

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite recent improvements in advanced life support, the reported overall survival rate after cardiac arrest remains low.1)2)3) Several observational studies1)4) have demonstrated a low survival rate associated with prolonged cardiopulmonary resuscitation (CPR); this decreased further if the CPR time exceeded 30 minutes. Extracorporeal membrane oxygenation (ECMO) has been suggested as a therapeutic option for refractory cardiac arrest in selected patients with a reversible cause, and this technique has helped to extend the accepted CPR duration.5)6) Previous studies6)7)8)9) have shown better survival rates and good neurological status after extracorporeal cardiopulmonary resuscitation (ECPR) in patients with in-hospital cardiac arrest (IHCA) compared with those who received conventional CPR; the trial numbers of ECPR for cardiac arrest are increasing worldwide every year.7)8)9)
In clinical practice, determining the optimal time when to initiate ECMO and rapid cannulation during chest compressions is difficult, particularly in the emergency department (ED), because of insufficient information regarding the cardiac arrest situation. Accordingly, the Extracorporeal Life Support Organization recommends that ECPR should be performed by a collaborative multidisciplinary team comprising trained specialists.10)11) However, limited data are available on the effect of the approach of a multidisciplinary team that includes an emergency physician on the clinical outcomes of patients who undergo ECPR in the ED; this study aimed to investigate this association.
METHODS
Ethical statement
The study design was approved by the Institutional Review Board of the Samsung Medical Center (approval number: 2019-05-002). The requirement for informed consent was waived owing to the retrospective nature of the study.
Study population
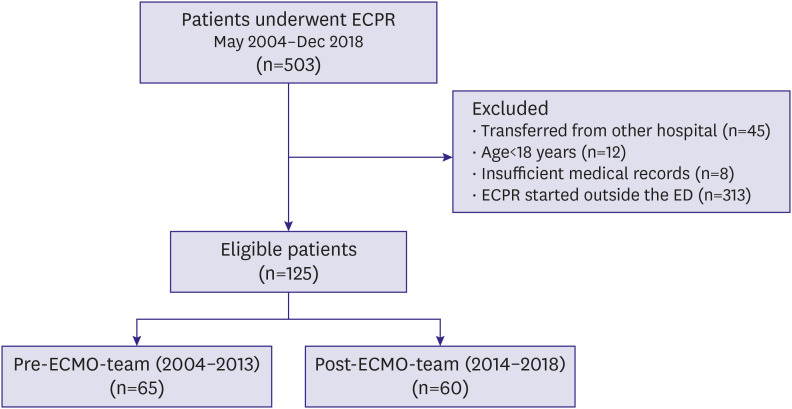
This was a retrospective, single-center, observational study of adult patients who underwent ECPR at the Samsung Medical Center between May 2004 and December 2018. All clinical and laboratory data were collected by a trained study coordinator using a standardized case report form. Additional information was obtained by reviewing electronic medical records. All consecutive patients who underwent ECPR were screened for inclusion in this study. The exclusion criteria were as follows: age of <18 years, transferred from another hospital, insufficient medical records, and started ECPR outside the ED (general ward, operating room, catheterization laboratory, or intensive care unit). Finally, 125 patients were included in this study (Figure 1). In January 2014, a multidisciplinary ECMO team was established at our hospital. This team comprised emergency physicians, interventional cardiologists, critical care physicians, cardiovascular surgeons, heart failure physicians, a pharmacist, a nutritionist, and perfusionists who had previously worked as formal intensive care registered nurses and had received specific ECMO training. Patients were divided into two groups: a pre-ECMO-team group (before January 2014, n=65) and a post-ECMO-team group (after January 2014, n=60).
Procedure and management of ECPR
CPR was led by an emergency physician in the ED, and the decision to call for ECPR was taken by the CPR team leader when CPR was performed for more than 10 minutes or when there was recurrent cardiac arrest. The final decision to initiate ECMO and the cannulation technique was determined collectively by ECMO specialists, such as cardiac surgeons, interventional cardiologists, and emergency physicians. The ECMO cannulation and management flow procedure used at our institution has been described previously.12) A veno-arterial (VA)-ECMO device was inserted by percutaneous cannulation using the Seldinger technique or surgical cannulation using the cut-down method. Size 14–17 French arterial cannulas and size 20–24 French venous cannulas were used. The femoral vessels were usually selected as vascular access sites. The Capiox Emergency Bypass System (Capiox EBS; Terumo, Inc., Tokyo, Japan) and Permanent Life Support (MAQUET GmbH, Rastatt, Germany) were available in our hospital at the time of the study. In the event of distal limb ischemia after arterial cannulation, a catheter was inserted distal to the cannulation site for limb perfusion. When persistent pulmonary edema occurred after ECMO initiation despite the use of diuretics and inotropes, left ventricular decompression was achieved by either percutaneous atrial septostomy or surgical venting. The ECMO-pump speed was adjusted to obtain a cardiac index of >2.2 L/minute/body surface area (m2), a mean arterial pressure of >65 mmHg, and a central mixed venous saturation of >70%. All patients received unfractionated heparin as an anticoagulant unless there was active bleeding. Intravenous heparin was also infused to maintain an activated clotting time ranging from 150–180 seconds or an activated partial thromboplastin time of 55–75 seconds. Before the ECMO team was established, each patient's assigned doctor and cardiology faculty physicians participated in the patient's care, but after the ECMO team was established, the approach by the multidisciplinary ECMO team was applied from the beginning of ECPR in the ED to the patient's hospital discharge. The care included the establishment of treatment protocols, such as the anticoagulation protocol, and by changing of systems, such as by determining the timing of circuit change and preventing mechanical complications through daily ECMO rounding. Furthermore, the multidisciplinary team members regularly discussed weekly cases in quality control meetings. After the patient's admission to the cardiac intensive care unit, there were regular rounds on weekdays (once or twice per day, routinely), and overnight coverage by the in-house general cardiologist who could be contacted by telephone or text messages at anytime of the day. Not only that, one ECMO machine was always primed for emergency ECMO application, minimizing the time required for priming.
Clinical outcomes
The primary outcome was in-hospital mortality. The secondary outcomes were neurological outcomes and procedure-related complications (cannulation site bleeding, limb ischemia, stroke, gastrointestinal bleeding, and procedure-related infections) after ECPR. We evaluated the patients' neurological outcomes using the Cerebral Performance Categories (CPC) scale upon hospital discharge.13) A good neurological outcome was defined as a CPC of 1–2, while a poor neurological outcome was defined as a CPC of 3–5.
Statistical analyses
Categorical variables were compared using the χ2 test or Fisher's exact test, as appropriate, and are presented as numbers and relative frequencies. Continuous variables were compared using Student's t-test or the Wilcoxon rank-sum test, as appropriate, and are presented as means±standard deviation or medians and interquartile ranges (IQRs). The risk of in-hospital mortality was determined using a logistic regression analysis and is presented as odds ratios (ORs) and 95% confidence intervals (CIs). To identify independent predictors of in-hospital mortality, a multivariable logistic regression analysis was performed. Variables were included in the analysis if they showed an association in the univariate analysis with p<0.2 or were considered clinically relevant. All probability values were 2-sided, and p<0.05 was considered statistically significant. Statistical analyses were performed using R Statistical Software (version 3.5.2; R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Patient characteristics
We analyzed 125 consecutive patients who underwent ECPR in the ED during the study period. Among them, 65 underwent ECPR before a multidisciplinary ECMO team was constituted, while the remaining 60 were treated after its formation. The baseline characteristics and laboratory findings of the study participants are shown in Table 1 and Supplementary Table 1, and they were comparable, except that, patients in the post-ECMO-team group were more likely to be younger. In addition, cardiac arrest characteristics and ECMO management data are presented in Table 2. Out-of-hospital cardiac arrest (OHCA), bystander-performed CPR, defibrillation, and pre-arrest rhythms were similar between the two groups. However, the number of witnessed cardiac arrests was higher in the post-ECMO-team group (86.2% vs. 98.3%, respectively; p=0.012).
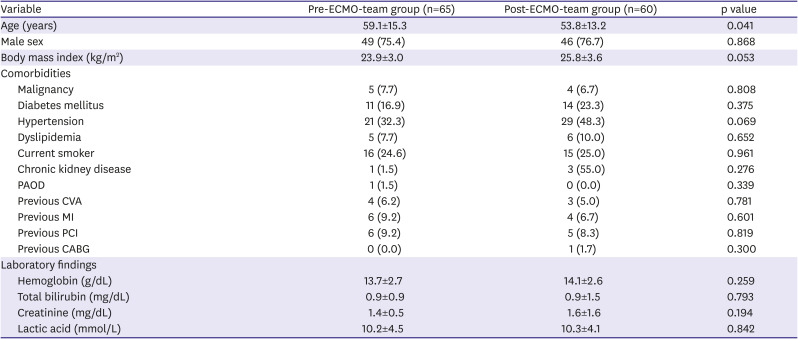
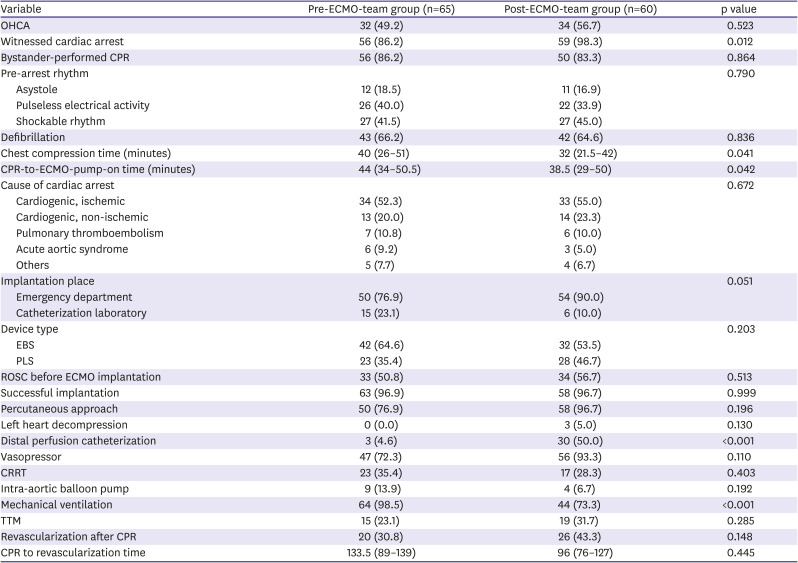
Table 1
Baseline characteristics of patients and laboratory findings
Values are presented as means±standard deviation or number (%).
CABG = coronary artery bypass surgery; CVA = cerebrovascular accident; ECMO = extracorporeal membrane oxygenation; MI = myocardial infarction; PAOD = peripheral arterial occlusive disease; PCI = percutaneous coronary intervention.
![]()
Table 2
Cardiac arrest characteristics and in-hospital management
Values are presented as means (interquartile ranges) or number (%).
CPR = cardiopulmonary resuscitation; CRRT = continuous renal replacement therapy; EBS = emergency bypass system; ECMO = extracorporeal membrane oxygenation; ECPR = extracorporeal cardiopulmonary resuscitation; OHCA = out-of-hospital cardiac arrest; PCI = percutaneous coronary intervention; PLS = permanent life support; ROSC = return of spontaneous circulation; TTM = therapeutic temperature management.
![]()
The most common causes of cardiac arrest were cardiogenic, and there was no significant difference between the two groups regarding the causes of cardiac arrest. Considering hospital management, the insertion of distal perfusion catheters increased after the formation of a multidisciplinary ECMO team (pre-ECMO-team group vs. post-ECMO-team group) (4.6% vs. 51.7%, respectively; p<0.001), while the use of mechanical ventilation decreased (98.5% vs. 73.3%, respectively; p<0.001). The chest compression time (median, 40 [IQR, 26–51] vs. 32 [IQR, 21.5–42] minutes; p=0.041) and CPR-to-ECMO-pump-on time (median, 44 [IQR, 34–50.5] vs. 38.5 [IQR, 29–50] minutes; p=0.042) were shorter for patients who underwent ECPR after the formation of a multidisciplinary ECMO team (Table 2 and Supplementary Table 2).
Among the 65 OHCA patients, 32 underwent ECPR before the formation of a multidisciplinary ECMO team, while the remaining 33 were treated after its formation. The CPR-to-ECMO-pump-on time (median, 52 [IQR, 42.75–29.5] vs. 45 [IQR, 37–59] minutes; p=0.058) was shorter for patients who underwent ECPR after a multidisciplinary ECMO team was formed; however, the arrest-to-ED-arrival time (median, 20.5 [IQR, 14–26] vs. 23 [IQR, 14–30] minutes; p=0.284) did not differ significantly between the 2 groups.
Clinical outcomes
The overall clinical outcomes are shown in Table 3, Supplementary Table 3, and Supplementary Figure 1. In the study period, patients who underwent ECPR after the formation of a multidisciplinary ECMO team had a lower in-hospital mortality rate than those who underwent ECPR before its formation; however, the difference was not statistically significant (72.3% vs. 58.3%, respectively; p=0.102). There was no significant difference between the neurological outcomes at hospital discharge between the pre-ECMO-team and the post-ECMO-team groups, although fewer patients had a poor neurological outcome (CPC 3–5) in the post-ECMO-team group (78.5% vs. 68.3%; p=0.283). Furthermore, there were no significant differences in cannulation failure and procedure-related complications, including cannulation site bleeding, limb ischemia, stroke, gastrointestinal bleeding, procedure-related infections, and rhabdomyolysis, after ECPR between the 2 groups. In OHCA patients, the difference in the rates of in-hospital mortality (68.8% vs. 72.7%; p=0.729) and poor neurological outcomes at hospital discharge (78.1% vs. 84.8%; p=0.302) were not statistically significant between the 2 groups. However, in IHCA patients, in-hospital mortality (75.8% vs. 40.7%; p=0.006) and poor neurological outcomes (CPC 3–5) at hospital discharge (78.8% vs. 48.1%; p=0.015) were significantly lower in the post-ECMO-team group (Figure 2).
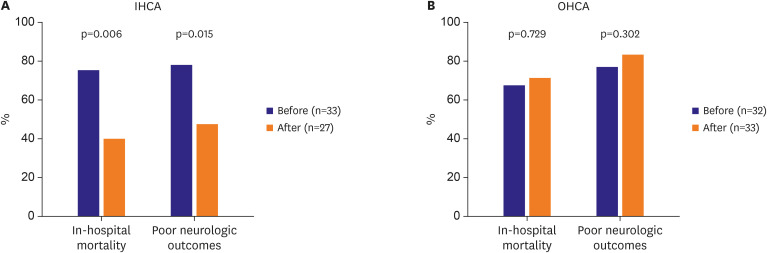
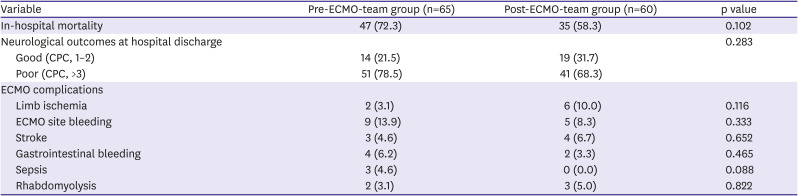
Figure 2
In-hospital mortality and poor neurological outcomes in the pre- and post-ECMO-team groups. A multidisciplinary team approach was associated with improved clinical outcomes in (A) IHCA patients, but not in (B) OHCA patients.
ECMO = extracorporeal membrane oxygenation; IHCA = in-hospital cardiac arrest; OHCA = out-of-hospital cardiac arrest.
![]()
Table 3
Clinical outcomes
![]()
Factors associated with in-hospital mortality
The univariate and multivariable logistic regression analyses of factors associated with in-hospital mortality in all populations and IHCA patients are presented in Table 4. In all populations, the factor associated with increased odds of in-hospital mortality was age (adjusted OR, 1.05; 95% CI, 1.01–1.09; p=0.005) and the factor associated with decreased odds of in-hospital mortality was IHCA (adjusted OR, 0.38; 95% CI, 0.16–0.89; p=0.025). The presence of a multidisciplinary ECMO team did not show statistical significance for in-hospital mortality in all populations. However, in IHCA patients, a multidisciplinary ECMO team decreased the odds of in-hospital mortality (adjusted OR, 0.20; 95% CI, 0.06–0.74; p=0.016).

Table 4
Factors associated with in-hospital mortality in all populations and in IHCA patients
CPR = cardiopulmonary resuscitation; ECMO = extracorporeal membrane oxygenation; IHCA = in-hospital cardiac arrest; OR = odds ratio; PCI = percutaneous coronary intervention.
*Adjusted covariates included age, pre-arrest rhythm, in-hospital cardiac arrest, successful PCI, cause of cardiac arrest, and a multidisciplinary ECMO team approach in all populations; †Adjusted covariates included age, pre-arrest rhythm, successful PCI, cause of cardiac arrest, and a multidisciplinary ECMO team approach in IHCA patients.
![]()
DISCUSSION
In the present study, we investigated the association of a multidisciplinary ECMO team approach with clinical outcomes in patients who underwent ECPR in the ED. In general, there was no significant difference in the in-hospital mortality rates and poor neurological outcomes between the pre- and post-ECMO-team groups; however, in IHCA patients, these parameters were significantly lower in the post-ECMO-team group than in the pre-ECMO-team group. Furthermore, among IHCA patients, a multidisciplinary ECMO team approach was an independent prognostic factor for in-hospital mortality.
After the formation of a multidisciplinary ECMO team, there were major changes in the resuscitation strategy employed for cardiac arrest patients. First, the chest compression time and CPR-to-ECMO-pump-on time were significantly shortened. Several previous studies14)15)16) have shown that no-flow and low-flow times are the most important predictors of overall clinical outcomes after ECPR along with age, initial shockable rhythm, cardiac arrest etiology, lactate and creatinine levels, and Sequential Organ Failure Assessment score. Among them, a low-flow time represented by the CPR-to-ECMO-pump-on time is a unique, modifiable prognostic factor. In our study, the no-flow or low-flow time might have been shorter because of the quick decision-making process regarding ECMO initiation during CPR in the ED. Furthermore, the multidisciplinary team included emergency physicians who regularly participated in weekly quality control meetings. This has greatly contributed to reduce the time to ECMO pump on by emergency physicians acting as an assistant in the procedures. Especially, by changing the protocol to that requiring mandatory calling of the ECMO team whenever CPR was performed for longer than 10 minutes or when there was recurrent cardiac arrest; has helped to save time. In addition, consultation with multidisciplinary teams on patients with ECPR indication at an early stage reduced the ED arrival time of the cardiac surgeon or interventional cardiologists. Second, before the formation of a multidisciplinary ECMO team, some ECPR patients were transferred to the catheterization laboratory for fluoroscopy-guided cannulation while undergoing chest compressions. Conversely, more recently, ECPR patients undergo cannulation for ECMO in the ED. This method allows for safe cannulation with proper detection of the wire position by an emergency physician using bedside ultrasound guidance and may also result in shorter CPR-to-ECMO-pump-on times, because patients need not be moved. Moreover, the frequency of percutaneous approach and distal perfusion catheter insertion were increased numerically after multidisciplinary team foundation. These changes were thought to have contributed to the reduction of CPR-to-ECMO-pump-on time. Third, the number of patients who could breathe spontaneously without the aid of mechanical ventilation during VA-ECMO increased in the post-ECMO-team group. This has some benefits; it helps to prevent ventilator-induced diaphragm dysfunction and ventilator-/intubation-associated pneumonia, reduces delirium, and facilitates improved rehabilitation and interaction with medical staff.17) Recently, this strategy has been attempted in patients undergoing high-risk percutaneous coronary intervention, those suffering from refractory cardiogenic shock, and those awaiting organ transplantation, and has resulted in improved clinical outcomes.17)18)19)20)21) Fourth, there are precise criteria for the selection of candidates for ECPR currently. In this study, the rate of witnessed cardiac arrests was higher in the post-ECMO-team group; only 1 patient with unwitnessed cardiac arrest was present in this group, and this patient also received CPR within 10 minutes of the cardiac arrest. Both improved ECPR quality and strict criteria for patient selection might have improved the clinical outcomes in IHCA patients after the formation of a multidisciplinary ECMO team.
However, in this study, clinical outcomes were not improved in OHCA patients, even after the formation of a multidisciplinary ECMO team. Several studies22)23)24) have suggested that a longer prehospital duration of resuscitation is associated with poor outcomes. According to resuscitation guidelines and expert opinion, the ideal therapeutic window for ECPR is within 60 minutes of cardiac arrest.25)26)27) Therefore, we selected a prehospital low-flow time of <30 minutes as a criterion for eligibility so as not to exceed the 60-minute duration from patient collapse to ECMO-pump-on time. We could adhere to this time limit in almost all cases after a multidisciplinary ECMO team was established. The median CPR-to-ECMO-pump-on time decreased after the formation of a multidisciplinary ECMO team; however, the median time that elapsed between cardiac arrest and arrival at the ED did not change significantly. This could be the main reason why there were no change in the clinical outcomes of OHCA patients, even after the formation of a multidisciplinary ECMO team. The number of emergency medical service practitioners and their experience has remained limited to date and is often insufficient during prehospital resuscitation. Accordingly, clinical outcomes may improve with reduced prehospital resuscitation times and improvement in the quality of prehospital management of ECPR patients.
This study has several limitations. First, it was conducted as a retrospective cohort study; hence, there is always the possibility of selection bias influencing the significance of our findings. This is particularly true for the CPC score used as a measure of neurological outcomes that was determined from patient medical records. By using 2 independent specialists' agreement on the score, any bias may have been ameliorated to some extent. Second, this was a single-center study, which may limit the generalizability of our results and produce a selection bias of the patient subset. Additionally, the relatively small sample size, because of the strict indications for ECPR, could have resulted in limited precision of the estimates. Nevertheless, this study is meaningful in that it is the first to evaluate the effect of a multidisciplinary team approach on the clinical outcomes of patients undergoing ECPR in the ED. Finally, this analysis was performed as a before-and-after study, over a long period, at a single center, which could have influenced the study results. Especially, the advances in the treatment of shock patients or accumulation of experiences over time may have served as potential bias in the study. Considering the long duration of this study, this may affect the study results.28) Recently, the ELSO registry has shown improved outcomes in patients supported with ECMO over time, which may be attributed to the accumulation of experience.29) However, except for the post-arrest management and a multidisciplinary team approach change, there were no significant systemic changes, such as in the resuscitation methods and equipment in the ED, during the study period.
In conclusion, a multidisciplinary ECMO team approach was associated with improved clinical outcomes in IHCA patients who underwent ECPR in the ED, but not in patients with OHCA. These findings could aid in improving the selection criteria for ECPR in the ED, and further studies to overcome the study limitations may also help to improve the outcomes of OHCA patients.
 XML Download
XML Download