

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lung cancer is one of the most common causes of cancer death. Several clinical trials of lung cancer screening using low-dose computed tomography (CT) have demonstrated a significant reduction in lung cancer mortality.12 The presentation of the Dutch/Belgian Nederland-Leuvens Longkanker screenings Onderzoek (NELSON) trial at the World Conference on Lung Cancer in 2018 reported decreased mortality in women (39–61%).3 Furthermore, lung cancer screening using low-dose CT has additional benefits of early detection of other diseases.45
The increasing frequency of lung cancer screening has led to increased detection of ground-glass nodules (GGNs).678 GGNs are lung nodules with a hazy increased attenuation indicative of preserved underlying bronchiolar or vascular structure, and their volume-doubling time is reportedly 769–1,005 days.9 Although there is a concern of overdiagnosis,10 stable or slowly growing GGNs are often associated with adenocarcinoma.1112 According to the Early Lung Cancer Action Project study, subsolid nodules have a higher incidence of malignancy than do solid nodules, and part-solid nodules have the highest incidence of malignancy (63%).1
Although several studies have provided new data concerning the natural course of subsolid pulmonary nodules (i.e., GGNs), there is no definitive protocol for the treatment of accompanying GGNs encountered during curative resection for NSCLC. The current Fleischner Society guidelines are not indicated for patients with a history of malignancy,13 presumably due to the lack of data concerning the natural course of accompanying GGNs. There is evidence that a history of lung cancer is a major risk factor for GGN growth.1914 Thus, to determine a follow-up strategy, there is a need to examine the natural course of accompanying GGNs that remain after curative resection for lung cancer.
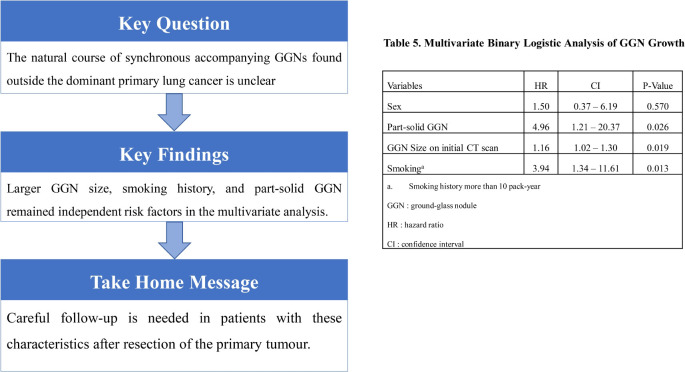
The primary purpose of this study was to review the natural course of synchronous accompanying GGNs found outside the dominant primary lung cancer, and the secondary purpose was to determine which clinical and radiological factors constitute risk factors for the growth of such GGNs.
METHODS
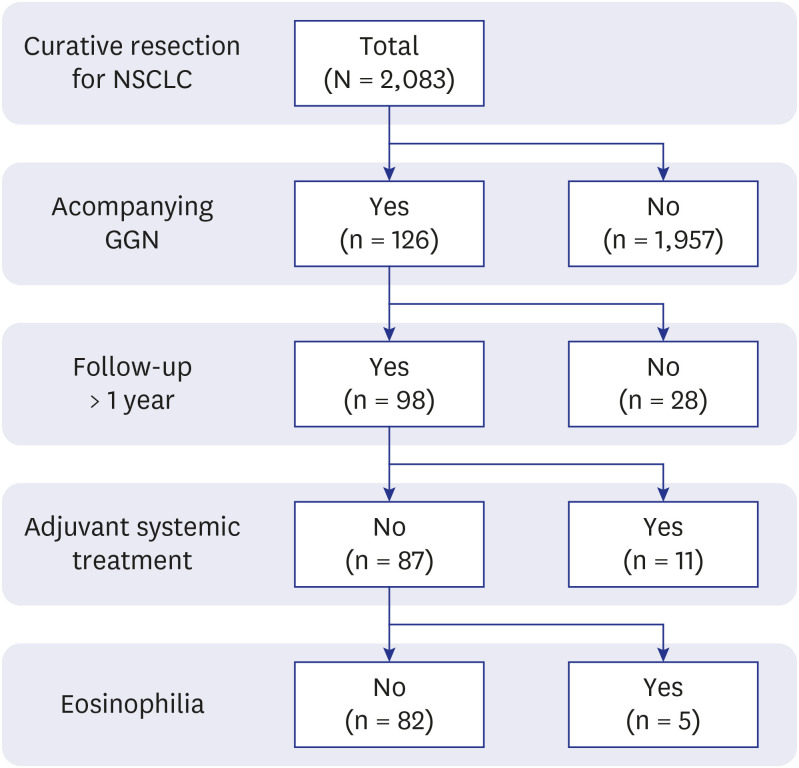
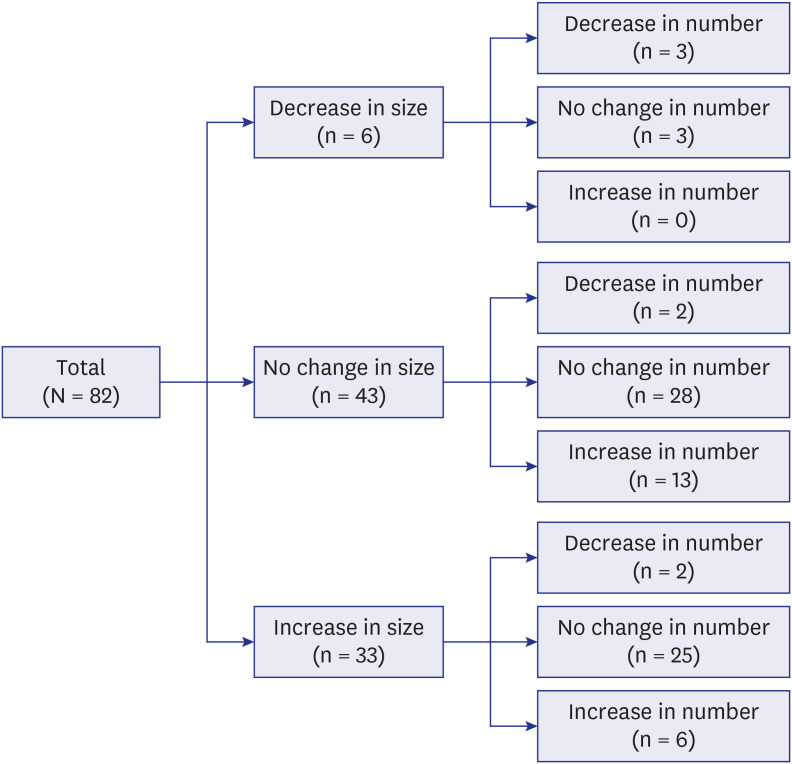
In total, 2,083 patients underwent curative resection for lung cancer between July 2009 and February 2018. Among these, the data of 126 patients who had synchronous accompanying GGNs were collected prospectively. In this study, we reviewed the retrospective data of 82 patients who had been followed up for more than 1 year (Fig. 1). We obtained informed consent from each patient for the storage of medical data, together with consent for surgery.
Fig. 1
Flow diagram of patient enrolment.
NSCLC = non-small-cell lung cancer, GGN = ground-glass nodule.
Contrast-enhanced CT, [F-18] fluorodeoxyglucose positron emission tomography-CT, contrast-enhanced magnetic resonance imaging of the brain, bone scans, and pulmonary function testing (including assessment of diffusion capacity) were performed on all patients during preoperative evaluations. In addition, endobronchial ultrasound-transbronchial needle aspiration was performed when nodal metastasis was suspected. Patients who had pulmonary metastasis were excluded from this study.
The general principles of surgical resection were to resect all suspected malignant lesions, and the extent of resection was often discussed with a multidisciplinary team. Generally, the extent of surgical resection was determined on the basis of tumour stage, estimated postoperative pulmonary function, preoperative comorbidities, and tumour location. In addition, the distribution of lesions was an important consideration during the resection of multiple primary lesions. Lobar resections were primarily preferred, but sublobar resections were conducted in selected instances (e.g., a patient diagnosed with clinical stage cT1a by 7th-edition staging, or a patient with poor lung function or general condition). If a patient had sufficient pulmonary function and seemed capable of tolerating bilateral resection, two-stage simultaneous bilateral surgical resection was performed. Thus, only small GGNs with unknown significance remained for subsequent follow-up.
In the first 2 years after surgery, patients visited the outpatient clinic at 3-month intervals for a history, plain chest radiography, and a physical examination. Chest CT scans were performed at 6-month intervals for up to 5 years after surgery. Then, follow-up CT scans were continued annually. Each CT scan included a high-resolution CT scan or a thin-section CT scan.
For person-based analyses, tumour size was determined based on the largest GGN. The size of a GGN was measured as the longest length in any section on a three-dimensional reconstructed CT scan. Definitions of GGN growth were a ≥ 2-mm increase in total size, ≥ 1-mm increase in solid component size, or the development of a new solid component.914 Although changes in GGN numbers were closely followed, this study considered nodule size to be a more significant outcome. The clinical and pathological stages were reclassified in accordance with the 8th edition of the TNM classification for lung cancer.15 Histopathological diagnoses were reclassified in accordance with the 2015 World Health Organization classification of lung tumours.16
Categorical variables are expressed as numbers and percentages, and were compared using the χ2 test or Fisher's exact test. Continuous values that exhibited normal distributions are expressed as means and standard deviations. Continuous values that did not exhibit normal distributions are expressed as medians and interquartile ranges. Student's t-test and the Mann-Whitney U test were used to evaluate differences between continuous variables, depending on the results of the Shapiro-Wilk normality test. Logistic regression was used for multivariate analyses. Two-sided P values < 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics, version 22.0 (IBM Corp. Armonk, NY, USA).
RESULTS
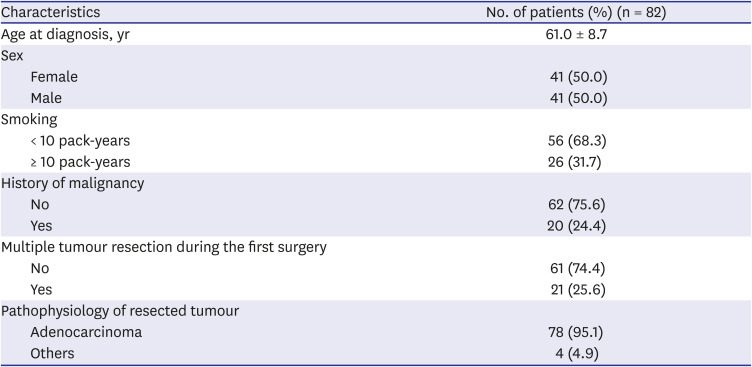
The clinical characteristics of the included patients are shown in Table 1. There were 41 women and 41 men, and their mean age was 61.0 ± 8.7 years. Fifty-one patients (62.2%) were never-smokers, and 20 patients (24.4%) had one or more histories of other malignancies. Multiple lesions were resected during the first operation in 21 of 82 patients (25.6%), and all lesions were classified as adenocarcinoma. Most of the patients with multiple tumours had one or more lepidic-type adenocarcinomas or atypical adenomatous hyperplasia (19 of 21; 90.5%).
Table 1
Baseline characteristics and operative outcomes of the patients
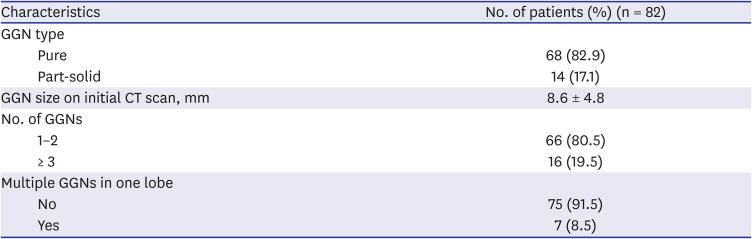
The characteristics of the accompanying GGNs (each patient's largest GGN) are shown in Table 2. Fourteen patients (17.1%) had GGNs with a solid component, 16 had three or more remnant GGNs, and the GGN size was < 10 mm in 55 patients. In addition, the distribution of the remaining multiple GGNs (three or more) was limited to a single lobe in 7 patients.
Table 2
GGN characteristics
The median duration of follow-up was 36.0 months (interquartile range, 23.0–59.3 months). No patient died during follow-up, but Tumour recurrence was observed in five patients. The natural courses of the accompanying GGNs are shown in Fig. 2. During the follow-up period, a decrease in GGN size was observed in only 6 patients (7.3%, group A) and no change in GGN size was detected in approximately half of the patients (43 of 82, 52.4%, group B). GGNs increased in size in 33 patients (40.2%, group C), and there was no statistical difference of follow-up period between the groups B and C (P = 0.259).
Among these 33 patients with increased GGN, three underwent a second surgery for GGNs that increased in size, and all three were diagnosed with adenocarcinoma; however, the type of adenocarcinoma differed from the tumour resected during the first surgery (second primary adenocarcinoma) (Table 3). Five patients could not undergo a second surgery due to tumour recurrence. Six patients are now under consideration for a second surgery (including two patients who refuse second surgery), and the remaining 19 patients are continuing follow-up because their GGNs remain < 2 cm.
Table 3
Pathological outcomes of the second surgery

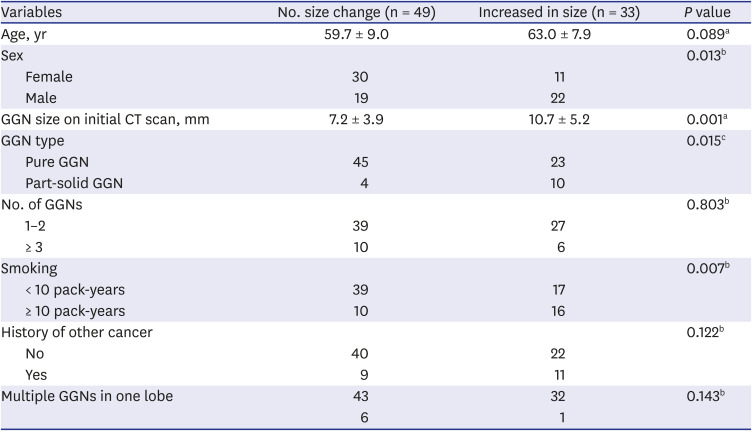
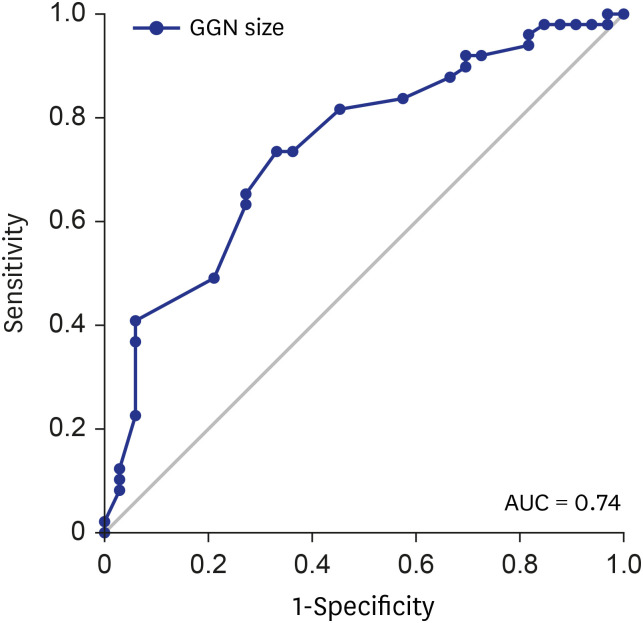
Univariate analysis indicated that male sex, larger GGN size, part-solid GGN and smoking history were significant risk factors (Table 4). Of these, larger GGN size, part-solid GGN and smoking history remained independent prognostic factors in the multivariate analysis (Table 5). We performed a receiver operating characteristic curve analysis to determine the cut-off value of the GGN size and to predict the growth of GGNs. A cut-off value of ≥ 8 mm was optimal, with an area under the receiver operating characteristic curve of 0.74. The respective sensitivity and specificity were 72.7% and 65.3% with a cut-off value of 8 mm and 93.9% and 40.8% with a cut-off value of 6 mm (Fig. 3).
Table 4
Univariate analysis of GGN growth

DISCUSSION
It is highly expected that lung cancer screening using low-dose CT will be a new standard healthcare strategy because of the positive results in clinical trials. This is because detection of multiple primary lung cancers or the dominant tumour with accompanying GGNs will increase. Given a previous genetic study concerning lepidic-type adenocarcinoma, accompanying GGNs are highly expected to be multifocal, independent tumours.17
However, it is not technically feasible to resect all accompanying GGNs simultaneously, particularly when multiple small GGNs are scattered in bilateral lungs or when a GGN is centrally located on the contralateral side. Because resecting the dominant tumour with multiple accompanying GGNs has comparable survival outcomes, surgical resection maintains its role in primary treatment.1819 The reported mean volume-doubling time of GGNs is 769–1,005 days620; thus, follow-up without resection of accompanying GGNs is a reasonable approach. Lee et al.21 reported that 9% of part-solid GGNs were upstaged from T1a to T1b (classified by the 7th American Joint Committee on Cancer staging system) during the follow-up period, but no significant decreases in disease-free or overall survival were observed.
Several studies have attempted to identify clinical factors or radiological findings related to the prognosis of synchronous or metachronous GGNs.9222324 However, the results of those studies were inconsistent, potentially because of differences in study design, the characteristics of the study population, management strategy, or the definitions of variables and outcomes. Our study was a person-based study9 confined to accompanying GGNs,23 and focused on GGN size changes. In clinical practice, it is important to identify patients at greater risk of second surgery. Therefore, we presumed that GGN growth is clinically more significant (for determining second-surgery status) than an increase in GGN number (i.e., newly emerged small metachronous GGNs).
In our study, larger GGN size was a risk factor for GGN growth, as in previous studies.923 The cut-off value of our study (8 mm) was similar to the findings of previous studies. Also, the presence of a part-solid GGN yielded results consistent with those reported in previous studies.924 Smoking was an independent risk factor for GGN growth in our study. Most of our patients were diagnosed with adenocarcinoma in primary tumours (95.1%). Adenocarcinoma with a GGN pattern generally exhibits a weak association with smoking. However, several studies have reported paradoxical effects of smoking on GGN growth, which is consistent with our results.25
Some limitations of our study should be discussed. First, this person-based retrospective study focused on the largest GGN and the change in its size, which created difficulty when comparing outcomes directly with other studies. Second, the small sample size and heterogeneity of the patient population might have affected the study outcomes. Third, the follow-up duration was short, which may have influenced patient outcomes. Fourth, because of the short follow-up duration, small numbers of patients underwent a second surgery, resulting in a smaller number of pathologically confirmed GGNs that increased in size.
In conclusion, among patients who underwent curative resection for lung cancer, 6.0% had accompanying GGNs that could not be resected simultaneously. Growth of the accompanying GGNs was observed in 40.2% of patients, and the pathological results for the three resected GGNs differed from those of the primary tumours in those patients. The GGN size, part-solid GGN and smoking history were independent risk factors that influenced GGN growth. Careful follow-up is needed in patients with these characteristics after resection of the primary tumour.
 XML Download
XML Download