

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD) is a leading cause of morbidity and mortality worldwide.1) For early diagnosis and individualized therapy, it is of paramount importance to understand the mechanism of CAD development as well as the factors determining the prognosis of CAD patients. Over the past century, many risk factors associated with CAD development have been identified and utilized for prevention and treatment.2) However, the incidence of CAD is still high and the prognosis is poor.1) Given that substantial portion of individuals without traditional cardiovascular risk factors suffering from cardiovascular events,3) more accurate risk predictions are needed. As the causes of initiation and progression of coronary atherosclerosis are multifactorial, there is still a room for improvement in the prognosis of CAD patients by identifying new modifiable risk factors.
Many epidemiologic studies have shown a close association between the level of blood pressure (BP) and cardiovascular events and mortality.4) BP reduction is very effective way to reduced cardiovascular risk.5)6) Specific levels of systolic and diastolic BPs have been used in the diagnosis and treatment of hypertension and to define cardiovascular risk.7)8) However, BP is a periodic phenomenon that can be divided into 2 components: steady (mean arterial pressure) and pulsatile (pulse pressure [PP]). The steady component is determined by cardiac output and small resistance arterial function. The pulsatile component is mainly determined by left ventricular (LV) ejection, large artery compliance (the opposite of stiffness) and the speed and the intensity of the reflected waves returning toward the heart from arterial bifurcation points (due to impedance changes).9) The large conduit arteries buffer the pulsating blood ejection generated by LV contraction by intermittent expansion according to the cardiac cycle. In the LV diastolic phase, when there is no blood ejection from the heart, the arteries maintain perfusion pressure to major organs and periphery by wall contraction through vascular recoil.10) Many studies have shown that measurements of these pulsatile components of BP such as PP, augmentation index (AIx) and pulse wave velocity (PWV) are associated with the development of future cardiovascular events independent of BP and other risk factors.11)12)13)14)15)16)17)18)19)20) Therefore, it is important to understand that BP is composed of pulsatile component as well as steady component, which may offer better insight into pathophysiology of the development of target organ damage and cardiovascular risk. Moreover, this in-depth understanding might help to evaluate and monitor patients' response to treatment, as well as to develop effective treatment strategies.
Here, we will review the role of arterial pulsatile hemodynamics in CAD, focused on the association between pulsatile hemodynamics and CAD, and prognostic value as well as clinical implications of pulsatile hemodynamics in CAD patients.
Go to : 
MEASUREMENT OF ARTERIAL PULSATILE HEMODYNAMICS
There are several non-invasive measures that allow assessment of arterial pulsatile hemodynamics.
Pulse pressure
PP is the result of a combination of the episodic nature of LV contraction and the elastic properties of the large arteries.21) Brachial PP (brPP) is the simplest and most widely used indicator of atrial pulsatile hemodynamics. brPP is defined as the pressure difference between systolic and diastolic BP of at the site of brachial artery. Many studies have shown that brPP is associated with target organ damage and cardiovascular outcome.11)12)13)14)15) However, it should be noted that brPP does not adequately reflect central aortic PP (aPP) or aortic stiffness because there is PP amplification between central and peripheral arteries.22) Central aPP can be obtained using non-invasive methods by analyzing the waveforms of the brachial or radial arteries.22) Since central aorta is located closer to the heart, brain, and kidney than brachial artery, aPP is more influential to these vital organs and may have a higher degree of clinical relevance than brPP.22)23)24) In addition to arterial stiffness, PP is greatly affected by factors related to cardiac function such as stroke volume, heart rate and pattern of LV ejection.21) Therefore, the effects of these factors should be considered and controlled during analysis. Moreover, PP is not a direct measure of arterial hemodynamics but just a mathematical difference between systolic and diastolic BP.
Wave reflections
Normally, when the pulse wave from the heart passes through the elastic arteries and reaches the muscular artery, a smaller reflected wave that goes backwards to the heart is generated, mainly at branch points or sites of impedance mismatch.21) In a compliant arterial system, effectively timed wave reflections (i.e. with a maximum during diastole) enhance coronary perfusion, which mainly occurs during diastole.9) In a stiffened arterial system, the velocity of reflected wave increases, thus reflected waves merge earlier with forward waves, leading to increase (augmentation) in late systolic BP and PP, and to a higher workload on the LV.25) Standard integrated measure of wave reflection is AIx, which is defined as the amount of pressure augmentation relative to PP. The most widely used method for evaluating central AIx is to first obtain a waveform by performing applanation tonometry on the radial artery, and then calculate the waveform and AIx of central aorta using a generalized transfer function (GTF).23)26) The central AIx estimated by the GTF method is very well correlated with the values measured by invasive catheterization.27)28) Many studies have shown that increased central AIx is associated with atherosclerotic burden and cardiovascular risk.16)17) However, while AIx is a sensitive marker of arterial aging in young individuals, AIx may underestimate the degree of arterial stiffness and cardiovascular risk in older people, likely associated with reduced impedance mismatch.29)30) Since several clinical factors such as age, height and heart rate affect AIx, it is important to consider the effects of these confounding variables when analyzing AIx-related data.31) Given that AIx is highly affected by heart rate, it is sometimes used after calibrating to 75 heart rate per minute (AIx@75).32)33)34) Also, LV function has a major influence of central waveforms and, thus, on AIx.35) For certain types of pulse waveforms, in particularly in young healthy individuals, AIx can be calculated as negative.36)
Pulse wave velocity
The pressure generated by the LV contraction is transmitted towards the periphery not only with the bloodstream but also in the arterial wall. Since the degree of stiffening of the arterial wall and the speed of the pulse wave traveling along the arterial wall are proportional, the pulse wave transmission speed (= PWV) is an important measure of arterial stiffness.37) PWV is defined as the distance between 2 specific arterial points divided by the time difference of the pulse wave passing through these 2 distances. The higher the PWV value, the greater the arterial stiffness. Of note, higher PWV is a risk factor for future cardiovascular events and all-cause mortality independent of traditional risk factors.18)19) Because it is non-invasive, relatively easily quantitated, and well supported by a wealth of outcome data, PWV is considered to be the most useful clinical marker of arterial stiffness.37)38) There are various PWVs depending on the measurement locations, but among them, aortic PWV (aPWV), carotid-femoral PWV (cfPWV) and brachial-ankle PWV (baPWV) are the most widely used. As cfPWV is the direct measures of arterial stiffness of central elastic arteries, it is considered as gold standard for the noninvasive measure of arterial stiffness.39) Compared to cfPWV, more recently developed baPWV is more simple to measure by just wrapping BP cuffs in both upper arms and legs, and is validated in many clinical studies.18)40)41) Thus, baPWV may be useful in mass screening, and it has been more commonly used in Asian countries in research and clinical fields.41) Main limitation of PWV is that it is highly affected by various clinical factors, mainly by age and BP.39)42) When BP rises, the tension of the vessel wall increases, and the pulse wave transmission speed increases as if arterial stiffness increases.43) When interpreting PWV, the effect of these factors should be considered. In addition, for the accuracy of the PWV value, it is necessary to measure the distance between 2 points in the blood vessel. However, it is generally difficult to accurately measure the distance between these 2 points of vessel wall, so it is estimated by measuring the distance between 2 points on the surface of the human body, or by calculating with a predetermined equation.37)41)
Invasive measurements
Direct measurement of pressure by inserting an intraarterial catheter is the most accurate method assessing arterial pulsatile hemodynamics. However, its use is hindered due to invasiveness and cost. Therefore, these measurements are primarily limited to patients undergoing invasive coronary angiography (CAG).44)45)46) Although the invasive measurement can be performed in limited clinical conditions, information on central arterial hemodynamics measured invasively can be used for validation of non-invasively measured values.46)47)48) It also provides diagnostic and prognostic value of patients with undergoing invasive CAG.44)49)50)51)52)53) Invasive hemodynamic measurement may be feasible in patients undergoing invasive CAG because it can be performed during the procedure, so there is no additional cost or risk, and the measurement time is short.
Go to :
PATHOPHYSIOLOGY
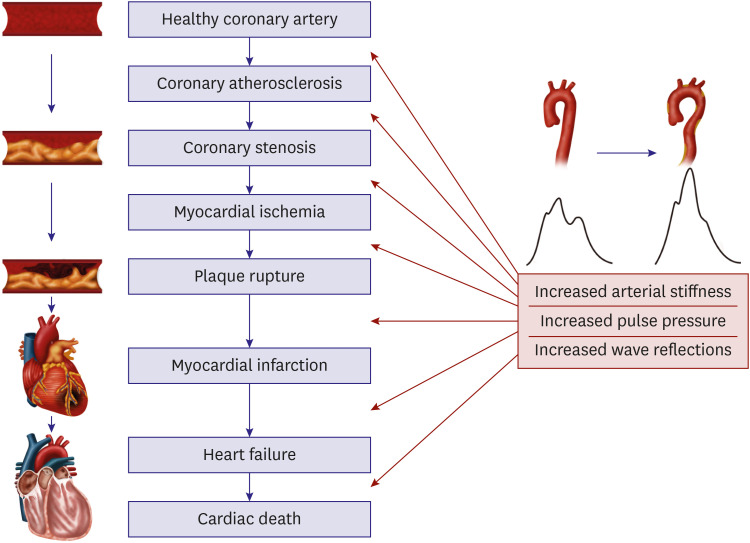
In a recent animal model in hypercholesteremic, transgenic minipigs, the role of elevated BP in facilitating the accumulation of low-density lipoprotein-cholesterol (LDL-C) and plaque formation in coronary arteries was nicely illustrated.54) A closer look unveils that the cyclic strain of the arterial wall is mainly determined by the cyclic (pulsatile) change of BP,55) playing an important role on every stage of the development of atherosclerosis.55) For instance, at an early stage, elevated PP was the driver of the activation of C-reactive protein and of the influx of lipids into the arterial intima, leading to oxidized LDL-C.56) Later on, through various mechanisms, cyclic stretch promotes plaque progression,55)57) weakening of the fibrous cap and plaque rupture.58) These findings may explain the consistent association between pulsatile hemodynamics and the presence and severity of coronary atherosclerosis outlined below. Figure 1 shows that pulsatile hemodynamics are deeply involved in development and progression of coronary atherosclerosis, plaque rupture, and subsequent myocardial infarction and, ultimately, heart failure.
When clinicians estimate the severity of CAD, the anatomical extent of a coronary stenosis is typically considered. Based on animal experiments, at diameter stenosis of 50%, maximum coronary flow (coronary flow reserve [CFR]) begins to fall, and at 85% diameter stenosis resting coronary flow begins to fall.59) Recent advances take the functional severity of a coronary stenosis into account, using fractional flow reserve or related measurements, which are based on pressure measurements proximal (in the aorta or at a coronary ostium) and distal to a coronary stenosis (as a measure of relative CFR), the latter with dedicated intracoronary wires.60) These methods are now recommended by clinical practice guidelines from major Cardiology societies61) and not the focus of this review. We rather address the impact of pulsatile hemodynamics of large arteries on coronary blood flow. A prerequisite of correct understanding of the physiology is the fact that—in contrast to other vascular beds in the body—perfusion of the myocardium (in particular the subendocardium) occurs predominantly during diastole, because during systole the contracting myocardium interrupts flow in intramyocardial arteries.62) The ratio between myocardial oxygen demand (tension time index in systole) and myocardial oxygen supply (diastolic pressure time index) can be approximated by the area under the aortic pressure waveforms in systole and diastole, respectively.63) This ratio is well balanced in young, healthy individuals. With aging, arterial stiffness increases, shifting reflected waves towards systole, thus increasing systolic and decreasing diastolic BP, and distorting the above mentioned ratio to a tendency towards ischemia.62) The interplay between coronary stenosis and aortic stiffening was nicely shown in an animal experiment: in 10 mongrel dogs, a coronary stenosis was produced in the circumflex artery with a metal constrictor, while the left anterior descending coronary (LAD) artery was left healthy. This stenosis was not sufficient to induce ischemia at rest and with pacing, as long as the aorta remained elastic. When the aorta was stiffened with banding, however, the combination of exercise (pacing), stenosis and a stiffened aorta led to ischemia in the territorium of the circumflex artery,64) but not in the LAD. In humans, coronary blood flow was measured invasively following successful percutaneous coronary intervention (PCI) in 18 patients.65) Resting, but more hyperemic coronary blood flow was strongly and inversely related to aPWV and central PP. Moreover, the gain in coronary blood flow following PCI was substantial in patients with a compliant aorta, but much less so in patients with a stiff aorta. These results were confirmed by non-invasive studies, showing inverse relationships between cfPWV,66) baPWV,67)68) and AIx68) and CFR in patients without severe coronary stenosis. As a clinical consequence, patients with established CAD and a high amount of wave reflections reach the ischemic threshold earlier, as proven in a study of 96 patients with CAD, undergoing treadmill exercise tests.69)
Furthermore, increased arterial stiffness and increased wave reflections may lead to LV hypertrophy, prolongation of mechanical systole70) (with consecutive reduction of diastolic time) and impairment of diastolic function10)71) (with increased LV diastolic pressures72)), all of them further compromising myocardial perfusion and predisposing to (subendocardial) ischemia.
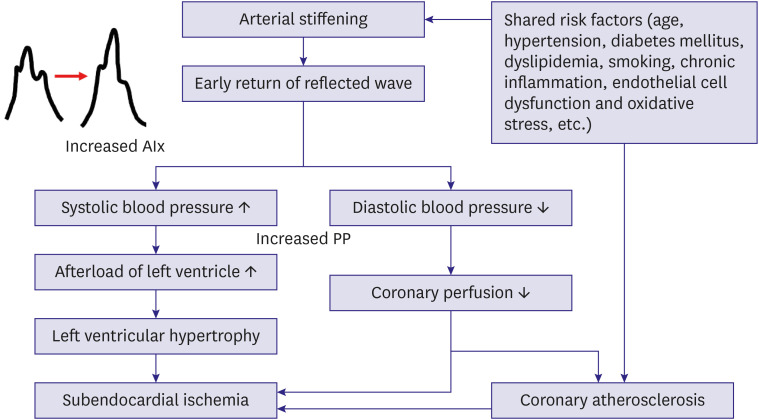
Another mechanism for the relationship between pulsatile hemodynamics/arterial stiffness and coronary atherosclerosis is that both share common risk factors, most prominent aging, but also including traditional cardiovascular risk factors, endothelial dysfunction, chronic inflammation and oxidative stress.39)41) A summary of the association of arterial stiffening and increased wave reflection with CAD is shown in Figure 2.
Go to :
ASSOCIATION OF PULSATILE HEMODYNAMICS WITH THE PRESENCE AND EXTENT OF CORONARY ATHEROSCLEROSIS
Many clinical studies have shown that measures of arterial stiffness and wave reflections are associated with CAD (Table 1).50)52)53)73)74)75)76)77)78)79)80)81)82)83)84)85)86)87)88)89)90)91)92)93)94)95) Most studies were conducted with patients undergoing invasive CAG, and CAD was assessed by the analysis of invasive CAG. In some studies, CAD was assessed using coronary computed tomography angiography (CCTA).74)79)88)89)90) Most of study subjects of these studies were with suspected or documented CAD, but one study included stroke patients.79) There were various methods of measuring arterial pulsatile hemodynamics used in these studies, which included brPP, cfPWV, baPWV, aPWV, AIx and aPP. aPWV/cfPWV and AIx, measured by tonometry, aPP measured invasively using intra-arterial catheter monitoring, and baPWV were the most widely applied measures for arterial pulsatile hemodynamics in these studies. In one study, aortic distensibility was assessed using aortic CTA.90) Most of these studies have shown consistent findings that measurements of arterial pulsatile hemodynamics were associated with the presence and severity of CAD even after controlling for potential confounders. In a longitudinal study with cardiac CTA, even the progression of aortic stiffness was associated with the progression of coronary atherosclerosis.90) However, another study showed a neutral result indicating that there was no significant difference in AIx in patients with and without CAD.82)
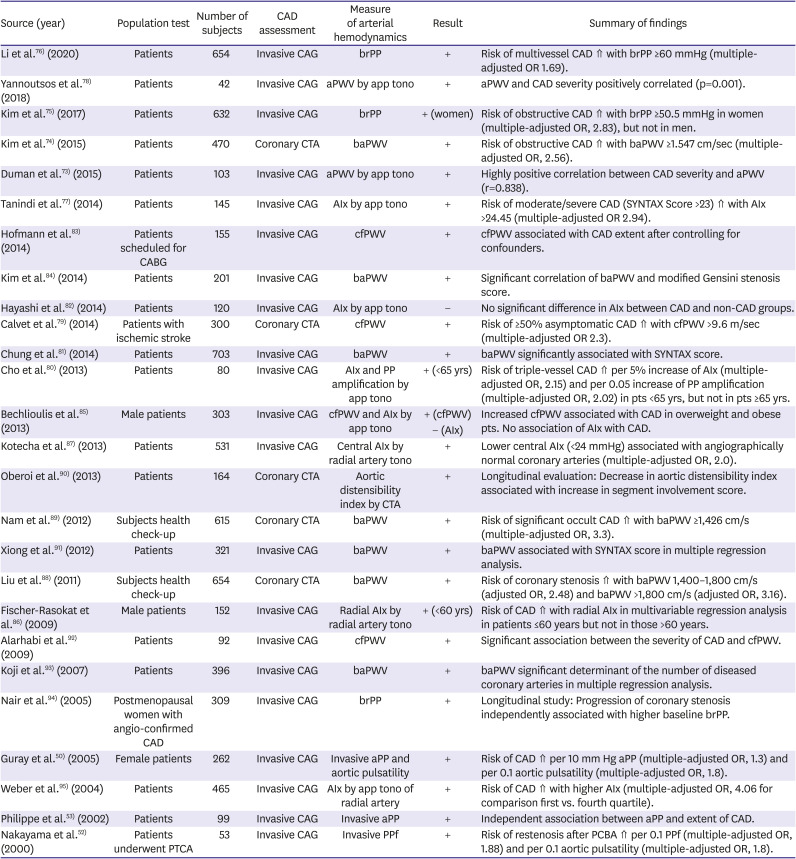
Table 1
Summary of studies showing the association of arterial pulsatile hemodynamics and CAD
| Source (year) | Population test | Number of subjects | CAD assessment | Measure of arterial hemodynamics | Result | Summary of findings |
|---|---|---|---|---|---|---|
| Li et al.76) (2020) | Patients | 654 | Invasive CAG | brPP | + | Risk of multivessel CAD ⇑ with brPP ≥60 mmHg (multiple-adjusted OR 1.69). |
| Yannoutsos et al.78) (2018) | Patients | 42 | Invasive CAG | aPWV by app tono | + | aPWV and CAD severity positively correlated (p=0.001). |
| Kim et al.75) (2017) | Patients | 632 | Invasive CAG | brPP | + (women) | Risk of obstructive CAD ⇑ with brPP ≥50.5 mmHg in women (multiple-adjusted OR, 2.83), but not in men. |
| Kim et al.74) (2015) | Patients | 470 | Coronary CTA | baPWV | + | Risk of obstructive CAD ⇑ with baPWV ≥1.547 cm/sec (multiple-adjusted OR, 2.56). |
| Duman et al.73) (2015) | Patients | 103 | Invasive CAG | aPWV by app tono | + | Highly positive correlation between CAD severity and aPWV (r=0.838). |
| Tanindi et al.77) (2014) | Patients | 145 | Invasive CAG | AIx by app tono | + | Risk of moderate/severe CAD (SYNTAX Score >23) ⇑ with AIx >24.45 (multiple-adjusted OR 2.94). |
| Hofmann et al.83) (2014) | Patients scheduled for CABG | 155 | Invasive CAG | cfPWV | + | cfPWV associated with CAD extent after controlling for confounders. |
| Kim et al.84) (2014) | Patients | 201 | Invasive CAG | baPWV | + | Significant correlation of baPWV and modified Gensini stenosis score. |
| Hayashi et al.82) (2014) | Patients | 120 | Invasive CAG | AIx by app tono | − | No significant difference in AIx between CAD and non-CAD groups. |
| Calvet et al.79) (2014) | Patients with ischemic stroke | 300 | Coronary CTA | cfPWV | + | Risk of ≥50% asymptomatic CAD ⇑ with cfPWV >9.6 m/sec (multiple-adjusted OR 2.3). |
| Chung et al.81) (2014) | Patients | 703 | Invasive CAG | baPWV | + | baPWV significantly associated with SYNTAX score. |
| Cho et al.80) (2013) | Patients | 80 | Invasive CAG | AIx and PP amplification by app tono | + (<65 yrs) | Risk of triple-vessel CAD ⇑ per 5% increase of AIx (multiple-adjusted OR, 2.15) and per 0.05 increase of PP amplification (multiple-adjusted OR, 2.02) in pts <65 yrs, but not in pts ≥65 yrs. |
| Bechlioulis et al.85) (2013) | Male patients | 303 | Invasive CAG | cfPWV and AIx by app tono | + (cfPWV) | Increased cfPWV associated with CAD in overweight and obese pts. No association of AIx with CAD. |
| − (AIx) | ||||||
| Kotecha et al.87) (2013) | Patients | 531 | Invasive CAG | Central AIx by radial artery tono | + | Lower central AIx (<24 mmHg) associated with angiographically normal coronary arteries (multiple-adjusted OR, 2.0). |
| Oberoi et al.90) (2013) | Patients | 164 | Coronary CTA | Aortic distensibility index by CTA | + | Longitudinal evaluation: Decrease in aortic distensibility index associated with increase in segment involvement score. |
| Nam et al.89) (2012) | Subjects health check-up | 615 | Coronary CTA | baPWV | + | Risk of significant occult CAD ⇑ with baPWV ≥1,426 cm/s (multiple-adjusted OR, 3.3). |
| Xiong et al.91) (2012) | Patients | 321 | Invasive CAG | baPWV | + | baPWV associated with SYNTAX score in multiple regression analysis. |
| Liu et al.88) (2011) | Subjects health check-up | 654 | Coronary CTA | baPWV | + | Risk of coronary stenosis ⇑ with baPWV 1,400–1,800 cm/s (adjusted OR, 2.48) and baPWV >1,800 cm/s (adjusted OR, 3.16). |
| Fischer-Rasokat et al.86) (2009) | Male patients | 152 | Invasive CAG | Radial AIx by radial artery tono | + (<60 yrs) | Risk of CAD ⇑ with radial AIx in multivariable regression analysis in patients ≤60 years but not in those >60 years. |
| Alarhabi et al.92) (2009) | Patients | 92 | Invasive CAG | cfPWV | + | Significant association between the severity of CAD and cfPWV. |
| Koji et al.93) (2007) | Patients | 396 | Invasive CAG | baPWV | + | baPWV significant determinant of the number of diseased coronary arteries in multiple regression analysis. |
| Nair et al.94) (2005) | Postmenopausal women with angio-confirmed CAD | 309 | Invasive CAG | brPP | + | Longitudinal study: Progression of coronary stenosis independently associated with higher baseline brPP. |
| Guray et al.50) (2005) | Female patients | 262 | Invasive CAG | Invasive aPP and aortic pulsatility | + | Risk of CAD ⇑ per 10 mm Hg aPP (multiple-adjusted OR, 1.3) and per 0.1 aortic pulsatility (multiple-adjusted OR, 1.8). |
| Weber et al.95) (2004) | Patients | 465 | Invasive CAG | AIx by app tono of radial artery | + | Risk of CAD ⇑ with higher AIx (multiple-adjusted OR, 4.06 for comparison first vs. fourth quartile). |
| Philippe et al.53) (2002) | Patients | 99 | Invasive CAG | Invasive aPP | + | Independent association between aPP and extent of CAD. |
| Nakayama et al.52) (2000) | Patients underwent PTCA | 53 | Invasive CAG | Invasive PPf | + | Risk of restenosis after PCBA ⇑ per 0.1 PPf (multiple-adjusted OR, 1.88) and per 0.1 aortic pulsatility (multiple-adjusted OR, 1.8). |
AIx = augmentation index; aPP = aortic pulse pressure; app tono = applanation tonometry; aPWV = aortic pulse wave velocity; AUC = area under curve; baPWV = brachial-ankle pulse wave velocity; brPP = brachial pulse pressure; CABG = coronary artery bypass graft; CAD = coronary artery disease; CAG = coronary angiography; cfPWV = carotid-femoral pulse wave velocity; CI = confidence interval; CTA = computed tomography angiography; OR = odds ratio; PCBA = percutaneous coronary balloon angioplasty; PPf = fractional pulse pressure; SYNTAX = Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery.
![]()
Go to :
PROGNOSTIC VALUE OF ARTERIAL PULSATILE HEMODYNAMICS IN CORONARY ARTERY DISEASE PATIENTS
The prognostic value of arterial pulsatile hemodynamics in CAD patients has been reported in several studies (Table 2).34)44)49)51)96)97)98)99)100)101)102)103)104)105)106)107)108) In these studies, non-invasive measurements for arterial pulsatile hemodynamics included AIx assessed by radial artery applanation tonometry, baPWV, cfPWV and brPP. Invasive assessment of aPP, aPWV, AP and AIx were also used as indicators of arterial pulsatile hemodynamics. During about 1–5 year of clinical follow-up, these measurements were independently associated with the occurrence of cardiovascular events or mortality in multivariable analyses. To be more specific, in recent a study of 1,040 patients undergoing invasive CAG, aPWV was invasively measured during CAG, and it was associated with cardiovascular events during the follow-up after CAG.44) cfPWV could predict 1-year cardiovascular outcome in patients with successful PCI.104) In patients after a first acute ST-elevation myocardial infarction, those with a higher aPWV measured by cardiac magnetic resonance imaging had a worse prognosis.96) Higher value of baPWV was an independent predictor of adverse cardiovascular events in patients with or suspected CAD in Asian countries.97)98)100)101)102)103)105)107) Non-invasively measured AIx using radial artery tonometry were also useful in the prediction of cardiovascular events in patients undergoing invasive CAG.34)108) All this data suggests that the measurements of arterial pulsatile hemodynamics in CAD patients is valuable in the prediction of future cardiovascular events.
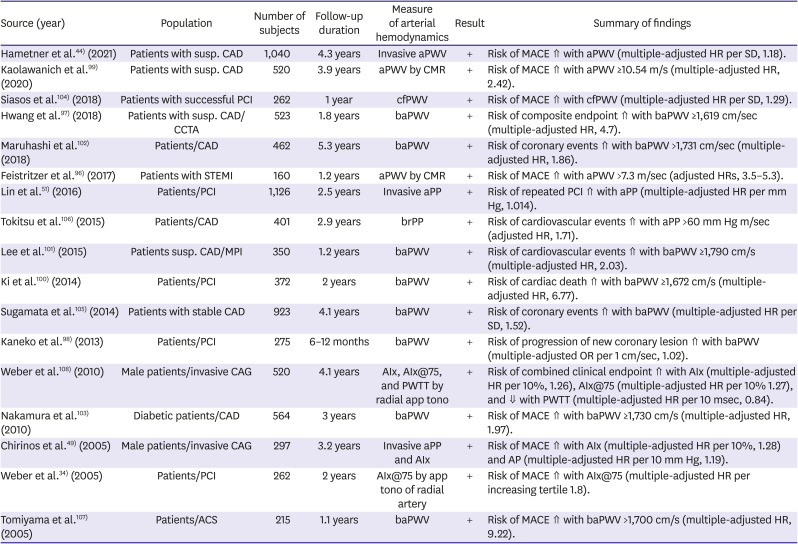
Table 2
Summary of studies showing the prognostic value of arterial pulsatile hemodynamics in patients with CAD
| Source (year) | Population | Number of subjects | Follow-up duration | Measure of arterial hemodynamics | Result | Summary of findings |
|---|---|---|---|---|---|---|
| Hametner et al.44) (2021) | Patients with susp. CAD | 1,040 | 4.3 years | Invasive aPWV | + | Risk of MACE ⇑ with aPWV (multiple-adjusted HR per SD, 1.18). |
| Kaolawanich et al.99) (2020) | Patients with susp. CAD | 520 | 3.9 years | aPWV by CMR | + | Risk of MACE ⇑ with aPWV ≥10.54 m/s (multiple-adjusted HR, 2.42). |
| Siasos et al.104) (2018) | Patients with successful PCI | 262 | 1 year | cfPWV | + | Risk of MACE ⇑ with cfPWV (multiple-adjusted HR per SD, 1.29). |
| Hwang et al.97) (2018) | Patients with susp. CAD/CCTA | 523 | 1.8 years | baPWV | + | Risk of composite endpoint ⇑ with baPWV ≥1,619 cm/sec (multiple-adjusted HR, 4.7). |
| Maruhashi et al.102) (2018) | Patients/CAD | 462 | 5.3 years | baPWV | + | Risk of coronary events ⇑ with baPWV >1,731 cm/sec (multiple-adjusted HR, 1.86). |
| Feistritzer et al.96) (2017) | Patients with STEMI | 160 | 1.2 years | aPWV by CMR | + | Risk of MACE ⇑ with aPWV >7.3 m/sec (adjusted HRs, 3.5–5.3). |
| Lin et al.51) (2016) | Patients/PCI | 1,126 | 2.5 years | Invasive aPP | + | Risk of repeated PCI ⇑ with aPP (multiple-adjusted HR per mm Hg, 1.014). |
| Tokitsu et al.106) (2015) | Patients/CAD | 401 | 2.9 years | brPP | + | Risk of cardiovascular events ⇑ with aPP >60 mm Hg m/sec (adjusted HR, 1.71). |
| Lee et al.101) (2015) | Patients susp. CAD/MPI | 350 | 1.2 years | baPWV | + | Risk of cardiovascular events ⇑ with baPWV ≥1,790 cm/s (multiple-adjusted HR, 2.03). |
| Ki et al.100) (2014) | Patients/PCI | 372 | 2 years | baPWV | + | Risk of cardiac death ⇑ with baPWV ≥1,672 cm/s (multiple-adjusted HR, 6.77). |
| Sugamata et al.105) (2014) | Patients with stable CAD | 923 | 4.1 years | baPWV | + | Risk of coronary events ⇑ with baPWV (multiple-adjusted HR per SD, 1.52). |
| Kaneko et al.98) (2013) | Patients/PCI | 275 | 6–12 months | baPWV | + | Risk of progression of new coronary lesion ⇑ with baPWV (multiple-adjusted OR per 1 cm/sec, 1.02). |
| Weber et al.108) (2010) | Male patients/invasive CAG | 520 | 4.1 years | AIx, AIx@75, and PWTT by radial app tono | + | Risk of combined clinical endpoint ⇑ with AIx (multiple-adjusted HR per 10%, 1.26), AIx@75 (multiple-adjusted HR per 10% 1.27), and ⇓ with PWTT (multiple-adjusted HR per 10 msec, 0.84). |
| Nakamura et al.103) (2010) | Diabetic patients/CAD | 564 | 3 years | baPWV | + | Risk of MACE ⇑ with baPWV ≥1,730 cm/s (multiple-adjusted HR, 1.97). |
| Chirinos et al.49) (2005) | Male patients/invasive CAG | 297 | 3.2 years | Invasive aPP and AIx | + | Risk of MACE ⇑ with AIx (multiple-adjusted HR per 10%, 1.28) and AP (multiple-adjusted HR per 10 mm Hg, 1.19). |
| Weber et al.34) (2005) | Patients/PCI | 262 | 2 years | AIx@75 by app tono of radial artery | + | Risk of MACE ⇑ with AIx@75 (multiple-adjusted HR per increasing tertile 1.8). |
| Tomiyama et al.107) (2005) | Patients/ACS | 215 | 1.1 years | baPWV | + | Risk of MACE ⇑ with baPWV >1,700 cm/s (multiple-adjusted HR, 9.22). |
ACS = acute coronary syndrome; AIx = augmentation index; AIx@75 = AIx corrected by heart rate 75 bpm; aPP = aortic pulse pressure; app tono = applanation tonometry; aPWV = aortic pulse wave velocity; baPWV = brachial-ankle pulse wave velocity; brPP = brachial pulse pressure; CAD = coronary artery disease; CAG = coronary angiography; CCTA = coronary computed tomography angiography; cfPWV = carotid-femoral pulse wave velocity; CI = confidence interval; CMR = cardiac magnetic resonance imaging; CTA = computed tomography angiography; HR = hazard ratio; MACE = major adverse cardiovascular event; MPI = myocardial perfusion imaging; OR = odds ratio; PCI = percutaneous coronary intervention; PWTT = pulse wave transit time; SD = standard deviation; STEMI = ST-elevation myocardial infarction; susp. = suspected.
![]()
Go to :
THERAPEUTIC CONSIDERATIONS
Since the measures of arterial pulsatile hemodynamics are closely related to the occurrence of cardiovascular events, efforts to find ways to improve arterial elastic properties have continued (examples are given in Table 3). The association between weight gain and arterial stiffness, as well as between weight loss and arterial stiffness regression has been suggested in healthy young adults.109) Also, improved aortic distensibility by weight reduction after bariatric surgery in obese patients has been reported.110) Exercise training has been suggested as an another effective way to improve arterial stiffness in healthy individuals,111) hypertensives,112) and in patients with CAD.113) The beneficial effect of exercise training on arterial stiffness may be additive to the effect of medication in CAD patients.113) Arterial stiffness is increased in smokers,114) and smoking cessation decreases arterial stiffness.115)116)117) Therefore, healthy lifestyle habits such as weight loss, exercise, and smoking cessation can help reduce arterial stiffness, although there were some studies showing that such lifestyle modifications have little effect on arterial stiffness.118)119)120) Healthy lifestyle therapy is a basic and important treatment method that should be emphasized for the primary and secondary prevention of CAD. In particular, for subjects with high arterial stiffness, these lifestyle modifications should be better followed to lower arterial stiffness and further reduce cardiovascular risk. Although study sample size was small and the results are still inconsistent, several studies have reported that renin-angiotensin system blocker or statin have favorable effects on arterial pulsatile hemodynamics.121)122)123)124) Therefore, the use of these drugs should be actively considered in high-risk patients. Recently, there have been reports that new anti-diabetic drugs known to have protective effects on cardiovascular system (glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter-2 inhibitors) effectively lower arterial stiffness.125)126)127) Additional studies on the effects of these drugs on lowering arterial stiffness should be followed. It has been suggested that continuous positive airway pressure in patients with sleep apnea was associated with a significant improvement in arterial stiffness measured by PWV or AIx.128)
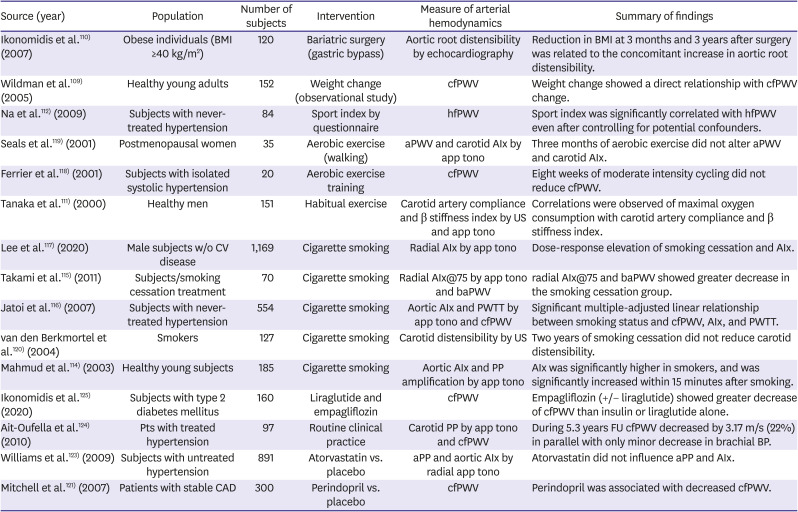
Table 3
Typical examples of studies on methods to improve arterial pulsatile hemodynamics
| Source (year) | Population | Number of subjects | Intervention | Measure of arterial hemodynamics | Summary of findings |
|---|---|---|---|---|---|
| Ikonomidis et al.110) (2007) | Obese individuals (BMI ≥40 kg/m2) | 120 | Bariatric surgery (gastric bypass) | Aortic root distensibility by echocardiography | Reduction in BMI at 3 months and 3 years after surgery was related to the concomitant increase in aortic root distensibility. |
| Wildman et al.109) (2005) | Healthy young adults | 152 | Weight change (observational study) | cfPWV | Weight change showed a direct relationship with cfPWV change. |
| Na et al.112) (2009) | Subjects with never-treated hypertension | 84 | Sport index by questionnaire | hfPWV | Sport index was significantly correlated with hfPWV even after controlling for potential confounders. |
| Seals et al.119) (2001) | Postmenopausal women | 35 | Aerobic exercise (walking) | aPWV and carotid AIx by app tono | Three months of aerobic exercise did not alter aPWV and carotid AIx. |
| Ferrier et al.118) (2001) | Subjects with isolated systolic hypertension | 20 | Aerobic exercise training | cfPWV | Eight weeks of moderate intensity cycling did not reduce cfPWV. |
| Tanaka et al.111) (2000) | Healthy men | 151 | Habitual exercise | Carotid artery compliance and β stiffness index by US and app tono | Correlations were observed of maximal oxygen consumption with carotid artery compliance and β stiffness index. |
| Lee et al.117) (2020) | Male subjects w/o CV disease | 1,169 | Cigarette smoking | Radial AIx by app tono | Dose-response elevation of smoking cessation and AIx. |
| Takami et al.115) (2011) | Subjects/smoking cessation treatment | 70 | Cigarette smoking | Radial AIx@75 by app tono and baPWV | radial AIx@75 and baPWV showed greater decrease in the smoking cessation group. |
| Jatoi et al.116) (2007) | Subjects with never-treated hypertension | 554 | Cigarette smoking | Aortic AIx and PWTT by app tono and cfPWV | Significant multiple-adjusted linear relationship between smoking status and cfPWV, AIx, and PWTT. |
| van den Berkmortel et al.120) (2004) | Smokers | 127 | Cigarette smoking | Carotid distensibility by US | Two years of smoking cessation did not reduce carotid distensibility. |
| Mahmud et al.114) (2003) | Healthy young subjects | 185 | Cigarette smoking | Aortic AIx and PP amplification by app tono | AIx was significantly higher in smokers, and was significantly increased within 15 minutes after smoking. |
| Ikonomidis et al.125) (2020) | Subjects with type 2 diabetes mellitus | 160 | Liraglutide and empagliflozin | cfPWV | Empagliflozin (+/− liraglutide) showed greater decrease of cfPWV than insulin or liraglutide alone. |
| Ait-Oufella et al.124) (2010) | Pts with treated hypertension | 97 | Routine clinical practice | Carotid PP by app tono and cfPWV | During 5.3 years FU cfPWV decreased by 3.17 m/s (22%) in parallel with only minor decrease in brachial BP. |
| Williams et al.123) (2009) | Subjects with untreated hypertension | 891 | Atorvastatin vs. placebo | aPP and aortic AIx by radial app tono | Atorvastatin did not influence aPP and AIx. |
| Mitchell et al.121) (2007) | Patients with stable CAD | 300 | Perindopril vs. placebo | cfPWV | Perindopril was associated with decreased cfPWV. |
AIx = augmentation index; AIx@75 = AIx corrected by heart rate 75 bpm; aPP = aortic pulse pressure; app tono = applanation tonometry; aPWV = aortic pulse wave velocity; baPWV = brachial-ankle pulse wave velocity; BMI = body mass index; BP = blood pressure; CAD = coronary artery disease; cfPWV = carotid-femoral pulse wave velocity; CV = cardiovascular; FU = follow up; hfPWV = heart-femoral pulse wave velocity; PP = pulse pressure; PWTT = pulse wave transit time; SBP = systolic blood pressure; US = ultrasound.
![]()
Go to :
CLINICAL IMPLICATIONS
The onset of atherosclerosis occurs at an early stage and progresses to CAD over a period of decades.129) The speed of progress is determined by the individual risk factor burden of each person. Therefore, it is very effective to identify high-risk individuals for CAD early and implement strong primary preventive strategy. However, risk prediction based on traditional cardiovascular risk factors is limited,3) requiring additional risk prediction tools. Measurements of arterial pulsatile hemodynamics are correlated with the presence and extent of CAD. Also, these measurements are good surrogate markers for future cardiovascular events and mortality in patients with CAD. Since information on arterial pulsatile hemodynamics can be obtained through non-invasive methods, it may be useful in predicting the occurrence of future cardiovascular events in both primary and secondary setting. Also, invasively measured indicators of arterial mechanics such as aPP, aPWV and AIx could predict cardiovascular events, and thus, it is worth considering measuring these parameters during the procedure of invasive CAG. However, we should keep in mind that it is not known to which extent such a strategy influences cardiovascular risk and clinical outcome. In this regard, additional studies should be supported.
Go to :
CONCLUSIONS
Information on arterial pulsatile hemodynamics, such as arterial stiffness and wave reflections, is useful in the estimation of the risk of having coronary atherosclerosis. Also, it provides prognostic information on the development of future cardiovascular events in CAD patients. Noninvasive assessment of arterial pulsatile hemodynamics may be valuable tool in risk stratification. For patients undergoing invasive CAG, measuring pulsatile aortic parameters requires little additional risk, cost, effort, or time, so it may be recommended to measure it during CAG. Further research is needed on whether nonpharmacologic and pharmacologic approaches that have favorable impact on arterial pulsatile hemodynamics improve the patients’ clinical outcome.
Go to :
 XML Download
XML Download