmia symptoms.
Statistical analysis
Statistical analysis was performed using SPSS ver. 27.0 software (SPSS Inc., Chicago, IL, USA). Continuous variables were compared using the unpaired t-test or Wilcoxon rank-sum test, and categorical variables were compared using either the χ2 test or Fisher's exact test, as appropriate. Events rate curves were obtained by Kaplan–Meier analysis and compared using a log-rank test. A P value < 0.05 was considered significant.
RESULTS
Baseline characteristics
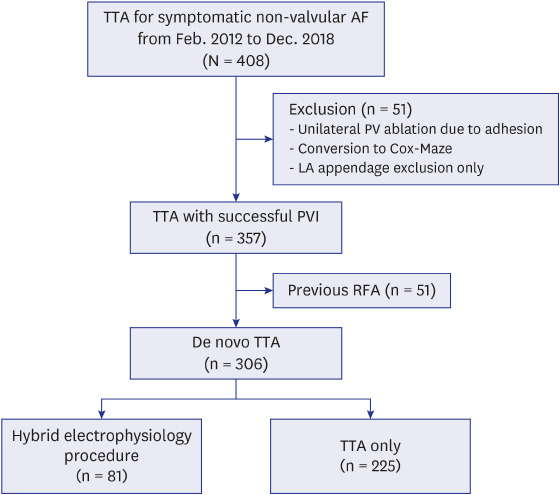
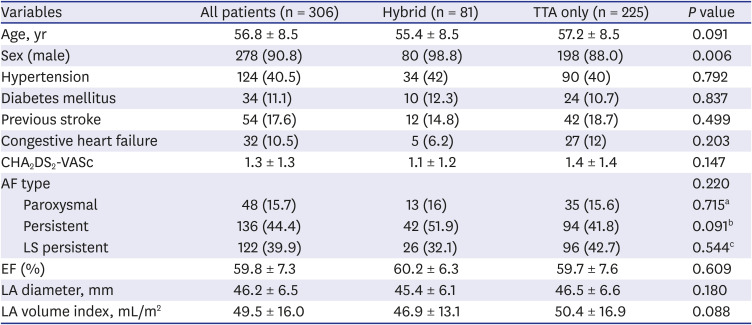
The study selection process is shown in Fig. 1. Among the initially included 408 patients who received totally thoracoscopic ablation procedure, 51 were excluded due to incomplete PVI or conversion to Cox–Maze surgery. An additional 51 patients who received RFCA before totally thoracoscopic ablation was excluded. Finally, a total of 306 patients (mean age, 56.8 ± 8.5 years; 278 [90.8%] males) was included in the study. The overall mean LA diameter was 46.2 ± 6.5 mm, and 258 (84.3%) patients showed persistent AF. Among the included patients, 81 were in the hybrid group and 225 were in the totally thoracoscopic ablation only group. The baseline characteristics are summarized in Table 1. The only significant differences between the hybrid group and the totally thoracoscopic ablation only group was sex.
Fig. 1
Flow chart.
TTA = totally thoracoscopic ablation, AF = atrial fibrillation, LA = left atrium, PVI = PV isolation, RFA = radiofrequency ablation.

Table 1
Baseline characteristics of the subjected patients
Outcomes
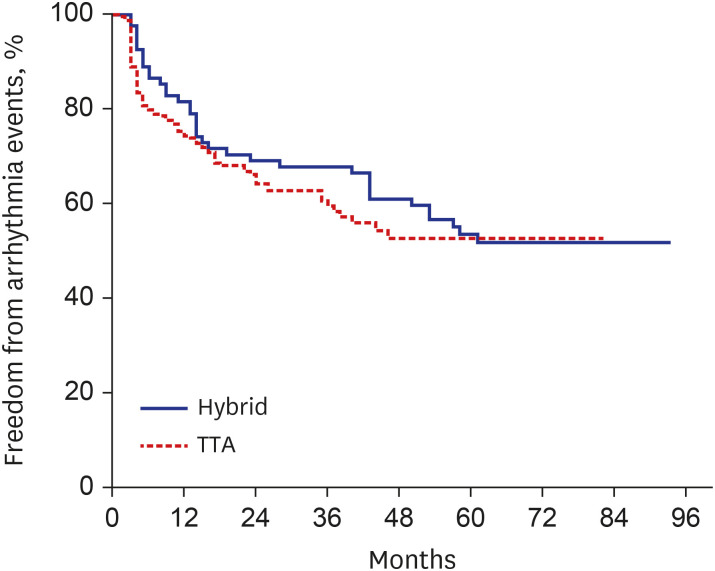
The mean follow-up duration was 30.0 months (46 months in hybrid group and 24 months in TTA only group). The one- and two-year atrial tachyarrhythmia–free survival rates were 73.9% and 63.8% in the totally thoracoscopic ablation only group and 85.2% and 67.8% in the hybrid group, respectively. The overall arrhythmia-free survival curves showed no significant differences between the two groups (log-rank P = 0.402, Fig. 2)
Fig. 2
Atrial tachyarrhythmia event-free survival in treatment groups after total thoracoscopic ablation.
TTA = totally thoracoscopic ablation.
In the hybrid group, 18 (22%) patients underwent repeat catheter ablation for recurrent atrial tachyarrhythmia who were refractory to antiarrhythmic agents or cardioversion compared to 50 (22%) in the totally thoracoscopic ablation only group. There was no significant difference in the rate of repeat procedure between the two groups (log-rank P = 0.111).
Detailed characteristics of the two groups
Electrophysiology study was performed at a median 6 days after surgery in the hybrid group. Complete PV isolation (PVI) was confirmed in 72 (88.9%) patients. The patients who showed PV gap received additional catheter ablation, and complete PVI was identified in all patients. All but 3 patients underwent CTI ablation and bidirectional block was confirmed. Other additional linear lesion sets including septal line, perimitral line, and superior vena cava isolation were created in 10 patients by physician's discretion. A total of 37 patients in the hybrid group showed recurrence of atrial arrhythmia during follow-up. Among these patients, 27 showed recurrence with AF and 10 showed atypical atrial flutter (AFL).
In the totally thoracoscopic ablation only group, 86 showed recurrence of atrial tachyarrhythmia during follow-up. Among these patients, 7 showed recurrence with definite CTI-dependent typical AFL. Fifty-eight patients had recurrence of AF, and 21 showed atypical AFL.
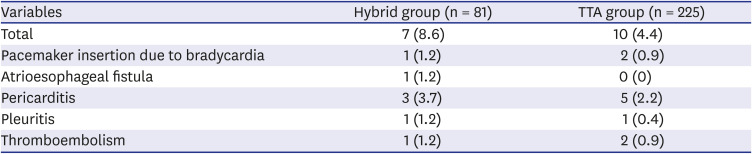
The procedure-related complications are summarized in Table 2. Atrioesophageal fistula was observed in one case in the hybrid group. Other complications including bradycardia, thromboembolism, pericarditis, and pleuritis were observed in both groups.
DISCUSSION
This is the largest study evaluating the efficacy of the hybrid approach for treatment of AF. The main finding was that more than 70% of patients maintained sinus rhythm at one year of follow-up, and there was no significant difference between the early staged hybrid group and the totally thoracoscopic ablation only group. Furthermore, the rate of repeat catheter ablation procedures showed no significant difference between the two groups.
Totally thoracoscopic ablation have advantages of hybrid cardiac surgery. This is a video-assisted minimally invasive surgery and does not require median sternotomy or a cardiac pump.14 One weakness of surgical ablation of AF is that it is difficult to ablate inaccessible cardiac structures not in face with the epicardial side, such as the CTI or interatrial septal region. Therefore, hybrid AF ablation has an advantage for improved ablation of these inaccessible structures and confirmation of electrical block using a detailed mapping technique. Furthermore, confident transmural lesions can be achieved through additional touch up ablation. In our cohort, almost 90% of patients showed complete PVI immediately after totally thoracoscopic surgical ablation. In addition, 7 of the 225 patients showed recurrence with definite CTI-dependent flutter. In this sense, the routine second stage of the approach just after surgery is not cost effective and force the patients to a longer hospital stay.
When AF progresses, atrial fibrosis and atriopathy can develop. In these cases, it is effective to identify scar and border areas through additional voltage mapping, and this often requires additional endocardial ablation.1516 Notably, detailed mapping and additional ablation are not possible through totally thoracoscopic ablation alone. However, it was not effective to perform the hybrid procedure in all patients and we confirmed that the routine electrophysiology study during the hospital stay did not show additional benefit. In this study, the frequencies of unplanned additional electrophysiology study and catheter ablation showed no significant differences between the two groups. Also, routine hybrid procedures in hospitalization after totally thoracoscopic ablation to perform prophylactic CTI ablation and confirm complete PVI did not show additional benefits. Additional electrophysiology study and catheter ablation is required only in patients with recurrence of atrial tachyarrhythmia during follow-up after totally thoracoscopic ablation. This demonstrates that deferring second-stage electrophysiology study after arrhythmia recurrence is sufficient and cost-effective.
This is a single-center, retrospective cohort study. Physician performance depends on experience and skills, and these technical approaches should be performed at experienced centers. In addition, the routine hybrid approach was the initial strategy of our hospital. Therefore, there might be differences in surgical outcomes between the two groups related to a learning curve. There also was a difference in follow-up duration. All patients were followed up with 24-hour Holter monitor or ECG instead of implantable loop recorder or longer duration Holter monitoring. However, both groups were followed up with same strategy. Therefore, this might be not affected to the difference between two groups. Finally, patients with unilateral PV isolation during surgical ablation were purposely excluded from the study. It could be creating a bias in favor of surgical ablation. The further larger-scale prospective studies would be needed.
The early staged hybrid procedure after totally thoracoscopic ablation could not improve the outcome of recurrence of atrial tachyarrhythmia. The second stage of electrophysiology study could be deferred to patients with recurrence of atrial tachyarrhythmia during follow-up after totally thoracoscopic ablation.
 XML Download
XML Download